
Abstract
Introduction
Enhanced recovery after surgery (ERAS) programs have been developed to improve patient outcomes, accelerate recovery after surgery, and reduce healthcare costs. ERAS programs are a multimodal approach, with interventions during all stages of care. This meta-analysis examines the impact of ERAS programs on patient outcomes and recovery.
Methods
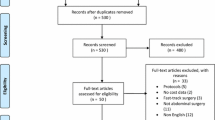
A comprehensive search of all published randomized control trials (RCTs) assessing the use of ERAS programs in surgical patients was conducted. Outcomes analyzed were length of stay (LOS), overall mortality, 30-day readmission rates, total costs, total complications, time to first flatus, and time to first bowel movement.
Results
Forty-two RCTs involving 5241 patients were analyzed. ERAS programs significantly reduced LOS, total complications, and total costs across all types of surgeries (p < 0.001). Return of gastrointestinal (GI) function was also significantly improved, as measured by earlier time to first flatus and time to first bowel movement, p < 0.001. There was no overall difference in mortality or 30-day readmission rates; however, 30-day readmission rates after upper GI surgeries nearly doubled with the use of ERAS programs (RR = 1.922; p = 0.019).
Conclusions
ERAS programs are associated with a significant reduction in LOS, total complications, total costs, as well as earlier return of GI function. Overall mortality and readmission rates remained similar, but there was a significant increase in 30-day readmission rates after upper GI surgeries. ERAS programs are effective and a valuable part in improving patient outcomes and accelerating recovery after surgery.








Similar content being viewed by others


References
Rose J, Weiser TG, Hider P, Wilson L, Gruen RL, Bickler SW (2015) Estimated need for surgery worldwide based on prevalence of diseases: a modelling strategy for the WHO Global Health Estimate. Lancet Glob Health 3(Suppl 2):S13–S20
Fearon KC, Ljungqvist O, Von MM, Revhaug A, Dejong CH, Lassen K et al (2005) Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 24(3):466–477
Kehlet H, Wilmore DW (2002) Multimodal strategies to improve surgical outcome. Am J Surg 183(6):630–641
Nanavati AJ, Prabhakar S (2014) Fast-track surgery: toward comprehensive peri-operative care. Anesth Essays Res 8(2):127–133
Varadhan KK, Neal KR, Dejong CH, Fearon KC, Ljungqvist O, Lobo DN (2010) The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr 29(4):434–440
Nicholson A, Lowe MC, Parker J, Lewis SR, Alderson P, Smith AF (2014) Systematic review and meta-analysis of enhanced recovery programmes in surgical patients. Br J Surg 101(3):172–188
Carli F (2015) Physiologic considerations of Enhanced Recovery After Surgery (ERAS) programs: implications of the stress response. Can J Anaesth 62(2):110–119
Neville A, Lee L, Antonescu I, Mayo NE, Vassiliou MC, Fried GM et al (2014) Systematic review of outcomes used to evaluate enhanced recovery after surgery. Br J Surg 101(3):159–170
Feldman LS, Lee L, Fiore J Jr (2015) What outcomes are important in the assessment of Enhanced Recovery After Surgery (ERAS) pathways? Can J Anaesth 62(2):120–130
Nygren J, Thacker J, Carli F, Fearon KC, Norderval S, Lobo DN et al (2012) Guidelines for perioperative care in elective rectal/pelvic surgery: enhanced Recovery After Surgery (ERAS(R)) Society recommendations. Clin Nutr 31(6):801–816
Greco M, Capretti G, Beretta L, Gemma M, Pecorelli N, Braga M (2014) Enhanced recovery program in colorectal surgery: a meta-analysis of randomized controlled trials. World J Surg 38(6):1531–1541. doi:10.1007/s00268-013-2416-8
Lei QC, Wang XY, Zheng HZ, Xia XF, Bi JC, Gao XJ et al (2015) laparoscopic versus open colorectal resection within fast track programs: an Update meta-analysis based on randomized controlled trials. J Clin Med Res 7(8):594–601
