
Background:
There is insufficient evidence to suggest the routine use of postmastectomy radiotherapy (PMRT) in patients with one to three positive axillary nodes and T1/2 tumors. We have assessed the risk of locoregional recurrence (LRR) with or without RT in this group of patients, and focused on the results in subgroups defined by tumor size.
Patients and Methods: 249 women with T1/2 tumors and one to three positive nodes underwent mastectomy and axillary dissection between 1983 and 1987. Locoregional RT of 50 Gy was given to 175 patients. Chemotherapy or hormonal therapy was administered to 41 and 71 women, respectively. The median follow-up time of survivors was 189 months (range, 167–227 months).
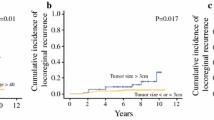
Results: The rates of isolated LRR without or with RT were 16% (12/74) and 8% (14/175), respectively (p = 0.05), and the total (with or without distant relapse) LRR rates 23% and 12%, respectively (p = 0.03). 15-year overall survival amounted to 41% without RT and to 52% with RT (p = 0.2). The rates of isolated LRR for patients treated with chemotherapy or hormonal therapy only were 25% and 12%, respectively. In the absence of RT, age (> 45 vs = 45 years; p = 0.06), tumor size (T1 vs T2; p = 0.07), and extranodal invasion (ENI; absent vs present; p = 0.09) were related to the risk of developing an isolated LRR. On multivariate analysis, only tumor size (relative risk [RR], 3.92; 95% confidence interval [CI], 1.11–15.14) and age (RR, 3.37; 95% CI, 1.03–11.09) emerged as independent significant predictors, whereas ENI (RR, 1.50; 95% CI, 0.81–2.77) did not. In the T1 subgroup, the estimated 15-year isolated LRR rate was 9% (3/36) without and 9% (8/99) with RT (p = 0.9775). 15-year disease-free survival amounted to 62% and 57%, respectively (p = 0.5153). For patients without RT, according to the age groups (= 45 vs > 45 years), the 15-year rates of isolated LRR were 9% and 9%, respectively (p = 0.9910). In the T2 subgroup, the estimated 15-year isolated LRR rate was 30% (9/38) without and 10% (6/76) with RT (RR, 0.33; 95% CI, 0.12–0.92; p = 0.0244). 15-year disease-free survival amounted to 32% and 50%, respectively (p = 0.1213). For patients without RT, according to the age groups (≤ 45 vs > 45 years), the 15-year rates of isolated LRR were 57% and 16%, respectively (p = 0.0049).
Conclusion: Patients with T1 tumor and one to three positive nodes are at low risk of isolated LRR either with or without RT. Patients with T2 tumor and one to three positive nodes are at high risk of isolated LRR without RT. Our findings support the routine use of PMRT in patients with T2 tumor, especially those aged ≤ 45 years.
Hintergrund:
Es gibt nicht genügend Hinweise darauf, ob eine adjuvante Strahlentherapie nach Mastektomie bei Patientinnen mit kleinen Tumoren (T1/2) und ein bis drei positiven axillären Lymphknoten indiziert ist. Wir haben das Risiko, lokoregionäre Rezidive (LRR) zu entwickeln, bei dieser Gruppe mit oder ohne Radiotherapie (RT) untersucht und insbesondere die Untergruppen analysiert, die aus der Größe des Primärtumors gebildet wurden.
Patienten und Methodik: Von 1983 bis 1987 führten wir bei 249 Patientinnen mit T1/2-Karzinomen der Brust und ein bis drei positiven axillären Lymphknoten eine Mastektomie und Dissektion der Axilla durch. Bei 175 Patientinnen folgte eine adjuvante lokoregionale Strahlenbehandlung mit 50 Gy. Die Nachbeobachtungszeit lag zwischen 167 und 227 Monaten, im Median bei 189 Monaten.
Ergebnisse: Von 249 Patientinnen entwickelten zwölf (16%) ohne RT (n = 74) und 14 (8%) mit RT (n = 175) ein isoliertes LRR (p = 0,05). Im Gesamtkollektiv entstanden LRR bei 23% ohne RT und bei 12% mit RT (p = 0,03). Folgende Rezidivlokalisationen wurden beobachtet: Brustwand 17 (65%), Achselhöhle fünf (19%), Supraklavikulargrube drei (12%) und parasternale Lymphknoten eine (4%). Die 15-Jahres-Gesamtüberlebensrate betrug 52% für Patientinnen mit vs. 41% ohne Strahlenbehandlung (p = 0,2). In der Subgruppe der pT1-Tumoren lag die Rate an isolierten LRR bei 9% (3/36) ohne RT vs. 9% (8/99) mit RT (p = 0,9775). Die krankheitsfreie 15-Jahres-Überlebensrate betrug 62% für Patientinnen ohne RT vs. 57% mit RT (p = 0,5153). In der Subgruppe der pT2-Tumoren lag die Rate an isolierten LRR bei 30% (9/38) ohne versus 10% (6/76) mit RT (relatives Risiko 0,33; 95%-Vertrauensintervall 0,12–0,92; p = 0,0244). Die krankheitsfreie 15-Jahres-Überlebensrate betrug 32% für Patientinnen ohne vs. 50% mit RT (p = 0,1213).
Schlussfolgerung: Patientinnen mit T1-Tumoren und ein bis drei axillären Lymphknotenmetastasen weisen insgesamt ein niedriges Risiko auf, ein isolierte LRR zu entwickeln. Patientinnen mit T2-Tumoren und ein bis drei axillären Lymphknotenmetastasen haben dagegen ein hohes Risiko für die Entwicklung eines LRR mit oder ohne adjuvante Strahlenbehandlung, jedoch signifikant niedriger in der Gruppe mit RT. Aufgrund unserer langjährigen Erfahrungen und der Ergebnisse dieser retrospektiven Auswertung empfehlen wir die adjuvante Strahlenbehandlung für Tumorgrößen ab pT2 mit ein bis drei Lymphknotenmetastasen, nicht jedoch für pT1.
Similar content being viewed by others


Author information
Authors and Affiliations
Additional information
Received: February 21, 2002; accepted: August 2, 2002
Correspondence Address János Fodor, MD PhD, Department of Radiotherapy, National Institute of Oncology, Ráth Gy. u. 7–9, 1122-Budapest, Hungary, Phone (+36/1) 2248-600, Fax -620, e-mail: fodor@oncol.hu
Rights and permissions
About this article
Cite this article
Fodor, J., Polgár, C., Major, T. et al. Locoregional Failure 15 Years after Mastectomy in Women with One to Three Positive Axillary Nodes with or without Irradiation . Strahlenther Onkol 179, 197–202 (2003). https://doi.org/10.1007/s00066-003-1010-7
Issue Date:
DOI: https://doi.org/10.1007/s00066-003-1010-7