
Abstract
Summary
Boys with vertebral fractures (VF) identified through routine spine radiographs had milder, less symptomatic, and fewer VF compared to those diagnosed with VF following consultation for back pain. Spontaneous (i.e., medication-unassisted) reshaping of fractured vertebral bodies was absent. Long bone fractures were present even before Duchenne muscular dystrophy (DMD) diagnosis in some boys.
Introduction
The objective of the study was to determine the time to and characteristics of first fractures in Duchenne muscular dystrophy.
Methods
This study was a retrospective longitudinal study of 30 boys with DMD <18 years. Boys were classified into four groups according to their first fracture: those with VF identified on routine lateral spine radiographs, those with VF diagnosed following consultation for back pain, those with long bone fractures, and those without fractures.
Results
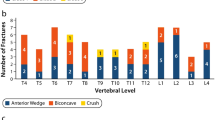
Compared to boys diagnosed with VF as their initial fracture following consultation for back pain, those with VF surveillance radiographs had shorter durations of glucocorticoid (GC) therapy at the time of VF diagnosis (median 1.6 versus 5.3 years, p < 0.01), higher areal (mean ± standard deviation −1.4 ± 0.7 versus −3.1 ± 0.8, p = 0.01), and volumetric (−0.3 ± 0.5 versus −2.6 ± 0.8, p < 0.01) lumbar spine bone mineral density Z-scores, as well as fewer VF (median 1.4 versus 5.2 per person, p < 0.01) and a lower median spinal deformity index (median 1.5 versus 9.5, p < 0.01). Vertebral body reshaping following VF was not observed. Ten boys sustained a long bone fracture as their first fracture at a mean age of 8.9 ± 4.0 years; four of these boys later sustained a total of 27 incident VF.
Conclusions
Routine lateral spine radiographs led to detection of VF in their earlier stages, vertebral body reshaping following VF was absent, and VF were frequent after the first long bone fracture. These results support the inclusion of a lateral spine radiograph starting at the time of GC initiation as part of routine bone health monitoring in DMD.




Similar content being viewed by others


References
Emery AE (1991) Population frequencies of inherited neuromuscular diseases—a world survey. Neuromuscul Disord 1:19–29
McDonald CM, Abresch RT, Carter GT, Fowler WM Jr, Johnson ER, Kilmer DD, Sigford BJ (1995) Profiles of neuromuscular diseases. Duchenne muscular dystrophy. Am J Phys Med Rehabil 74:S70–S92
Manzur AY, Kuntzer T, Pike M, Swan AV (2009) Glucocorticoid corticosteroids for Duchnne muscular dystrophy (Review). The Cochrane Library., pp 1–91
McMillan HJ, Campbell C, Mah JK (2010) Duchenne muscular dystrophy: Canadian paediatric neuromuscular physicians survey. Can J Neurol Sci 37:195–205
Larson CM, Henderson RC (2000) Bone mineral density and fractures in boys with Duchenne muscular dystrophy. J Pediatr Orthop 20:71–74
McDonald DG, Kinali M, Gallagher AC, Mercuri E, Muntoni F, Roper H, Jardine P, Jones DH, Pike MG (2002) Fracture prevalence in Duchenne muscular dystrophy. Dev Med Child Neurol 44:695–698
King WM, Ruttencutter R, Nagaraja HN, Matkovic V, Landoll J, Hoyle C, Mendell JR, Kissel JT (2007) Orthopedic outcomes of long-term daily corticosteroid treatment in Duchenne muscular dystrophy. Neurology 68:1607–1613
Alos N, Grant RM, Ramsay T et al (2012) High incidence of vertebral fractures in children with acute lymphoblastic leukemia 12 months after the initiation of therapy. J Clin Oncol 30:2760–2767
Rodd C, Lang B, Ramsay T et al (2012) Incident vertebral fractures among children with rheumatic disorders 12 months after glucocorticoid initiation: a national observational study. Arthritis Care Res 64:122–131
Marshall WA, Tanner JM (1970) Variations in the pattern of pubertal changes in boys. Arch Dis Child 45:13–23