Bu J, Li N, Huang X, He S, Wen J, Wu X (2015) Feasibility of fast-track surgery in elderly patients with gastric cancer. J Gastrointest Surg 19(8):1391–1398
Wang H, Zhu D, Liang L, Ye L, Lin Q, Zhong Y et al (2015) Short-term quality of life in patients undergoing colonic surgery using enhanced recovery after surgery program versus conventional perioperative management. Qual Life Res 24(11):2663–2670
Wu CL, Benson AR, Hobson DB, Roda CP, Demski R, Galante DJ et al (2015) Initiating an enhanced recovery pathway program: an anesthesiology department’s perspective. Jt Comm J Qual Patient Saf 41(10):447–456
Pearsall EA, Meghji Z, Pitzul KB, Aarts MA, McKenzie M, McLeod RS et al (2015) A qualitative study to understand the barriers and enablers in implementing an enhanced recovery after surgery program. Ann Surg 261(1):92–96
Kahokehr A, Sammour T, Zargar-Shoshtari K, Thompson L, Hill AG (2009) Implementation of ERAS and how to overcome the barriers. Int J Surg 7(1):16–19
Hughes M, Coolsen MM, Aahlin EK, Harrison EM, McNally SJ, Dejong CH et al (2015) Attitudes of patients and care providers to enhanced recovery after surgery programs after major abdominal surgery. J Surg Res 193(1):102–110
Lyon A, Solomon MJ, Harrison JD (2014) A qualitative study assessing the barriers to implementation of enhanced recovery after surgery. World J Surg 38(6):1374–1380. doi:10.1007/s00268-013-2441-7
Roulin D, Donadini A, Gander S, Griesser AC, Blanc C, Hubner M et al (2013) Cost-effectiveness of the implementation of an enhanced recovery protocol for colorectal surgery. Br J Surg 100(8):1108–1114
Stowers MD, Lemanu DP, Hill AG (2015) Health economics in Enhanced Recovery After Surgery programs. Can J Anaesth 62(2):219–230
Stone AB, Grant MC, Pio RC, Hobson D, Pawlik T, Wu CL et al (2016) Implementation costs of an enhanced recovery after surgery program in the United States: a financial model and sensitivity analysis based on experiences at a quaternary academic medical center. J Am Coll Surg 222(3):219–225
Anderson AD, McNaught CE, MacFie J, Tring I, Barker P, Mitchell CJ (2003) Randomized clinical trial of multimodal optimization and standard perioperative surgical care. Br J Surg 90(12):1497–1504
Delaney CP, Zutshi M, Senagore AJ, Remzi FH, Hammel J, Fazio VW (2003) Prospective, randomized, controlled trial between a pathway of controlled rehabilitation with early ambulation and diet and traditional postoperative care after laparotomy and intestinal resection. Dis Colon Rectum 46(7):851–859
Gatt M, Anderson AD, Reddy BS, Hayward-Sampson P, Tring IC, MacFie J (2005) Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection. Br J Surg 92(11):1354–1362
Recart A, Duchene D, White PF, Thomas T, Johnson DB, Cadeddu JA (2005) Efficacy and safety of fast-track recovery strategy for patients undergoing laparoscopic nephrectomy. J Endourol 19(10):1165–1169
Petersen MK, Madsen C, Andersen NT, Soballe K (2006) Efficacy of multimodal optimization of mobilization and nutrition in patients undergoing hip replacement: a randomized clinical trial. Acta Anaesthesiol Scand 50(6):712–717
Gralla O, Haas F, Knoll N, Hadzidiakos D, Tullmann M, Romer A et al (2007) Fast-track surgery in laparoscopic radical prostatectomy: basic principles. World J Urol 25(2):185–191
Khoo CK, Vickery CJ, Forsyth N, Vinall NS, Eyre-Brook IA (2007) A prospective randomized controlled trial of multimodal perioperative management protocol in patients undergoing elective colorectal resection for cancer. Ann Surg 245(6):867–872
Larsen K, Sorensen OG, Hansen TB, Thomsen PB, Soballe K (2008) Accelerated perioperative care and rehabilitation intervention for hip and knee replacement is effective: a randomized clinical trial involving 87 patients with 3 months of follow-up. Acta Orthop 79(2):149–159
