
Abstract
Using country- and region-level data, I investigate the effect of HIV/AIDS on fertility in Africa during 1985–2000. Results differ depending on the variation used and the estimation method. Between estimates that exploit cross-sectional variation suggest a positive significant effect of HIV/AIDS on fertility, whereas within estimates that are identified of off time-series variation show both positive and negative results depending on the HIV/AIDS variable used. These within estimates are insignificant in most of the specifications.







Similar content being viewed by others

Notes
While most of the researchers find negative effects of the epidemic on economic growth, some find no effect and some even find positive effects. Bloom and Mahal (1997) run cross-country regressions of growth of GDP per capita on HIV/AIDS prevalence and find no effect. Papageorgiou and Stoytcheva (2007) find a negative significant effect of AIDS on income per worker but the effect is small. Werker et al. (2006) instrument HIV/AIDS prevalence by national circumcision rates and show that there is no effect of the epidemic on growth of the African countries. Corrigan et al. (2005) show calibration results that imply large negative effects of the epidemic on growth. The results of Lorentzen et al. (2008) imply significant long-run costs of AIDS on various outcome variables.
Many African studies, both clinic and cohort based, indicate lower fertility (around 40%) and childbearing odds among HIV-positive women. See Lewis (2007) for a recent review of these studies.
It is hard to separate the biological effect from the behavioral response without data on individual HIV status. In Juhn et al. (2008), we take a first step in separating these two effects by utilizing recent rounds of the demographic health surveys (DHS) which link an individual woman’s fertility outcomes to her own HIV status, based on testing.
Mwaluko et al. (2003), Bloom et al. (2000), Stoneburner and Low-Beer (2004), Lagarde et al. (1996), Lindan et al. (1991), Ng’weshemi et al. (1996), Williams et al. (2003) and Caldwell et al. (1999) all find no change or very small change in sexual behavior. Oster (2005), using DHS data on sexual behavior from a subset of African countries finds that sexual behavior changed relatively little since the onset of the epidemic. Other researchers finds some evidence of risky behavior reductions in Zambia and Zimbabwe such as reductions in multiple partners; see Cheluget et al. (2006) and Fylkesnes et al. (2001).
Temmerman et al. (1990) find that in Nairobi a single session of counseling—which is common in most African countries—has no effect on the subsequent reproductive behavior of HIV-positive women. Allen et al. (1993) using cohort data from Kigali, Rwanda, find that in the first 2 years of follow-up after HIV testing, HIV-negative women were more likely to become pregnant than HIV-positive women. However, among HIV-positive women, those with no children were more likely to become pregnant than those with children and married women are more likely to become pregnant than unmarried women. The desire to have children among HIV-positive women altogether was 45%. On the other hand, Noel-Miller (2003) using panel data from Malawi shows that women who have higher subjective HIV risk perceptions for themselves were less likely to have children.
There might also be differences across countries as far as the links between AIDS and mortality and HIV and AIDS are concerned. We use country-specific time trends to partially account for this. A better approach will be country-year dummies which cannot be used given the fact that this is the exact variation we exploit.
I also use data on desired fertility rate per woman ages 15–49, available for 34 countries, from DHS. Details of the variables and a full list of countries and survey years are provided in the Appendix.
See also Durevall and Lindskog (2011).
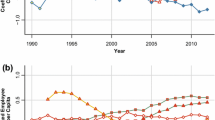
Each countries survey year is on or around the dates shown on the x-axis.
See Juhn et al. (2008) for a comparison of the various estimates.
It chooses a set minimizing least squares and projects future course based on fitted parameters, such as a parameter for the start year of the epidemic; one for the force of infection (how explosive the epidemic is in its initial stage); one for the fraction of new entrants to the population going into to the at-risk category (a parameter largely determines where the epidemic levels off); and one for the recruitment (a high value means people are brought into the at-risk population as people die of HIV, thus helping to sustain the epidemic at a higher level).
I also use data on perceptions, specifically the variable “know someone died of AIDS.” The data on the percent female who know someone personally who has the virus that causes AIDS or has died of AIDS are from DHS. This is the ideal measure for the purpose of this paper however since this question has only been asked in the most recent surveys the data are available only for 22 countries whose survey years fall between 1993 and 2004. The results with this measure are available upon request.
Controlling for these variables in the robustness analysis yielded same results. See also Schultz (1997).
This regressions is also run at the regional level with country dummies included, i.e., for region r: \(\mathit{\rm TFR}_r=\alpha_i + \beta \mathit{\rm HIV/AIDS}_r + {\bf X}'_r \gamma + \epsilon_r\), where α i is the country dummy.
