
Abstract
Purpose
Typically, selection of lowest instrumented vertebra (LIV) in Adolescent Idiopathic Scoliosis (AIS) is based on the coronal radiograph; however, increasing evidence suggests that fusions proximal to the stable sagittal vertebrae (SSV) on the lateral radiograph can result in distal junctional kyphosis (DJK). The purpose of this study is to compare rates of DJK in patients with AIS that have a discordance between the Lowest Touched Vertebra (LTV) and the SSV and to identify risk factors for developing DJK.
Methods
Patients with AIS Lenke type 1, 2 and 3 curves treated with a posterior spinal fusion were separated into two groups. Group 1 had SSV that was proximal to the LTV whereas group 2 had SSV that was distal to the LTV. Comparisons were made for patients that were fused to the SSV(a), LTV(b) or between(c). Distal junctional angle (DJA) > 5° and increasing kyphosis at the end of the fusion construct were evaluated as risk factors for DJK.
Results
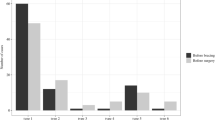
The rate of DJK was 0.0% in group 1a, 1b, and 1c compared to 4.3%, 18.5% and 10.0% in groups 2a, 2b and 2c, respectively(p < 0.001). The rate of DJK was 22.9% when the distal junctional angle(DJA) > 5° versus 1.4% when the DJA < 5°(p < 0.001).
Conclusion
There was a low risk for progression of DJK when the SSV was proximal to the LTV, however, those with SSV distal to the LTV represent a high-risk group. Importantly, the development of DJK occurred almost exclusively in patients with LIV at the thoracolumbar junction which demonstrates that surgeons need to be cautious when ending fusions at T11, T12, and L1 in patients at high risk for DJK. Furthermore, having a distal junctional angle 5° or greater increased the risk of developing DJK by roughly 16-fold. At a minimum of 5-year follow-up, the development of DJK did not appear to adversely impact SRS outcomes or revision rates.