Muehling BM, Halter GL, Schelzig H, Meierhenrich R, Steffen P, Sunder-Plassmann L et al (2008) Reduction of postoperative pulmonary complications after lung surgery using a fast track clinical pathway. Eur J Cardiothorac Surg 34(1):174–180
Borgwardt L, Zerahn B, Bliddal H, Christiansen C, Sylvest J, Borgwardt A (2009) Similar clinical outcome after unicompartmental knee arthroplasty using a conventional or accelerated care program: a randomized, controlled study of 40 patients. Acta Orthop 80(3):334–337
Ionescu D, Iancu C, Ion D, Al-Hajjar N, Margarit S, Mocan L et al (2009) Implementing fast-track protocol for colorectal surgery: a prospective randomized clinical trial. World J Surg 33(11):2433–2438. doi:10.1007/s00268-009-0197-x
Muehling B, Schelzig H, Steffen P, Meierhenrich R, Sunder-Plassmann L, Orend KH (2009) A prospective randomized trial comparing traditional and fast-track patient care in elective open infrarenal aneurysm repair. World J Surg 33(3):577–585. doi:10.1007/s00268-008-9892-2
Muller S, Zalunardo MP, Hubner M, Clavien PA, Demartines N (2009) A fast-track program reduces complications and length of hospital stay after open colonic surgery. Gastroenterology 136(3):842–847
Serclova Z, Dytrych P, Marvan J, Nova K, Hankeova Z, Ryska O et al (2009) Fast-track in open intestinal surgery: prospective randomized study (Clinical Trials Gov Identifier no. NCT00123456). Clin Nutr 28(6):618–624
Liu XX, Jiang ZW, Wang ZM, Li JS (2010) Multimodal optimization of surgical care shows beneficial outcome in gastrectomy surgery. J Parenter Enter Nutr 34(3):313–321
Wang D, Kong Y, Zhong B, Zhou X, Zhou Y (2010) Fast-track surgery improves postoperative recovery in patients with gastric cancer: a randomized comparison with conventional postoperative care. J Gastrointest Surg 14(4):620–627
Demanet J, Wattier JM, Colin P, Fantoni JC, Villers A, Lebuffe G (2011) Feasibility of fast track strategy for patients undergoing radical nephrectomy: a prospective randomized study: 8AP4-10. Eur J Anaesth 28(Suppl 48):120
Garcia-Botello S, de Canovas LR, Tornero C, Escamilla B, Espi-Macias A, Esclapez-Valero P et al (2011) Implementation of a perioperative multimodal rehabilitation protocol in elective colorectal surgery. A prospective randomised controlled study. Cir Esp 89(3):159–166
Lee TG, Kang SB, Kim DW, Hong S, Heo SC, Park KJ (2011) Comparison of early mobilization and diet rehabilitation program with conventional care after laparoscopic colon surgery: a prospective randomized controlled trial. Dis Colon Rectum 54(1):21–28
Roig JV, Garcia-Fadrique A, Salvador A, Villalba FL, Tormos B, Lorenzo-Linan MA et al (2011) Selective intestinal preparation in a multimodal rehabilitation program. Influence on preoperative comfort and the results after colorectal surgery. Cir Esp 89(3):167–174
Sokouti M, Aghdam BA, Golzari SE, Moghadaszadeh M (2011) A comparative study of postoperative pulmonary complications using fast track regimen and conservative analgesic treatment: a randomized clinical trial. Tanaffos 10(3):12–19
Vlug MS, Wind J, Hollmann MW, Ubbink DT, Cense HA, Engel AF et al (2011) Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery: a randomized clinical trial (LAFA-study). Ann Surg 254(6):868–875
Wang G, Jiang ZW, Xu J, Gong JF, Bao Y, Xie LF et al (2011) Fast-track rehabilitation program vs conventional care after colorectal resection: a randomized clinical trial. World J Gastroenterol 17(5):671–676
Chen HJ, Xin JL, Cai L, Tao ZH, Yuan HS, Bing CH et al (2012) Preliminary experience of fast-track surgery combined with laparoscopy-assisted radical distal gastrectomy for gastric cancer. J Gastrointest Surg 16(10):1830–1839
Kim YM, Yim HW, Jeong SH, Klem ML, Callaway CW (2012) Does therapeutic hypothermia benefit adult cardiac arrest patients presenting with non-shockable initial rhythms?: a systematic review and meta-analysis of randomized and non-randomized studies. Resuscitation 83(2):188–196
