
Abstract
Background
Common cause analysis of hospital safety events that involve radiology can identify opportunities to improve quality of care and patient safety.
Objective
To study the most frequent system failures as well as key activities and processes identified in safety events in an academic children’s hospital that underwent root cause analysis and in which radiology was determined to play a contributing role.
Materials and methods
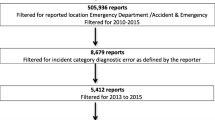
All safety events involving diagnostic or interventional radiology from April 2013 to November 2018, for which the hospital patient safety department conducted root cause analysis, were retrospectively analyzed. Pareto charts were constructed to identify the most frequent modalities, system failure modes, key processes and key activities.
Results
In 19 safety events, 64 sequential interactions were attributed to the radiology department by the patient safety department. Five of these safety events were secondary to diagnostic errors. Interventional radiology, radiography and diagnostic fluoroscopy accounted for 89.5% of the modalities in these safety events. Culture and process accounted for 55% of the system failure modes. The three most common key processes involved in these sequential interactions were diagnostic (39.1%) and procedural services (25%), followed by coordinating care and services (18.8%). The two most common key activities were interpreting/analyzing (21.9%) and coordinating activities (15.6%).
Conclusion
Proposing and implementing solutions based on the analysis of a single safety event may not be a robust strategy for process improvement. Common cause analyses of safety events allow for a more robust understanding of system failures and have the potential to generate more specific process improvement strategies to prevent the reoccurrence of similar errors. Our analysis demonstrated that the most common system failure modes in safety events attributed to radiology were culture and process. However, the generalizability of these findings is limited given our small sample size. Aligning with other children’s hospitals to use standard safety event terminology and shared databases will likely lead to greater clarity on radiology’s direct and indirect contributions to patient harm.





Similar content being viewed by others

References
Lyren A, Brilli RJ, Zieker K et al (2017) Children’s hospitals’ solutions for patient safety collaborative impact on hospital-acquired harm. Pediatrics 140. https://doi.org/10.1542/peds.2016-3494
Lyren A, Coffey M, Shepherd M et al (2018) We will not compete on safety: how children's hospitals have come together to hasten harm reduction. Jt Comm J Qual Patient Saf 44:377–388
Lyren A, Dawson A, Purcell D et al (2019) Developing evidence for new patient safety bundles through multihospital collaboration. J Patient Saf. https://doi.org/10.1097/PTS.0000000000000564
Throop C, Stockmeier C (2011) SEC & SSER Patient safety measurement system for healthcare, revision 2. Virginia Beach, VA: Healthcare Performance Improvement (HPI) white paper series
McClead RE, Brady M (2016) Sentinel events/patient safety events. Pediatr Rev 37:448–450
Teets J, Czekalinski S, Teman S (2015) Forging together without competition: embedding culture principles using cause analysis. https://www.solutionsforpatientsafety.org/wp-content/uploads/CMS-Special-Webinar-3-11-15-FINAL-Read-Only.pdf. Accessed 12 Feb 2020
Vincent C, Carthey J, Macrae C, Amalberti R (2017) Safety analysis over time: seven major changes to adverse event investigation. Implement Sci 12:151
Trbovich P, Shojania KG (2017) Root-cause analysis: swatting at mosquitoes versus draining the swamp. BMJ Qual Saf 26:350–353
Marx D (2019) Patient safety and the just culture. Obstet Gynecol Clin N Am 46:239–245
Larson DB, Kruskal JB, Krecke KN, Donnelly LF (2015) Key concepts of patient safety in radiology. Radiographics 35:1677–1693
Choksi VR, Marn C, Piotrowski MM et al (2005) Illustrating the root-cause-analysis process: creation of a safety net with a semiautomated process for the notification of critical findings in diagnostic imaging. J Am Coll Radiol 2:768–776
Brook OR, Kruskal JB, Eisenberg RL, Larson DB (2015) Root cause analysis: learning from adverse safety events. Radiographics 35:1655–1667
Morse RB, Pollack MM (2012) Root cause analyses performed in a children's hospital: events, action plan strength, and implementation rates. J Healthc Qual 34:55–61
Charles R, Hood B, Derosier JM et al (2016) How to perform a root cause analysis for workup and future prevention of medical errors: a review. Patient Saf Surg 10:20