If sexual behavior declines for some other reason than HIV/AIDS, then this will lead a positive association between fertility and the epidemic since both will decline as a result. One cannot rule this out.
In a previous version of the paper, I also undertook an IV exercise, which yielded similar results.
Using other measures of female schooling yield similar results.
See Appendix for details on survey years.
I also used desired fertility from DHS obtaining very similar results and hence I do not report them but they are available upon request.
To deal with zero HIV/AIDS we pursued two different strategies where we dropped the zero observations and we use the HIV as log(1 + HIV). Both of these strategies yielded similar results.
I also perform weighted least squares (WLS) panel regressions; where all observations are weighted in the second step with the inverse of the estimated standard deviations from the first step. Weighting by country’s population or log population yields similar results.
I also experimented with a common non-linear quadratic and cubic trend obtaining similar results.
An alternative story that explain the difference between AIDS and HIV and between and within results might the fact that AIDS is a measure of death and HIV is the current infection. We repeat the time-series specifications including lagged variables and the results stay the same. These exercises are available upon request.
The results with HIV-Oster are similar and available upon request. For robustness, we have also tried many other control variables such as contraception, population age and size, and so on; all of the results remain the same and available upon request.
I also run IV regressions for a smaller sub-sample. In spite of a strong first stage, the second stage regressions gave statistically insignificant results.
Peterson (2009) shows this for the standard OLS regression but he reports that his results generalizes to non-linear models too. Bertrand et al. (2004) focuses on a DD model such as; Y ist = A s + B t + c X ist + βI st + ε ist , for individual i, state s, and time t. They also show simple parametric corrections, such as fitting an AR1 process for the error structure, or non parametric corrections, such as block bootstrap, only works with large number of states/cross-sectional units. They show that clustering at state level not just at state-year cell is the best solution.
Kezdi (2004) shows clustered standard errors can be too large in a fixed effects model but he also shows only clustered standard errors are unbiased irrespective of having a country effect, as also shown by Peterson (2009). Peterson (2009) also shows the generalization of the results for the GLS case. Kezdi (2004) shows that the general robust standard error estimator known as the cluster estimator is not only consistent in general but it behaves well in finite samples. His Monte Carlo simulations shows that only cluster estimator gives unbiased results even in small cross-sectional samples. He shows in a fixed effect model with short time series (as here), serial correlation in the error process and the right hand side variables induce severe bias in conventional standard errors. Clustered estimator applied to mean-differenced data is consistent and behaves well in finite sample and it does not get biased with high T or small N.
References
Allen S, Serufilira A, Gruber V, Kegeles S, Van de Perre P, Carael M, Coates TJ (1993) Pregnancy and contraception use among urban Rwandan women after HIV testing and counseling. Am J Public Health 83(5):705–710
Angeles L (2011) Demographic transitions: analyzing the effects of mortality on fertility. J Popul Econ 23(1):99–120
Becker GS, Barro RJ (1988) A reformulation of the economic theory of fertility. Q J Econ 103(1):1–25
Bertrand M, Duflo E, Mullainathan S (2004) How much should we trust difference in differences estimates? Q J Econ 119(1):249–275
Bloom D, Mahal A (1997) Does the AIDS epidemic threaten economic growth? J Econom 77(1):105–124
Bloom S, Banda C, Songolo G, Mulendema S Cunningham A, Boerma JT (2000) Looking for change in response to the AIDS epidemic: trends in AIDS knowledge and sexual behavior in Zambia, 1990 through 1998. AIDS 25:77–85
Boldrin M, Jones LE (2002) Mortality, fertility, and saving in a Malthusian economy. Rev Econ Dyn 5(4):775–814
Caldwell J, Orubuloyeb IO, Caldwell P (1999) Resistances to behavioural change to reduce HIV/AIDS infection in predominantly heterosexual epidemics in third world countries. Health Transition Center
Cervellati M, Sunde U (2007) Human capital, mortality, and fertility: a unified theory of demographic transition. IZA Working Paper 2905