Ren L, Zhu D, Wei Y, Pan X, Liang L, Xu J et al (2012) Enhanced Recovery After Surgery (ERAS) program attenuates stress and accelerates recovery in patients after radical resection for colorectal cancer: a prospective randomized controlled trial. World J Surg 36(2):407–414. doi:10.1007/s00268-011-1348-4
Wang G, Jiang Z, Zhao K, Li G, Liu F, Pan H et al (2012) Immunologic response after laparoscopic colon cancer operation within an enhanced recovery program. J Gastrointest Surg 16(7):1379–1388
Wang G, Jiang ZW, Zhao K, Gao Y, Liu FT, Pan HF et al (2012) Fast track rehabilitation programme enhances functional recovery after laparoscopic colonic resection. Hepatogastroenterology 59(119):2158–2163
Yang D, He W, Zhang S, Chen H, Zhang C, He Y (2012) Fast-track surgery improves postoperative clinical recovery and immunity after elective surgery for colorectal carcinoma: randomized controlled clinical trial. World J Surg 36(8):1874–1880. doi:10.1007/s00268-012-1606-0
Feng F, Ji G, Li JP, Li XH, Shi H, Zhao ZW et al (2013) Fast-track surgery could improve postoperative recovery in radical total gastrectomy patients. World J Gastroenterol 19(23):3642–3648
Jones C, Kelliher L, Dickinson M, Riga A, Worthington T, Scott MJ et al (2013) Randomized clinical trial on enhanced recovery versus standard care following open liver resection. Br J Surg 100(8):1015–1024
Lemanu DP, Singh PP, Berridge K, Burr M, Birch C, Babor R et al (2013) Randomized clinical trial of enhanced recovery versus standard care after laparoscopic sleeve gastrectomy. Br J Surg 100(4):482–489
Ni CY, Yang Y, Chang YQ, Cai H, Xu B, Yang F et al (2013) Fast-track surgery improves postoperative recovery in patients undergoing partial hepatectomy for primary liver cancer: a prospective randomized controlled trial. Eur J Surg Oncol 39(6):542–547
Feng F, Li XH, Shi H, Wu GS, Zhang HW, Liu XN et al (2014) Fast-track surgery combined with laparoscopy could improve postoperative recovery of low-risk rectal cancer patients: a randomized controlled clinical trial. J Dig Dis 15(6):306–313
Gonenc M, Dural AC, Celik F, Akarsu C, Kocatas A, Kalayci MU et al (2014) Enhanced postoperative recovery pathways in emergency surgery: a randomised controlled clinical trial. Am J Surg 207(6):807–814
Jia Y, Jin G, Guo S, Gu B, Jin Z, Gao X et al (2014) Fast-track surgery decreases the incidence of postoperative delirium and other complications in elderly patients with colorectal carcinoma. Langenbecks Arch Surg 399(1):77–84
Li K, Li JP, Peng NH, Jiang LL, Hu YJ, Huang MJ (2014) Fast-track improves post-operative nutrition and outcomes of colorectal surgery: a single-center prospective trial in China. Asia Pac J Clin Nutr 23(1):41–47
Lu H, Fan Y, Zhang F, Li G, Zhang C, Lu L (2014) Fast-track surgery improves postoperative outcomes after hepatectomy. Hepatogastroenterology 61(129):168–172
Mari GM, Costanzi A, Maggioni D, Origi M, Ferrari GC, De MP et al (2014) Fast-track versus standard care in laparoscopic high anterior resection: a prospective randomized-controlled trial. Surg Laparosc Endosc Percutaneous Tech 24(2):118–121
Nanavati AJ, Prabhakar S (2014) A comparative study of ‘fast-track’ versus traditional peri-operative care protocols in gastrointestinal surgeries. J Gastrointest Surg 18(4):757–767
Zhao G, Cao S, Cui J (2014) Fast-track surgery improves postoperative clinical recovery and reduces postoperative insulin resistance after esophagectomy for esophageal cancer. Support Care Cancer 22(2):351–358
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lau, C.S.M., Chamberlain, R.S. Enhanced Recovery After Surgery Programs Improve Patient Outcomes and Recovery: A Meta-analysis. World J Surg 41, 899–913 (2017). https://doi.org/10.1007/s00268-016-3807-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3807-4