
Abstract
Purpose
In this study, we addressed the correlation between the cross-sectional area (CSA) of the dural sac and the nerve root sedimentation sign (SedSign) and the correlation between the distance of claudication and the CSA of the dural sac or SedSign in patients with lumbar spinal stenosis. We also evaluated the reliability of clinical symptom prediction.
Methods
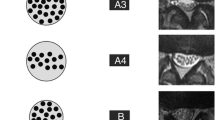
We checked claudication distance using a questionnaire, and we gauged low back pain when standing, referred pain, and radiating pain using visual analog scale scores. Three observers measured the CSA of the dural sac and SedSign, and normal nerve root sedimentation was classified as negative (N) and the absence of nerve root sedimentation was positive (P). P was sub-classified as positive with room [P(+); empty space apparent in the dura] or positive without room [P(−); no empty space in the dura]. SedSign reflected ongoing sedimentation inside the spinal canal of the nerve roots. We demonstrated negative sedimentation for the nerve root except for exiting nerve roots that settled into more than half of the dorsal region of the spinal canal and positive sedimentation as compressed nerve roots or as distribution of nerve roots that conglomerated from the ventral to the dorsal part of the equator as nerve roots. We evaluated functional outcomes using the Oswestry Disability Index and Roland–Morris Disability Questionnaire. One-way ANOVAs, Chi square tests, and correlation analyses evaluated the correlation CSAs and SedSigns.
Results
The total CSAs for the 716 sites were 98.63 ± 34.38 for N, 76.78 ± 28.78 for P(+), and 55.43 ± 27.77 for P(−), which were all statistically significant (p = 0.01). The correlations between pain and SedSign were not statistically significant (p > 0.05). There was no statistical significance in the correlations between the distance of the claudication and the CSA of the dura sac and the SedSign and between the functional score and the SedSign (both p > 0.05).
Conclusions
Increasing severity of SedSign indicates progressively smaller dural sac CSA, but there is an inconsistent association with clinical symptoms. Therefore, it is reasonable to suggest that spinal stenosis is severe in patients with severe symptoms.