Greulich WW, Pyle SI (1959) Radiographic atlas of skeletal development of the hand and wrist, 2nd edn. Stanford University Press, Stanford
Ogden CL, Kuczmarski RJ, Flegal KM, Mei Z, Guo S, Wei R, Grummer-Strawn LM, Curtin LR, Roche AF, Johnson CL (2002) Centers for Disease Control and Prevention 2000 growth charts for the United States: improvements to the 1977 National Center for Health Statistics version. Pediatrics 109:45–60
Institute of Medicine (2011) Dietary reference intakes for calcium and vitamin D. The National Academies Press, Washington, DC
Sbrocchi AM, Rauch F, Jacob P, McCormick A, McMillan HJ, Matzinger MA, Ward LM (2012) The use of intravenous bisphosphonate therapy to treat vertebral fractures due to osteoporosis among boys with Duchenne muscular dystrophy. Osteoporos Int 23:2703–2711
Fujita T, Satomura A, Hidaka M, Ohsawa I, Endo M, Ohi H (2000) Acute alteration in bone mineral density and biochemical markers for bone metabolism in nephrotic patients receiving high-dose glucocorticoid and one-cycle etidronate therapy. Calcif Tissue Int 66:195–199
Feber J, Gaboury I, Ni A et al (2012) Skeletal findings in children recently initiating glucocorticoids for the treatment of nephrotic syndrome. Osteoporos Int 23:751–760
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137–1148
Cummings EA, Ma J, Fernandez CV et al (2015) Incident vertebral fractures in children with leukemia during the four years following diagnosis. J Clin Endocrinol Metab 100:3408–3417
LeBlanc CM, Ma J, Taljaard M et al (2015) Incident vertebral fractures and risk factors in the first three years following glucocorticoid initiation among pediatric patients with rheumatic disorders. J Bone Miner Res 30:1667–1675
Kerkeni S, Kolta S, Fechtenbaum J, Roux C (2009) Spinal deformity index (SDI) is a good predictor of incident vertebral fractures. Osteoporos Int 20:1547–1552
Kroger H, Kotaniemi A, Vainio P, Alhava E (1992) Bone densitometry of the spine and femur in children by dual-energy x-ray absorptiometry. Bone Miner 17:75–85
van der Sluis IM, de Ridder MA, Boot AM, Krenning EP, de Muinck Keizer-Schrama SM (2002) Reference data for bone density and body composition measured with dual energy x ray absorptiometry in white children and young adults. Arch Dis Child 87:341–347; discussion 341–347
James KA, Cunniff C, Apkon SD, Mathews K, Lu Z, Holtzer C, Pandya S, Ciafaloni E, Miller L (2015) Risk factors for first fractures among males with Duchenne or Becker muscular dystrophy. J Pediatr Orthop 35:640–644
Bushby K, Finkel R, Birnkrant DJ et al (2010) Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol 9:77–93
Moxley RT 3rd, Ashwal S, Pandya S, Connolly A, Florence J, Mathews K, Baumbach L, McDonald C, Sussman M, Wade C (2005) Practice parameter: corticosteroid treatment of Duchenne dystrophy: report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 64:13–20
Nelson DA, Kleerekoper M, Peterson EL (1994) Reversal of vertebral deformities in osteoporosis: measurement error or “rebound”? J Bone Miner Res 9:977–982
Dal Osto LC, Konji VN, Halton J, Matzinger MA, Bassal M, Rauch F, Ward LM (2016) The spectrum of recovery from fracture-induced vertebral deformity in pediatric leukemia. Pediatr Blood Cancer 63:1107–1110
Ward LM, Glorieux FH, Rauch F, Verbruggen N, Heyden N, Lombardi A (2005) A randomized, placebo-controlled trial of oral alendronate in children and adolescents with osteogenesis imperfecta. Bone 36:0–18
Rauch F, Munns CF, Land C, Cheung M, Glorieux FH (2009) Risedronate in the treatment of mild pediatric osteogenesis imperfecta: a randomized placebo-controlled study. J Bone Miner Res 24:1282–1289
Sakkers R, Kok D, Engelbert R, van Dongen A, Jansen M, Pruijs H, Verbout A, Schweitzer D, Uiterwaal C (2004) Skeletal effects and functional outcome with olpadronate in children with osteogenesis imperfecta: a 2-year randomised placebo-controlled study. Lancet 363:1427–1431