Cheluget B, Baltazar G, Orege P, Ibrahim M, Marum LH, Stover J (2006) Evidence for population level declines in adult HIV prevalence in Kenya. Sex Transm Infect 82(Supplement 1):121–126
Corrigan P, Gloom G, Mendez F (2005) AIDS crisis and growth. J Dev Econ 77(1):107–124
Durevall D, Lindskog A (2011) Uncovering the impact of the HIV epidemic on fertility in Sub-Saharan Africa: the case of Malawi. J Popul Econ 24(2):629-655
Ehrlich I, Lui FT (1991) Intergenerational trade, longevity, intrafamily transfers and economic growth. J Polit Econ 99(5):1029–1059
Fink G, Linnemayr S (2008) HIV and fertility: long-term evidence from sub-Saharan Africa. Harvard University, mimeo
Fortson J (2009) HIV and fertility. Am Econ J Appl Econ 1(3):170–194
Fylkesnes K, Musonda RM, Sichone M, Ndhlovu Z, Monze M, Tembo F, Phiri S, Malamba C (2001) Declining HIV prevalence and risk behaviors in Zambia: evidence from surveillance and population-based surveys. AIDS 15(7):907–916
Galor O, Weil DN (1999) From Malthusian stagnation to modern growth. Am Econ Rev 89(2):150–154
Juhn C, Kalemli-Ozcan S, Turan B (2008) HIV and fertility in Africa: first evidence from population based surveys. NBER WP 14248
Kalemli-Ozcan S (2002) Does mortality decline promote growth? J Econ Growth 7(4):411–439
Kalemli-Ozcan S, Turan B (2011) HIV and fertility revisited. J Dev Econ (in press)
Kezdi G (2004) Robust standard error estimation in fixed-effects panel models. Hung Stat Rev 9:85–116
Lagarde E, Pison G, Enel C (1996) Knowledge, attitudes and perception of AIDS in rural Senegal: relationship to sexual behaviour and behaviour change. AIDS 10(3):327Ű-334
Lewis J (2007) The population impact of HIV on fertility in sub-Saharan Africa. AIDS 18(2):35–43
Lindan C, Allen S, Carael M, Nsengumuremyi F, Van de Perre P, Serufilira A, Tice J, Black D, Coates T, Hulley S (1991) Knowledge, attitudes, and perceived risk of AIDS among urban Rwandan women: relationship to HIV infection and behavior change. AIDS 5(8):993-Ű1002
Lorentzen P, McMillan J, Wacziarg R (2008) Death and development. J Econ Growth 13(2):81–124
Lucas RE (2002) Lectures on economic growth. Harvard University Press, Cambridge
McNeill D (2007) U.N. to say it overestimated AIDS cases by millions. New York Times
Mwaluko G, Urassa M, Isingo R, Zaba B, Boerma JT (2003) Trends in HIV and sexual behavior in a longitudinal study in a rural population in Tanzania, 1994–2000. AIDS 17:2645–2651
Ng’weshemi JZ, Boerma JT, Pool R, Barongo L, Senkoro K, Maswe M, Isingo R, Schapink D, Nnko S, Borgdorff MW (1996) Changes in male sexual behaviour in response to the AIDS epidemic: evidence from a cohort study in urban Tanzania. AIDS 10(12):1415-Ű1420
Noel-Miller CM (2003) Concern regarding the HIV/AIDS epidemic and individual childbearing, evidence from rural Malawi. Demographic Research. http://www.malawi.pop.upenn.edu/Level%203/Papers/PDF-files/noel-2003.pdf
Oster E (2005) Sexually transmitted infections, sexual behavior, and the HIV/AIDS epidemic. Q J Econ 120(2):467–515
Oster E (2011) Routes of infection: exports and HIV incidence in sub-Saharan Africa. J Eur Econ Assoc (in press)
Papageorgiou C, Stoytcheva P (2007) What do we know about the impact of AIDS on cross-country income so far? LSU, mimeo
Peterson M (2009) Estimating standard errors in finance panel data sets: comparing approaches. Rev Financ Stud 22(1):435–480
Schultz PT (1997) Demand for children in low income countries. In: Rosenzweig MR, Stark O (eds) Handbook of population and family economics. Elsevier, Amsterdam
Soares R (2005) Mortality reductions, educational attainment, and fertility choice. Am Econ Rev 95(3):580–601
Stoneburner R, Low-Beer D (2004) Population-level HIV declines and behavioral risk avoidance in Uganda. Science 304:714-Ű718
Tamura R (2006) Human capital and economic development. J Dev Econ 79(1):26–72
Temmerman M, Moses S, Kiragu D, Fusallah S, Wamola IA, Piot P (1990) Impact of single session post-partum counselling of HIV infected women on their subsequent reproductive behavior. AIDS 2:247–252
Timberg C (2006) How AIDS in Africa was overstated? Washington Post
UNAIDS/WHO (2003) Epidemiological fact sheets
UNAIDS/WHO (2006) Global report
US Census Bureau (2005) HIV surveillance database
Werker E, Ahuja A, Wendell B (2006) Male circumcision and the economic impact of AIDS in Africa. Harvard Business School, mimeo
Westoff C, Cross A (2006) The stall in the fertility transition in Kenya. DHS Analytical Studies no. 9
Williams BG, Taljaard D, Campbell CM, Gouws E, Ndhlovu L, Van Dam J, Caral M, Auvert B (2003) Changing patterns of knowledge, reported behavior and sexually transmitted infections in a South African gold mining community. AIDS 17:2099–2107