Similar content being viewed by others


References
Atlas SJ, Keller RB, Robson D, Deyo RA, Singer DE (2000) Surgical and nonsurgical management of lumbar spinal stenosis: four-year outcomes from the maine lumbar spine study. Spine 25:556–562
Resende VAC, Teixeira A, Silva JBd, Neto AC, Leal FJF, Gouveia ARF, Miranda A (2013) Lumbar spinal stenosis: sedimentation sign. Columna 12:192–195. https://doi.org/10.1590/S1808-18512013000300003
Macedo LG, Wang Y, Battié MC (2013) Sedimentation sign for differential diagnosis of lumbar spinal stenosis. Spine 38:827–831. https://doi.org/10.1097/BRS.0b013e31827e8ecd
Atlas SJ, Keller RB, Wu YA, Deyo RA, Singer DE (2005) Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the maine lumbar spine study. Spine 30:936–943
Fritz JM, Erhard RE, Delitto A, Welch WC, Nowakowski PE (1997) Preliminary results of the use of a two-stage treadmill test as a clinical diagnostic tool in the differential diagnosis of lumbar spinal stenosis. J Spinal Disord Tech 10:410–416
Kapural L, Mekhail N, Bena J, McLain R, Tetzlaff J, Kapural M, Mekhail M, Polk S (2007) Value of the magnetic resonance imaging in patients with painful lumbar spinal stenosis (LSS) undergoing lumbar epidural steroid injections. Clin J Pain 23:571–575
Genevay S, Atlas SJ, Katz JN (2010) Variation in eligibility criteria from studies of radiculopathy due to a herniated disc and of neurogenic claudication due to lumbar spinal stenosis: a structured literature review. Spine 35:803–811. https://doi.org/10.1097/BRS.0b013e3181bc9454
Airaksinen O, Herno A, Turunen V, Saari T, Suomlainen O (1997) Surgical outcome of 438 patients treated surgically for lumbar spinal stenosis. Spine 22:2278–2282
Attias N, Hayman A, Hipp JA, Noble P, Essess SI (2006) Assessment of magnetic resonance imaging in the diagnosis of lumbar spine foraminal stenosis—a surgeon’s perspective. J Spinal Disord Tech 19:249–256
Haig AJ, Geisser ME, Tong HC, Yamakawa KS, Quint DJ, Hoff JT, Chiodo A, Miner JA, Phalke W (2007) Electromyographic and magnetic resonance imaging to predict lumbar stenosis, low back pain, and no back symptoms. J Bone Jt Surg Am 89:358–366
Speciale AC, Pietrobon R, Urban CW, Richardson WJ, Helms CA, Major N, Enterline D, Hey L, Haglund M, Turner DA (2002) Observer variability in assessing lumbar spinal stenosis severity on magnetic resonance imaging and its relation to cross-sectional spinal canal area. Spine 27:1082–1086
Sirvanci M, Bhatia M, Ganiyusufoglu KA et al (2008) Degenerative lumbar spinal stenosis: correlation with Oswestry Disability Index and MR imaging. Eur Spine J 17:679–685
Barz T, Melloh M, Staub LP, Lord SJ, Lange J, Röder CP, Theis JC, Merk HR (2010) Nerve root sedimentation sign: evaluation of a new radiological sign in lumbar spinal stenosis. Spine 35:892–897. https://doi.org/10.1097/BRS.0b013e3181c7cf4b
Fazal A, Yoo A, Bendo JA (2013) Does the presence of the nerve root sedimentation sign on MRI correlate with the operative level in patients undergoing posterior lumbar decompression for lumbar stenosis? Spine J 13:837–842. https://doi.org/10.1016/j.spinee.2013.02.067
Lee SY, Kim TH, Oh JK, Lee SJ, Park MS (2015) Lumbar stenosis: a recent update by review of literature. Asian Spine J 9:818–828. https://doi.org/10.4184/asj.2015.9.5.818
Hamanishi C, Matukura N, Fujita M, Tomihara M, Tanaka S (1994) Cross-sectional area of the stenotic lumbar dural tube measured from the transverse views of magnetic resonance imaging. J Spinal Disord Tech 7:388–393
Lurie JD, Tosteson AN, Tosteson TD, Carragee E, Carrino JA, Kaiser J, Sequeiros RT, Lecomte AR, Grove MR, Blood EA, Pearson LH, Weinstein JN, Herzog R (2008) Reliability of readings of magnetic resonance imaging features of lumbar spinal stenosis. Spine 33:1605–1610. https://doi.org/10.1097/BRS.0b013e3181791af3
Sigmundsson FG, Kang XP, Jönsson B, Strömqvist B (2011) Correlation between disability and MRI findings in lumbar spinal stenosis: a prospective study of 109 patients operated on by decompression. Acta Orthop 82:204–210. https://doi.org/10.3109/17453674.2011.566150
Geisser ME, Haig AJ, Tong HC, Yamakawa KS, Quint DJ, Hoff JT, Miner JA, Phalke W (2007) Spinal canal size and clinical symptoms among persons diagnosed with lumbar spinal stenosis. Clin J Pain 23:780–785
Herno A, Partanen K, Talaslahti T, Kaukanen E, Turunen V, Suomalainen O, Airaksinen O (1999) Long-term clinical and magnetic resonance imaging follow-up assessment of patients with lumbar spinal stenosis after laminectomy. Spine 24:1533–1537
Mariconda M, Galasso O, Imbimbo L, Lotti G, Milano C (2007) Relationship between alterations of the lumbar spine, visualized with magnetic resonance imaging, and occupational variables. Eur Spine J 16:255–266
Amundsen T, Weber H, Lilleås F, Nordal HJ, Abdelnoor M, Magnaes B (1995) Lumbar spinal stenosis: clinical and radiologic features. Spine 20:1178–1186
Alyas F, Connell D, Saifuddin A (2008) Upright positional MRI of the lumbar spine. Clin Radiol 63:1035–1048. https://doi.org/10.1016/j.crad.2007.11.022
Barz T, Melloh M, Staub L, Roeder C, Lange J, Smiszek FG, Theis JC, Merk HR (2008) The diagnostic value of a treadmill test in predicting lumbar spinal stenosis. Eur Spine J 17:686–690. https://doi.org/10.1007/s00586-008-0593-1
Deen HG, Zimmerman RS, Lyons MK, McPhee MC, Verheijde JL, Lemens SM (2000) Test–retest reproducibility of the exercise treadmill examination in lumbar spinal stenosis. Mayo Clin Proc 75:1002–1007
Barz T, Staub LP, Melloh M, Hamann G, Lord SJ, Chatfield MD, Bossuyt PM, Lange J, Merk HR (2014) Clinical validity of the nerve root sedimentation sign in patients with suspected lumbar spinal stenosis. Spine J 14:667–674. https://doi.org/10.1016/j.spinee.2013.06.105
Staub LP, Barz T, Melloh M, Lord SJ, Chatfiled M, Bossuyt PM (2011) Clinical validation study to measure the performance of the nerve root sedimentation sign for the diagnosis of lumbar spinal stenosis. Contemp Clin Trials 32:470–474. https://doi.org/10.1016/j.cct.2011.01.015
Kanno H, Ozawa H, Koizumi Y, Morozumi N, Aizawa T, Kusakabe T, Ishii Y, Itoi E (2012) Dynamic change of dural sac cross-sectional area in axial loaded MRI correlates with the severity of clinical symptoms in patients with lumbar spinal canal stenosis. Spine 37:207–213. https://doi.org/10.1097/BRS.0b013e3182134e73
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing financial interest.
Rights and permissions
About this article

Cite this article
Ko, S. Correlations between sedimentation sign, dural sac cross-sectional area, and clinical symptoms of degenerative lumbar spinal stenosis. Eur Spine J 27, 1623–1628 (2018). https://doi.org/10.1007/s00586-017-5374-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-017-5374-2