Gatti D, Antoniazzi F, Prizzi R, Braga V, Rossini M, Tato L, Viapiana O, Adami S (2005) Intravenous neridronate in children with osteogenesis imperfecta: a randomized controlled study. J Bone Miner Res 20:758–763
Antoniazzi F, Zamboni G, Lauriola S, Donadi L, Adami S, Tato L (2006) Early bisphosphonate treatment in infants with severe osteogenesis imperfecta. J Pediatr 149:174–179
Astrom E, Jorulf H, Soderhall S (2007) Intravenous pamidronate treatment of infants with severe osteogenesis imperfecta. Arch Dis Child 92:332–338
Palomo T, Fassier F, Ouellet J, Sato A, Montpetit K, Glorieux FH, Rauch F (2015) Intravenous bisphosphonate therapy of young children with osteogenesis imperfecta: skeletal findings during follow up throughout the growing years. J Bone Miner Res 30:2150–2157
Allington N, Vivegnis D, Gerard P (2005) Cyclic administration of pamidronate to treat osteoporosis in children with cerebral palsy or a neuromuscular disorder: a clinical study. Acta Orthop Belg 71:91–97
Soderpalm AC, Magnusson P, Ahlander AC, Karlsson J, Kroksmark AK, Tulinius M, Swolin-Eide D (2007) Low bone mineral density and decreased bone turnover in Duchenne muscular dystrophy. Neuromuscul Disord 17:919–928
Ma J, Siminoski K, Alos N et al (2015) The choice of normative pediatric reference database changes spine bone mineral density Z-scores but not the relationship between bone mineral density and prevalent vertebral fractures. J Clin Endocrinol Metab 100:1018–1027
Bishop N, Arundel P, Clark E, Dimitri P, Farr J, Jones G, Makitie O, Munns CF, Shaw N (2014) Fracture prediction and the definition of osteoporosis in children and adolescents: the ISCD 2013 pediatric official positions. J Clin Densitom 17:275–280
Bachrach LK (2014) Diagnosis and treatment of pediatric osteoporosis. Curr Opin Endocrinol Diabetes Obes 21:454–460
Makitie O (2013) Causes, mechanisms and management of paediatric osteoporosis. Nat Rev Rheumatol 9:465–475
Ward LM, Konji V, Ma J (2016) Management of osteoporosis in children. Osteoporos Int 27:2147–2179
Hogler W, Ward L (2015) Osteoporosis in children with chronic disease. Endocr Dev 28:176–195
Misof BM, Roschger P, McMillan HJ, Ma J, Klaushofer K, Rauch F, Ward LM (2016) Histomorphometry and bone matrix mineralization before and after bisphosphonate treatment in boys with Duchenne muscular dystrophy: a paired trans-iliac biopsy study. J Bone Miner Res 31:1060–1069
Acknowledgments
This work was supported by the following programs and organizations: (1) LMW: The Canadian Institutes for Health Research New Investigator Program, The Canadian Child Health Clinician Scientist Program, the Children’s Hospital of Eastern Ontario (CHEO) Research Institute, The University of Ottawa Research Chair Program and the CHEO Departments of Pediatrics and Surgery; (2) JM: The CHEO Research Institute. (3) VNK: The CHEO Department of Surgery.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the CHEO Research Ethics Board.
Conflicts of interest
Leanne M. Ward has been a consultant to Novartis and Amgen Pharmaceuticals. Jinhui Ma, Hugh J McMillan, Gülay Karagüzel, Claire Goodin, Julie Wasson, Mary Ann Matzinger, Poppy DesClouds, Danielle Cram, Marika Page, Victor N Konji and Brian Lentle declare that they have no conflict of interest.
Funding
University of Ottawa Research Chair Programme and the CHEO Departments of Pediatrics and Surgery.
Rights and permissions
About this article

Cite this article
Ma, J., McMillan, H.J., Karagüzel, G. et al. The time to and determinants of first fractures in boys with Duchenne muscular dystrophy. Osteoporos Int 28, 597–608 (2017). https://doi.org/10.1007/s00198-016-3774-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-016-3774-5