
Abstract
Objectives
To determine the prevalence and determinants of xerophthalmia among children aged 0–60 months.
Methods
This cross-sectional study included 3571 children under 5 years of age from six villages and four periurban areas. Children with xerophthalmia were identified and severity graded using the WHO classification. The main outcome measures were sociodemographic, nutritional and comorbidity related risk factors of xerophthalmia. A pretested questionnaire carrying information on the above factors was administered to the caregivers. Univariate and multivariate binary logistic regression analyses were performed to examine the association of each of these factors with xerophthalmia.
Results
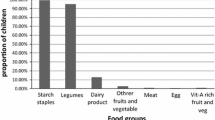
The overall prevalence of xerophthalmia was of serious public health importance at 9.1%. Prevalence of both mild (night blindness, and Bitot’s spots) and severe forms (corneal changes) of xerophthalmia increased with age. Bitot’s spots and night blindness were the commonest manifestations. Rural dwelling, lower social class, maternal illiteracy and occupation outside home were significant antecedent socio-demographic risk factors on univariate analysis. Multivariate analysis revealed low intake of proteins and vitamin A containing foods as well as predominant maize diet to be significant dietary factors. Nutritional wasting and a preceding history of measles were significant comorbid determinants (P<0.05). None of the socio-demographic variables emerged significant on multivariate analysis.
Conclusions
Vitamin A deficiency remains a significant public health problem in Aligarh district. The proximal factors in a child’s mileu viz nutrition and comorbidities were more significantly associated with xerophthalmia than the distal socio-demographic factors, thereby making a case for their cost effective prevention. The high magnitude of the problem calls for intensification of existing prophylactic measures in these areas.
Similar content being viewed by others


References
Ramakrishnan U, Darnton-Hill I. Assessment and control of vitamin A deficiency disorders. J Nutr. 2002;132:2947S–2953S.
Stephenson LS, Latham MC, Ottesen EA. Global malnutrition. Parasitology. 2000;121:S5–22.
NNMB National Nutrition Monitoring Bureau. Natio Institute of Nutrition, Hyderabad: NNMB Micronutrient Survey; 2002.
Kumar P. Social classification-need for constant updating. Indian J Comm Med. 1993;8:59–61.
WHO. Global Strategy for Infant and Young Child Feeding. Geneva: World Health Organization. 2003.
World Health Organization. Indicators for Assessing Vitamin A Deficiency and Their Application in Monitoring and Evaluating Intervention Programs. WHONUT/96. 10–66. Geneva: WHO; Micronutrient Series WHO/NUT. 1996.
Sommer A. Vitamin A deficiency and its consequences: A field guide to detection and control. Geneva: WHO publication, Third edition. 1995.
WHO Technical Report Series No. 590, 1976 (Vitamin A Deficiency and Xerophthalmia Report of a Joint WHO/USAID meeting). p. 17–18.
Pratinidhi AK, Shah U, Bapat VS. Screening tests for vitamin A deficiency. Indian J Pediatr. 1987;54:563–569.
WHO/UNICEF. “Indicators for Assessing Vitamin A Deficiency and their Application in Monitoring and Evaluating Intervention Programmes. Report of a Joint WHO/UNICEF Consultation. Geneva, Switzerland, 9–11 November 1992; Review Version. May 1994.
Khandait DW, Vasudeo ND, Zodpey SP, Ambadekar NN, Koram MR. Vitamin A intake and xerophthalmia among Indian children. Public Health. 1999;113;69–72.
Ajaiyeoba AI, Samaila E. Use of Bitot’s spot in screening for vitamin A deficiency in Nigerian children. Afr J Biomed Res. 2001;4:155–157.
Adelekan DA. Childhood nutrition and malnutrition in Nigeria. Nutrition. 2003;19:179–181.
Curtale F, Tammam H, Hammoud ES, Aloi A. Prevalence of xerophthalmia among children in Beheira governorate, Egypt. East Med Health J. 1999;5:984–991.
Swami HM, Thakur JS, Bhatia SP, Ahuja R. Rapid assessment and delivery of Vitamin A to slum children by using National Immunization Day in Chandigarh. Indian J Pediatr. 2001;68:719–723.
Pal R, Sagar V. Antecedent risk factors of xerophthalmia among Indian rural preschool children. Eye Contact Lens. 2008; 34:106–108.
Dole K, Gilbert C, Deshpande M, Khandekar R. Prevalence and determinants of xerophthalmia in preschool children in urban slums, Pune, India—A preliminary assessment. Ophthal Epidemio. 2009;16:8–14.
Semba RD, Pee SD, Panagides D, Poly O, Bloem MW. Risk factors for xerophthalmia among mothers and their children and for mother-child pairs with xerophthalmia in Cambodia. Arch Ophthalmol. 2004;122:517–523.
Sommer A, Muhilal. Nutritional factors in corneal xerophthalmia and keratomalacia. Arch Ophthalmol. 1982;100:399–403.
Semba RD. Bloen MW. Measles blindness. Surv Ophthalmol. 2004;49:243–255.
Schémann JF, Banou AA, Guindo A, Joret V, Traore L, Malvy D. Prevalence of undernutrition and vitamin A deficiency in the Dogon region, Mali. J Am Coll Nutr. 2002;21:381–387.
Measham CN, Khanum S, Ahmed N. Xerophthalmia in urban Bangladesh. Acta Pediatr Scand. 1983;72:531–536.
Harjes CE, Rocheford TR, Bai L, Brutnell TP, Kandianis CB, Sowinski SG, et al. Natural genetic variation in lycopene epsilon cyclase tapped for maize biofortification. Science. 2008;319:330–333.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sachdeva, S., Alam, S., Beig, F.K. et al. Determinants of vitamin a deficiency amongst children in Aligarh district, Uttar Pradesh. Indian Pediatr 48, 861–866 (2011). https://doi.org/10.1007/s13312-011-0140-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13312-011-0140-8