
Abstract
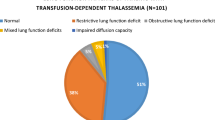
To study pulmonary function tests (PFT) in multiple transfusion recipient thalassemics, PFTs were done for 30 thalassemics and 20 matched controls. Confirmed cases of thalassemia on regular transfusion therapy were the subject of study. Apart from history and physical examination of the thalassemics, serum ferritin estimation and spirometry were done. Parameters studied included lung volumes—functional residual capacity (FRC), forced vital capacity (FVC), residual volume (RV) and total lung capacity (TLC); and flow rates —forced expiratory volume in one second (FEV,), forced expiratory volume in 1 second/forced vital capacity (FEV,/FVC), peak expiratory flow 25–75 (PEF 25–75%) and peak expiratory flow rate (PEFR). Single breath carbon monoxide diffusing capacity (DLco) and arterial blood gas (ABG) were also analysed. The mean height and weight of thalassemics were below that of age matched controls. A restrictive abnormality in PFT was found in 86.6% cases. These patients were found to have a decrease in all the lung volumes namely FVC, FRC, RV and TLC with a proportional decrease in the flow rates, FEV1, PEF 25–75% and PEF with a normal (> 0.75) FEV1/FVC ratio. DLco was decreased in all the patients with restrictive lung disease and fall in DLco showed a good correlation (r = 0.7, P <. 001) with the severity of restrictive disease suggesting that some intrapulmonary pathology is likely to be responsible for the restrictive pattern. None of the cases had an obstructive or mixed pattern of pulmonary dysfunction. No correlation was found between severity of restrictive disease and the serum ferritin levels. A negative correlation with degree of hepatosplenomegaly was found. No correlation was found between severity of the defect and age, number of blood transfusions received and hemoglobin at the time of doing the test. To conclude, restrictive lung disease is the predominant abnormality in multi-transfused thalassemics, which is probably due to pulmonary parenchymal pathology. The abnormality of PFTs is not directly related to iron overload.
Similar content being viewed by others

References
Kattami CA, Kattami AC. Management of thalassemia: Growth and Development, Vitamin supplementation and vaccination.Seminars Hematol 1995; 32: 269–279.
Zurlo MF, Destefano P, Borgna-Pignatti C et al. Survival and causes of death in thalassemia major.Lancet 1989; 2: 27–30.
Gaba A, D’Souza P, Chandra J, Narayan S, Sen S. Ocular changes in b thalassemia.Ann Ophthalm Glaucoma 1998; 30: 357–360.
Keens TG, Oneal MH, Ortega JA, Hymom CB, Platzkey AG. Pulmonary function abnormalities in thalassemia patients on a hypertransfusion programme.Pediatr 1980; 65: 1013–1017.
Cooper DM, Mansel AL, Weiner MA et al. Low lung capacity and hypoxemia in children with thalassemia major.Amer Rev Resp Dis 1980; 121: 639–646.
Hoyt RW, Nina S, Wilmott RW, Cohen A, Schwartz E. Pulmonary function abnormalities in homozygous b thalassemia.J Pediatr 1986; 109: 452–455.
Fung KP, Wun Chow OK, Yeungso S, Yuen PMP. Pulmonary function in thalassemia major.J Pediatr 1987; 111: 534–537.
Pfaff JK, Morgan WJ. Pulmonary function in infants and children.Pediatr Clin N Amer 1994; 41: 401–423.
Wall MA. Office pulmonary function testing.Pediatr Clin N Amer 1984; 31: 773–783.
Grisaru D, Rachmilewitz EA, Mosseri M et al. Cardio-pulmonary assessment in beta-thalassemia major.Chest 1990; 98:1138–1142.
Factor JM, Pottipati SR, Rappaport I, Rasner IK, Lesser ML, Giardina PJ. Pulmonary function abnormalities in thalassemia and the role of iron overload.Amer J Resp Crit Care Mod 1994; 149:1570–1574.
Luyt DK, Roode H, Dowdeswell RJ, vanRensberg AJ, Reinach SG. Thalassemia: Lung function studies with reference to iron studies and reactive oxidant status.Pediatr Hematol Oncol 1993; 10 :13–23.
Youngchaiyud P, Suthamsmai T, Fucharoen S et al. Lung function tests in splenectomised â thalassemia/ HbE patients.Birth Defects. 1988; 23: 361–370.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arora, M., Chandra, J., Suri, J.C. et al. Pulmonary function tests in beta thalassemia. Indian J Pediatr 68, 239–242 (2001). https://doi.org/10.1007/BF02723198
Issue Date:
DOI: https://doi.org/10.1007/BF02723198