
Abstract
Background
Posttraumatic anterior shoulder instability is associated with anterior glenoid bone loss, contributing to recurrence. Accurate preoperative quantification of bone loss is paramount to avoid failure of a soft tissue stabilization procedure as bone reconstruction is recommended for glenoid defects greater than 20% to 27%.
Questions/purposes
We determined whether radiography, MRI, or CT was most reliable to quantify glenoid bone loss in recurrent anterior shoulder instability.
Methods
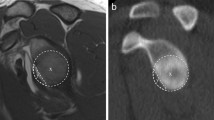
Seven intact fresh-frozen human cadaveric shoulders were imaged with radiography, MRI, CT, and three-dimensional (3-D) CT. Three sequential anterior glenoid defects then were created, measured, and the shoulders reimaged after each defect. Defect sizes were less than 12%, 12% to 25%, and 25% to 40%. The gold standard measurement was determined by comparing measurements taken on the cadaver by two surgeons using digital calipers with the measurements determined by using electronic digital calipers on the 3-D CT. This measurement was used for comparison of all estimations by the evaluators. Twelve independent blinded evaluators reviewed the 112 image sets and estimated the percent of glenoid bone loss. Images were scrambled and rereviewed by the same observers 2 months later to determine intraobserver reliability. We determined reliability with kappa values.
Results
Kappa values between predicted bone loss versus true loss (determined by our gold standard measurements) across all 12 raters for each modality were: 3-D CT, 0.50; CT, 0.40; MRI, 0.27; and radiographs, 0.15. Interobserver agreement (kappa) values were: 3-D CT, 0.54; CT, 0.47; MRI, 0.31; and radiographs, 0.15. The intraobserver agreement (kappa) values were: 3-D CT, 0.59; CT, 0.64; MRI, 0.51; and radiographs, 0.45.
Conclusions
Three-dimensional CT was the most reliable imaging modality for predicting glenoid bone loss. Regular CT was the second most reliable and reproducible modality.






Similar content being viewed by others


References
Barchilon VS, Kotz E, Barchilon Ben-Av M, Glazer E, Nyska M. A simple method for quantitative evaluation of the missing area of the anterior glenoid in anterior instability of the glenohumeral joint. Skeletal Radiol. 2008;37:731–736.
Bechhofer R, Santner R, Goldsman D. The Design and Analysis of Experiments for Statistical Selection, Screening, and Multiple Comparisons. New York, NY, USA: John Wiley and Sons; 1995.
Beran MC, Donaldson CT, Bishop JY. Treatment of chronic glenoid defects in the setting of recurrent anterior shoulder instability: a systematic review. J Shoulder Elbow Surg. 2010;19:769–780.
Bigliani LU, Newton PM, Steinmann SP, Connor PM, McIlveen SJ. Glenoid rim lesions associated with recurrent anterior dislocation of the shoulder. Am J Sports Med. 1998;26:41–45.
Boileau P, Villalba M, Hery JY, Balg F, Ahrens P, Neyton L. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. J Bone Joint Surg Am. 2006;88:1755–1763.
Burkhart SS, Danaceau SM. Articular arc length mismatch as a cause of failed bankart repair. Arthroscopy. 2000;16:740–744.
Burkhart SS, De Beer JF. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16:677–694.
Burkhart SS, De Beer JF, Barth JR, Cresswell T, Roberts C, Richards DP. Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss. Arthroscopy. 2007;23:1033–1041.
Burkhart SS, Debeer JF, Tehrany AM, Parten PM. Quantifying glenoid bone loss arthroscopically in shoulder instability. Arthroscopy. 2002;18:488–491.
Chen AL, Hunt SA, Hawkins RJ, Zuckerman JD. Management of bone loss associated with recurrent anterior glenohumeral instability. Am J Sports Med. 2005;33:912–925.
Chuang TY, Adams CR, Burkhart SS. Use of preoperative three-dimensional computed tomography to quantify glenoid bone loss in shoulder instability. Arthroscopy. 2008;24:376–382.