Kung JW, Brook OR, Eisenberg RL, Slanetz PJ (2016) How-I-do-it: teaching root cause analysis. Acad Radiol 23:881–884
Kudla AU, Brook OR (2018) Quality and efficiency improvement tools for every radiologist. Acad Radiol 25:757–766
Mallett R, Conroy M, Saslaw LZ, Moffatt-Bruce S (2012) Preventing wrong site, procedure, and patient events using a common cause analysis. Am J Med Qual 27:21–29
Browne AM, Mullen R, Teets J et al (2008) Common cause analysis: focus on institutional change. In: Henriksen K, Battles JB, Keyes MA, Grady ML (eds) Advances in patient safety: new directions and alternatives approaches, vol 1. Rockville, Agency for Healthcare Research and Quality
Muething SE, Goudie A, Schoettker PJ et al (2012) Quality improvement initiative to reduce serious safety events and improve patient safety culture. Pediatrics 130:e423–e431
Flug JA, Ponce LM, Osborn HH, Jokerst CE (2018) Never events in radiology and strategies to reduce preventable serious adverse events. Radiographics 38:1823–1832
Donnelly LF, Palangyo T, Bargmann-Losche J et al (2019) Creating a defined process to improve the timeliness of serious safety event determination and root cause analysis. Pediatr Qual Saf 4:e200
Snyder EJ, Zhang W, Jasmin KC et al (2018) Gauging potential risk for patients in pediatric radiology by review of over 2,000 incident reports. Pediatr Radiol 48:1867–1874
Lee CS, Nagy PG, Weaver SJ, Newman-Toker DE (2013) Cognitive and system factors contributing to diagnostic errors in radiology. AJR Am J Roentgenol 201:611–617
Kim YW, Mansfield LT (2014) Fool me twice: delayed diagnoses in radiology with emphasis on perpetuated errors. AJR Am J Roentgenol 202:465–470
Bruno MA, Walker EA, Abujudeh HH (2015) Understanding and confronting our mistakes: the epidemiology of error in radiology and strategies for error reduction. Radiographics 35:1668–1676
Busby LP, Courtier JL, Glastonbury CM (2018) Bias in radiology: the how and why of misses and misinterpretations. Radiographics 38:236–247
Itri JN, Patel SH (2018) Heuristics and cognitive error in medical imaging. AJR Am J Roentgenol 210:1097–1105
Itri JN, Tappouni RR, McEachern RO et al (2018) Fundamentals of diagnostic error in imaging. Radiographics 38:1845–1865
Taylor GA, Voss SD, Melvin PR, Graham DA (2011) Diagnostic errors in pediatric radiology. Pediatr Radiol 41:327–334
Donnelly LF, Dickerson JM, Goodfriend MA, Muething SE (2010) Improving patient safety in radiology. AJR Am J Roentgenol 194:1183–1187
Donnelly LF, Dickerson JM, Goodfriend MA, Muething SE (2009) Improving patient safety: effects of a safety program on performance and culture in a department of radiology. AJR Am J Roentgenol 193:165–171
Sammer MBK, Sammer MD, Donnelly LF (2019) Review of learning opportunity rates: correlation with radiologist assignment, patient type and exam priority. Pediatr Radiol 49:1269–1275
Kellogg KM, Hettinger Z, Shah M et al (2017) Our current approach to root cause analysis: is it contributing to our failure to improve patient safety? BMJ Qual Saf 26:381–387
Braithwaite J, Westbrook MT, Mallock NA et al (2006) Experiences of health professionals who conducted root cause analyses after undergoing a safety improvement programme. Qual Saf Health Care 15:393–399
Wu AW, Lipshutz AKM, Pronovost PJ (2008) Effectiveness and efficiency of root cause analysis in medicine. JAMA 299:685–687
Wallace LM, Spurgeon P, Adams S et al (2009) Survey evaluation of the National Patient Safety Agency's root cause analysis training programme in England and Wales: knowledge, beliefs and reported practices. Qual Saf Health Care 18:288–291
van der Starre C, van Dijk M, van den Bos A, Tibboel D (2014) Paediatric critical incident analysis: lessons learnt on analysis, recommendations and implementation. Eur J Pediatr 173:1449–1457
Macrae C (2016) The problem with incident reporting. BMJ Qual Saf 25:71–75
Peerally MF, Carr S, Waring J, Dixon-Woods M (2017) The problem with root cause analysis. BMJ Qual Saf 26:417–422
Francois P, Lecoanet A, Caporossi A et al (2018) Experience feedback committees: a way of implementing a root cause analysis practice in hospital medical departments. PLoS One 13:e0201067
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Khalatbari, H., Menashe, S.J., Otto, R.K. et al. Clarifying radiology’s role in safety events: a 5-year retrospective common cause analysis of safety events at a pediatric hospital. Pediatr Radiol 50, 1409–1420 (2020). https://doi.org/10.1007/s00247-020-04711-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-020-04711-3