World Bank (2006) World development indicators
Young A (2005) The gift of the dying: the tragedy of AIDS and the welfare of future African generations. Q J Econ 120(2):423–466
Young A (2007) In sorrow to bring forth children: fertility amidst the plaque of HIV. J Econ Growth 12(4):283–327
Acknowledgements
The author thanks Emily Oster, Rodrigo Soares, two anonymous referees, and the seminar participants at Bilkent University, Brown University, Harvard University School of Public Health, METU, and participants of the 2005 conference on “Health, Demographics and Economic Development” at Stanford University, of the 2006 AIDS Workshop at Amsterdam Institute for International Development for valuable comments and suggestions. The author also thanks Ms. Laura Heaton of the Health Studies Branch, Population Division, the US Bureau of Census for providing her the HIV estimates.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Junsen Zhang
Appendix
Appendix
1.1 Country-level data
Countries with survey years
Benin (1996, 2001), Burkina Faso (1992/1993, 1998/1999, 2003), Burundi (1987), Cameroon (1991, 1998), Central Republic of Africa (1994/1995), Chad (1996/1997), Cote D’Ivoire (1994, 1998), Ethiopia (2000), Gabon (2000), Ghana (1988, 1993, 1998, 2003), Guinea (1999), Kenya (1989, 1993, 1998, 2003), Liberia (1986), Malawi (1992, 2000), Mali (1987, 1995/1996, 2001), Mozambique (1997), Namibia (1992, 2000), Niger (1992, 1998), Nigeria (1990, 1999, 2003), Rwanda (1992, 2000), Senegal (1986, 1992/1993, 1997), South Africa (1998), Tanzania (1992, 1996, 1999), Togo (1988, 1998), Uganda (1988, 1995, 2000/2001), Zambia (1992, 1996, 2001/2002), and Zimbabwe (1988, 1994, 1999).
The following countries have no surveys. Angola, Botswana, Comoros, Congo Democratic Republic, Congo Republic, Equatorial Guinea, Guinea-Bissau, Lesotho, Mauritania, Mauritius, Seychelles, Sierra Leone, Sudan, and Swaziland.
-
AIDS: The AIDS data come from UNAIDS/WHO, Epidemiological Fact Sheets (2003) and US Census Bureau HIV/AIDS Surveillance Database (2005). These are the number of reported AIDS cases for each country in every year and available for 44 African countries for 1985–2004. I multiply these number of reported incidents by 100,000 and divide by the country’s population in each year, converting them to incidence per 100,000 per country per year.
-
Enrollment rates: Gross school enrollment rates are from World Bank, Word Development Indicators (2006). They are available for 35 countries and years between 1985 and 2004.
-
GDP per capita: GDP per capita (PPP 2000 $s) is from World Bank, World Development Indicators (2006).
-
HIV: HIV prevalence rates among pregnant women are from the US Census Bureau, HIV Surveillance Database (2003). UNAIDS/WHO also provides similar data. Both Census and UNAIDS databases collect all studies and estimates of HIV/AIDS prevalence since the early 1980s. They provide information on prevalence, population and other factors and also provide regional estimates. The main indicator for the epidemic is the percent HIV-1 incidence among pregnant women for each country and year.
-
HIV-EPP: The International Programs Center of the Census Bureau uses Estimation and Projection Package (EPP) from WHO/UNAIDS to estimate and project adult HIV prevalence among 15–49-year olds from surveillance data between 1985 and 2004. While EPP can be used in all countries with sufficient surveillance data, it is specifically recommended for countries with generalized epidemics. Generalized epidemics are those that have broken out into the general population or consistent HIV prevalence at over 1% in low-risk individuals. The proxy for low-risk individuals is women attending antenatal clinics. The input to EPP in countries with generalized epidemics is surveillance data from various sites and years showing HIV prevalence among pregnant women, as well as data from national population-based surveys. EPP estimates the trends over time of HIV prevalence by fitting an epidemiological model to data from urban and rural sites. It tests possible epidemiological parameters, chooses a set minimizing least squares and projects future course based on fitted parameters, such as a parameter for the start year of the epidemic; one for the force of infection (how explosive the epidemic is in its initial stage); one for the fraction of new entrants to the population going into to the at-risk category (a parameter largely determines where the epidemic levels off); and one for the recruitment (a high value means people are brought into the at-risk population as people die of HIV, thus helping to sustain the epidemic at a higher level).
