
Abstract
Purpose
The treatment of trauma patients requires significant hospital resources. Numerous protocols exist to triage the injured patient and determine the level of care they may require. The purpose of this work is to describe an institutional trauma nurse screening procedure and to evaluate its effectiveness in triaging injured patients.
Methods
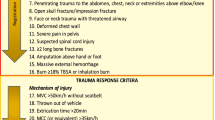
This retrospective study was conducted at a large, tertiary trauma center from January to June 2021. Patients were assessed by trauma nurse clinicians (TNC) utilizing a standardized screening process to determine suitability for trauma activation. If the patient did not meet activation criteria, they were sent to the main Emergency Department for evaluation and treatment. Patients could be activated later by the emergency physician. The primary variables of interest were number of activations after initial “rule out,” injury severity score (ISS) for patients who were activated, mechanism of injury, and disposition.
Results
A total of 1874 TNC screenings were performed. Of these, 1449 (77%) patients did not meet trauma activation criteria. Only 41 (2.8%) patients initially ruled out were later activated by the emergency physician and admitted for treatment of injuries. The average ISS of all activated patients was 9 ± 6. Thirty-six patients had an ISS ≤ 15, four between 16 and 25, and only one patient had an ISS > 25. Twenty-seven patients were admitted to the ward, five went to step-down units, and five required intensive care unit admission. Four patients required operative intervention for their injuries.
Conclusion
These results suggest that nursing screening protocols can be safe, effective tools for triage of trauma patients.

Similar content being viewed by others


References
MacKenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Frey KP, Egleston BL, et al. The national study on costs and outcomes of trauma. J Trauma Acute Care Surg. 2007;63(6):S54–67.
Morris RS, Karam BS, Murphy PB, Jenkins P, Milia DJ, Hemmila MR, et al. Field-triage, hospital-triage and triage-assessment: a literature review of the current phases of adult trauma triage. J Trauma Acute Care Surg. 2021;90(6):e138–45.
Jeppesen E, Cuevas-Østrem M, Gram-Knutsen C, Uleberg O. Undertriage in trauma: an ignored quality indicator? Scand J Trauma Resusc Emerg Med. 2020;28(1):1–3.
Schellenberg M, Benjamin E, Bardes JM, Inaba K, Demetriades D. Undertriaged trauma patients: who are we missing? J Trauma Acute Care Surg. 2019;87(4):865–9.
Tignanelli CJ, Vander Kolk WE, Mikhail JN, Delano MJ, Hemmila MR. Noncompliance with American College of Surgeons Committee on Trauma recommended criteria for full trauma team activation is associated with undertriage deaths. J Trauma Acute Care Surg. 2018;84(2):287–94.
Ghazali SA, Abdullah KL, Moy FM, Ahmad R, Hussin EOD. The impact of adult trauma triage training on decision-making skills and accuracy of triage decision at emergency departments in Malaysia: A randomized control trial. Int Emerg Nurs. 2020;51: 100889.
Gyang E, Shieh L, Forsey L, Maggio P. A nurse-driven screening tool for the early identification of sepsis in an intermediate care unit setting. J Hosp Med. 2015;10(2):97–103.
Hegazy SM, Elsayed LA, Ahmed TY, Rady MI. Avoiding pitfalls in trauma triage: effect of nursing staff development. Life Sci J. 2012;9(1):1006–14.
Newgard CD, Uribe-Leitz T, Haider AH. Undertriage remains a vexing problem for even the most highly developed trauma systems: the need for innovations in field triage. JAMA Surg. 2018;153(4):328–328.
Kodadek LM, Selvarajah S, Velopulos CG, Haut ER, Haider AH. Undertriage of older trauma patients: is this a national phenomenon? J Surg Res. 2015;199(1):220–9.
Xiang H, Wheeler KK, Groner JI, Shi J, Haley KJ. Undertriage of major trauma patients in the US emergency departments. Am J Emerg Med. 2014;32(9):997–1004.
Roden-Foreman JW, Rapier NR, Yelverton L, Foreman ML. Avoiding Cribari gridlock: the standardized triage assessment tool improves the accuracy of the Cribari matrix method in identifying potential overtriage and undertriage. J Trauma Acute Care Surg. 2018;84(5):718–26.
Hashmi ZG, Haut ER, Efron DT, Salim A, Cornwell EE III, Haider AH. A target to achieve zero preventable trauma deaths through quality improvement. JAMA Surg. 2018;153(7):686–9.
Jones TL, Mims BC, Luecke LE. Two successful models for preparing competent critical care nurses: the Parkland Health and Hospital system critical care and trauma nurse internship and critical care residency. Crit Care Nurs Clin N Am. 2001;13(1):35–52.
Ghaferi AA, Schwartz TA, Pawlik TM. STROBE reporting guidelines for observational studies. JAMA Surg. 2021;156(6):577–8.
Nederpelt CJ, Mokhtari AK, Alser O, Tsiligkaridis T, Roberts J, Cha M, et al. Development of a field artificial intelligence triage tool: confidence in the prediction of shock, transfusion, and definitive surgical therapy in patients with truncal gunshot wounds. J Trauma Acute Care Surg. 2021;90(6):1054–60.
Funding
The authors have no relevant financial or non-financial interests to disclose.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors did not receive support from any organization for the submitted work.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gupta, V.S., Burke, K., Bruns, B.R. et al. Utilization of trauma nurse screening procedure for triage of the injured patient. Eur J Trauma Emerg Surg (2022). https://doi.org/10.1007/s00068-022-02105-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00068-022-02105-8