Edwards TB, Boulahia A, Walch G. Radiographic analysis of bone defects in chronic anterior shoulder instability. Arthroscopy. 2003;19:732–739.
Flatow EL, Warner JI. Instability of the shoulder: complex problems and failed repairs: Part I. Relevant biomechanics, multidirectional instability, and severe glenoid loss. Instr Course Lect. 1998;47:97–112.
Huijsmans PE, de Witte PB, de Villiers RV, Wolterbeek DW, Warmerdam P, Kruger NR, de Beer JF. Recurrent anterior shoulder instability: accuracy of estimations of glenoid bone loss with computed tomography is insufficient for therapeutic decision-making. Skeletal Radiol. 2011;40:1329–1334.
Huijsmans PE, Haen PS, Kidd M, Dhert WJ, van der Hulst VP, Willems WJ. Quantification of a glenoid defect with three-dimensional computed tomography and magnetic resonance imaging: a cadaveric study. J Shoulder Elbow Surg. 2007;16:803–809.
Itoi E, Lee SB, Berglund LJ, Berge LL, An KN. The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: a cadaveric study. J Bone Joint Surg Am. 2000;82:35–46.
Ljungquist KL, Butler RB, Griesser MJ, Bishop JY. Prediction of coracoid thickness using a glenoid width-based model: implications for bone reconstruction procedures in chronic anterior shoulder instability. J Shoulder Elbow Surg. 2012;21:815–821.
Lynch JR, Clinton JM, Dewing CB, Warme WJ, Matsen FA 3rd. Treatment of osseous defects associated with anterior shoulder instability. J Shoulder Elbow Surg. 2009;18:317–328.
Nofsinger C, Browning B, Burkhart SS, Pedowitz RA. Objective preoperative measurement of anterior glenoid bone loss: a pilot study of a computer-based method using unilateral 3-dimensional computed tomography. Arthroscopy. 2011;27:322–329.
Ochoa E Jr, Burkhart SS. Glenohumeral bone defects in the treatment of anterior shoulder instability. Instr Course Lect. 2009;58:323–336.
Saito H, Itoi E, Sugaya H, Minagawa H, Yamamoto N, Tuoheti Y. Location of the glenoid defect in shoulders with recurrent anterior dislocation. Am J Sports Med. 2005;33:889–893.
Sugaya H, Moriishi J, Dohi M, Kon Y, Tsuchiya A. Glenoid rim morphology in recurrent anterior glenohumeral instability. J Bone Joint Surg Am. 2003;85:878–884.
Tauber M, Resch H, Forstner R, Raffl M, Schauer J. Reasons for failure after surgical repair of anterior shoulder instability. J Shoulder Elbow Surg. 2004;13:279–285.
Yamamoto N, Itoi E, Abe H, Kikuchi K, Seki N, Minagawa H, Tuoheti Y. Effect of an anterior glenoid defect on anterior shoulder stability: a cadaveric study. Am J Sports Med. 2009;37:949–954.
Acknowledgments
We thank the New Albany Surgical Hospital Foundation for donating the cadaveric specimens used in this study. The imaging facilities were provided by The Ohio State University Department of Radiology. The participating members of the MOON group were: Bruce Miller MD, Charles Cox MD, Robert Brophy MD, Rick Wright MD, Brian Wolf MD, Benjamin Ma MD, Matthew Smith MD, Joseph Abboud MD, Keith Baumgarten MD, and Jed Kuhn MD.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
The institution of one of the authors (GJ) has received, during the study period, funding from Genzyme (Cambridge, MA, USA) and Biomet (Warsaw, IN, USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article
Cite this article
Bishop, J.Y., Jones, G.L., Rerko, M.A. et al. 3-D CT is the Most Reliable Imaging Modality When Quantifying Glenoid Bone Loss. Clin Orthop Relat Res 471, 1251–1256 (2013). https://doi.org/10.1007/s11999-012-2607-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2607-x