-
Infant mortality: Infant mortality is the rate per 1,000 live births and from World Bank, World Development Indicators (2006). The data are available for 8 years (1985, 1987, 1990, 1992, 1995, 1997, 2000, and 2004).
-
Total fertility rate: Data on total fertility rates are from World Bank, World Development Indicators (2006) and available for 10 years (1985, 1987, 1990, 1992, 1995, 1997, 2000, 2002, 2003, and 2004), and 44 countries. DHS data on total fertility rate per woman ages 15–49 are from DHS, www.measuredhs.com, MEASURE DHS, Macro International Inc. The data are available for 34 countries whose survey years fall between 1986 and 2004.
1.2 Regional-level data
Regions
- Benin:
-
Atacora Province, Atlantique Province, Borgou Province, Mono Province, Oueme Province, and Zou Province.
- Ethiopia:
-
Addis Ababa, Dire Dawa, Gambella, and Harari.
- Ghana:
-
Accra, the Northern region, the upper East region, and the upper West region.
- Lesotho:
-
Maseru, Leribe district, Mafeteng district, Quthing district, and Mokhotlong.
- Madagascar:
-
Antananarivo, Antsiranana, Fianarantsoa, Mahajanga, Toamasina, and Toliary.
- Malawi:
-
Lilongwe, Blantyre, Mangochi, Mulanje, Mzimba, and Thyolo.
- Mali:
-
Bamako, Koulikoro, Mopti, and Sikasso.
- Niger:
-
Dosso, Maradi, Niamey, Tahoua, and Zinder.
- Nigeria:
-
North East zone, North West zone, South East zone, and South West zone.
- Rwanda:
-
Butare, Byumba, Gisenyi, Kigali, and Ruhengeri.
- South Africa:
-
Eastern Cape Province, Free State Province, Gauteng Province, Mpumalanga Province, Northern Cape Province, Northern Province, North-West Province, and Western Cape Province.
- Tanzania:
-
Dar es Salaam, Rukwa region, Arusha region, and Zanzibar area.
- Togo:
-
Kara, Plateaux, and Savanes.
- Zimbabwe:
-
Harare, Bulawayo, Manicaland, Masvingo, Mashonaland West Province, and Matabeleland South.
-
Fertility rates: Regional fertility rates are from DHS, www.measuredhs.com, MEASURE DHS, Macro International Inc., and available for 14 countries, whose surveys years fall between 1988 and 2004.
-
HIV rates–US census: Regional HIV data come from US Census Bureau, HIV Surveillance Database (2005) and available for 14 African countries. The data are available for 1985–1990 and also for later years for a smaller number of regions.
1.3 Individual-level data
Individual-level data are used for 27 countries from 57 Demographic Health Surveys: Benin (1996 and 2001), Burkina Faso (1992/1993, 1998/1999, and 2003), Burundi (1987), Cameroon (1991, 1998), Central Republic of Africa (1994/1995), Chad (1996/1997), Cote D’Ivoire (1994 and 1998), Ethiopia (2000), Gabon (2000), Ghana (1988, 1993, 1998, and 2003), Guinea (1999), Kenya (1989, 1993, 1998, 2003), Liberia (1986), Malawi (1992 and 2000), Mali (1987, 1995/1996, and 2001), Mozambique (1997), Namibia (1992 and 2000), Niger (1992, 1998), Nigeria (1990, 1999, and 2003), Rwanda (1992 and 2000), Senegal (1986, 1992/1993, and 1997), South Africa (1998), Tanzania (1992, 1996, and 1999), Togo (1988 and 1998), Uganda (1988, 1995, and 2000/2001), Zambia (1992, 1996, and 2001/2002), and Zimbabwe (1988, 1994, and 1999).
-
Educational attainment: This is a categorical variable for woman’s educational attainment level. Categories are “No Education”, “Primary Education”, “Secondary Education”, “Tertiary Education” (v106).
-
Fertility: Measured as number of births or pregnancies in last year for each woman (v209).
-
Controls: Other control variables from are: Age (v121), year of survey (v007), presence of radio in the household (v120), presence of television in the household (v121), presence of refrigerator in the household (v122), presence of bicycle in the household (v123), urban/rural (v102), number of born children (v201), and number of living children (v201-v206-v207).
Rights and permissions
About this article
Cite this article
Kalemli-Ozcan, S. AIDS, “reversal” of the demographic transition and economic development: evidence from Africa. J Popul Econ 25, 871–897 (2012). https://doi.org/10.1007/s00148-011-0368-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00148-011-0368-6