Similar content being viewed by others


References
Hosseinpour-Feizi H, Soleimanpour J, Sales JG et al (2011) Lenke and King classification systems for adolescent idiopathic scoliosis: interobserver agreement and postoperative results. Int J Gen Med 4:821–825
King HA, Moe JH, Bradford DS et al (1983) The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am 65(9):1302–1313
King HA (1988) Selection of fusion levels for posterior instrumentation and fusion in idiopathic scoliosis. Orthop Clin North Am 19(2):247–255
Qin X, Sun W, Xu L, et al. (2016) Selecting the Last "Substantially" Touching Vertebra as Lowest Instrumented Vertebra in Lenke Type 1A Curve: Radiographic Outcomes With a Minimum of 2-year Follow-Up. Spine (Phila Pa 1976). 41(12):E742–50
Suk SI, Lee SM, Chung ER et al (2005) Selective thoracic fusion with segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis: more than 5-year follow-up. Spine 30(14):1602–1609
Lenke LG, Betz RR, Harms J et al (2001) Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 83(8):1169–1181
Fischer CR, Lenke LG, Bridwell KH et al (2018) Optimal Lowest Instrumented Vertebra for Thoracic Adolescent Idiopathic Scoliosis. Spine Deform 6(3):250–256
Matsumoto M, Watanabe K, Hosogane N et al (2013) Postoperative distal adding-on and related factors in Lenke type 1A curve. Spine 38(9):737–744
Cho KJ, Lenke LG, Bridwell KH et al (2009) Selection of the optimal distal fusion level in posterior instrumentation and fusion for thoracic hyperkyphosis: the sagittal stable vertebra concept. Spine 34(8):765–770
Yang J, Andras LM, Broom AM et al (2018) Preventing Distal Junctional Kyphosis by Applying the Stable Sagittal Vertebra Concept to Selective Thoracic Fusion in Adolescent Idiopathic Scoliosis. Spine Deform 6(1):38–42
Segal DN, Orland KJ, Yoon E et al (2020) Fusions ending above the sagittal stable vertebrae in adolescent idiopathic scoliosis: does it matter? Spine Deform 8(5):983–989
Marciano G, Ball J, Matsumoto H et al (2021) Including the stable sagittal vertebra in the fusion for adolescent idiopathic scoliosis reduces the risk of distal junctional kyphosis in Lenke 1–3 B and C curves. Spine Deform 9:733–741
Lowe TG, Lenke L, Betz R et al (2006) Distal junctional kyphosis of adolescent idiopathic thoracic curves following anterior or posterior instrumented fusion: incidence, risk factors, and prevention. Spine 31(3):299–302
Kim YJ, Bridwell KH, Lenke LG et al (2005) Proximal junctional kyphosis in adolescent idiopathic scoliosis following segmental posterior spinal instrumentation and fusion: minimum 5-year follow-up. Spine 30(18):2045–2050
Lee GA, Betz RR, Clements DH 3rd et al (1999) Proximal kyphosis after posterior spinal fusion in patients with idiopathic scoliosis. Spine 24(8):795–799
Zhong J, Cao K, Wang B et al (2019) Incidence and risk factors for proximal junctional kyphosis in adolescent idiopathic scoliosis after correction surgery: a meta-analysis. World Neurosurg 125:e326–e335
Ferrero E, Bocahut N, Lefevre Y et al (2018) Proximal junctional kyphosis in thoracic adolescent idiopathic scoliosis: risk factors and compensatory mechanisms in a multicenter national cohort. Eur Spine J 27(9):2241–2250
Homans JF, Kruyt MC, Schlosser TPC et al (2020) Changes in the position of the junctional vertebrae after posterior spinal fusion in adolescent idiopathic scoliosis: implication in risk assessment of proximal junctional kyphosis development. J Pediatr Orthop 40(2):e84–e90
Segal DN, Grabel ZJ, Konopka JA, et al. (2020) Fusions ending at the thoracolumbar junction in adolescent idiopathic scoliosis: comparison of lower instrumented vertebrae. Spine Deform 8(2):205–211
Wang PY, Chen CW, Lee YF et al (2021) Distal Junctional Kyphosis after Posterior Spinal Fusion in Lenke 1 and 2 Adolescent Idiopathic Scoliosis-Exploring Detailed Features of the Sagittal Stable Vertebra Concept. Global Spine J. https://doi.org/10.1177/21925682211019692
Ball JR, Konigsberg MW, Plachta, et al (2020) Variability in stable sagittal vertebra (SSV) during full-length biplanar xrays can affect the choice of fusion levels in patients with adolescent idiopathic scoliosis (AIS). Spine Deform 8:1261–1267
Acknowledgements
Acknowledgement of Support: Setting Scoliosis Straight Foundation receives funding from DePuy Synthes Spine, EOS imaging, K2M, Medtronic, NuVasive, Zimmer Biomet and the Food and Drug Administration in support of Harms Study Group research. Harms Study Group: Setting Scoliosis Straight Foundation receives funding from DePuy Synthes Spine, EOS imaging, K2M, Medtronic, NuVasive, Zimmer Biomet and the Food and Drug Administration in support of Harms Study Group research. HSG Acknowledgements: This study was supported in part by grants to the Setting Scoliosis Straight Foundation in support of Harms Study Group research from DePuy Synthes Spine, EOS imaging, Stryker Spine, Medtronic, NuVasive, Zimmer Biomet and the Food and Drug Administration.
Harms Study Group Investigators: Aaron Buckland, MD; Royal Children’s Hospital – Melbourne Australia; Amer Samdani, MD; Shriners Hospitals for Children—Philadelphia; Amit Jain, MD; Johns Hopkins Hospital; Baron Lonner, MD; Mount Sinai Hospital; Benjamin Roye, MD; Columbia University; Burt Yaszay, MD; Rady Children’s Hospital; Chris Reilly, MD; BC Children’s Hospital; Daniel Hedequist, MD; Boston Children’s Hospital; Daniel Sucato, MD; Texas Scottish Rite Hospital; David Clements, MD; Cooper Bone & Joint Institute New Jersey; Firoz Miyanji, MD; BC Children’s Hospital; Harry Shufflebarger, MD; Paley Orthopedic & Spine Institute; Jack Flynn, MD; Children’s Hospital of Philadelphia; John Asghar, MD; Paley Orthopedic & Spine Institute; Jean Marc Mac Thiong, MD; CHU Sainte-Justine; Joshua Pahys, MD; Shriners Hospitals for Children—Philadelphia; Juergen Harms, MD; Klinikum Karlsbad-Langensteinbach, Karlsbad; Keith Bachmann, MD; University of Virginia; Lawrence Lenke, MD; Columbia University; Lori Karol, MD; Children’s Hospital, Denver Colorado; Mark Abel, MD; University of Virginia; Mark Erickson, MD; Children’s Hospital, Denver Colorado; Michael Glotzbecker, MD; Rainbow Children’s Hospital, Cleveland; Michael Kelly, MD; Washington University; Michael G. Vitale, MD, MPH; Columbia University; Michelle Marks, PT, MA; Setting Scoliosis Straight Foundation; Munish Gupta, MD; Washington University; Nicholas Fletcher, MD; Emory University; Noelle Larson, MD; Mayo Clinic Rochester Minnesota; Patrick Cahill, MD; Children’s Hospital of Philadelphia; Paul Sponseller, MD; Johns Hopkins Hospital; Peter Gabos, MD: Nemours/Alfred I. duPont Hospital for Children; Peter Newton, MD; Rady Children’s Hospital; Peter Sturm, MD; Cincinnati Children’s Hospital; Randal Betz, MD; Institute for Spine & Scoliosis; Stefan Parent, MD: CHU Sainte-Justine; Stephen George, MD; Nicklaus Children's Hospital; Steven Hwang, MD; Shriners Hospitals for Children—Philadelphia; Suken Shah, MD; Nemours/Alfred I. duPont Hospital for Children; Sumeet Garg, MD; Children’s Hospital, Denver Colorado ; Tom Errico, MD; Nicklaus Children's Hospital; Vidyadhar Upasani, MD; Rady Children’s Hospital
Funding
This study was supported in part by grants to the Setting Scoliosis Straight Foundation in support of Harms Study Group research from DePuy Synthes Spine, EOS imaging, Stryker Spine, Medtronic, NuVasive, Zimmer Biomet and the Food and Drug Administration.
Author information
Authors and Affiliations
Consortia
Contributions
DNS: Synthesis of idea, data analysis, manuscript writing, editing, approving work. JB: Synthesis of idea, data analysis, manuscript writing, editing, approving work. NDF: Synthesis of idea, manuscript editing, approving work. EY: Data analysis, manuscript writing, editing, approving work. TB: Data analysis, manuscript writing, editing, approving work. MGV: Synthesis of idea, manuscript editing, approving work. Harms Study Group: Synthesis of idea, manuscript editing, approving work.
Corresponding author
Ethics declarations
IRB approval/research ethics committee
IRB approval for the multicenter study was obtained locally from each contributing institution’s review board, and consent was obtained from each patient prior to data collection.
Copyright and patient information
No copyrighted materials or patient information is included in this manuscript submission.
Rights and permissions
About this article

Cite this article
Segal, D.N., Ball, J., Fletcher, N.D. et al. Risk factors for the development of DJK in AIS patients undergoing posterior spinal instrumentation and fusion. Spine Deform 10, 377–385 (2022). https://doi.org/10.1007/s43390-021-00413-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43390-021-00413-4