
Abstract
Background
Many studies show significantly improved survival after R0 resection compared with R1 resection in pancreatic adenocarcinoma (PAC); however, the effect of neoadjuvant chemoradiation (NACRT) on this association is unknown.
Objective
The aim of this study was to evaluate the prognostic significance of positive surgical margins (SMs) after NACRT compared with upfront surgery + adjuvant therapy in PAC.
Methods
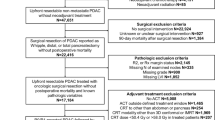
All cases of surgically resected PAC at a single institution were reviewed from 1996 to 2014; patients treated with palliative intent, metastatic disease, and biliary/ampullary tumors were excluded. The primary endpoint was overall survival (OS).
Results
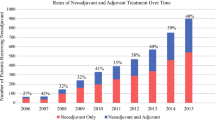
Overall, 300 patients were included; 134 patients received NACRT with concurrent 5-fluorouracil or gemcitabine followed by surgery, and 166 patients received upfront surgery (+ adjuvant chemotherapy in 72% of patients and RT in 65%); 31% of both groups had a positive SM (+SM). The median OS for patients with a +SM or negative SM (−SM) was 26.6 and 31.6 months, respectively for NACRT, and 12.0 and 24.5 months, respectively, for upfront surgery. OS was significantly improved with −SM compared with +SM in both groups (p = 0.006). When resection yielded +SM, NACRT patients had improved OS compared with upfront surgery patients (p < 0.001). On multivariable analysis, +SM in the upfront surgery group (hazard ratio [HR] 2.94, 95% confidence interval [CI] 2.04–4.24; p < 0.001) and older age (HR 1.01, 95% CI 1.00–1.03, per year; p = 0.007) predicted worse OS. +SM in the NACRT group was not associated with worse OS (HR 1.09, 95% CI 0.72–1.65; p = 0.70).
Conclusion
Patients with a positive margin after NACRT and surgery had longer survival compared with patients with a positive margin after upfront surgery. NACRT should be strongly considered for patients at high risk of R1 resections.




Similar content being viewed by others

References
Pingpank JF, Hoffman JP, Ross EA, et al. Effect of preoperative chemoradiotherapy on surgical margin status of resected adenocarcinoma of the head of the pancreas. J Gastrointest Surg. 2001;5:121–30.
Ghaneh P, Kleeff J, Halloran CM, et al. the impact of positive resection margins on survival and recurrence following resection and adjuvant chemotherapy for pancreatic ductal adenocarcinoma. Ann Surg. 2019;269:520–9.
Paniccia A, Hosokawa P, Henderson W, et al. Characteristics of 10-year survivors of pancreatic ductal adenocarcinoma. JAMA Surg. 2015;150:701–10.
Brown KM, Siripurapu V, Davidson M, et al. Chemoradiation followed by chemotherapy before resection for borderline pancreatic adenocarcinoma. Am J Surg. 2008;195:318–21.
Stessin AM, Meyer JE, Sherr DL. Neoadjuvant radiation is associated with improved survival in patients with resectable pancreatic cancer: an analysis of data from the surveillance, epidemiology, and end results (SEER) registry. Int J Radiat Oncol Biol Phys. 2008;72:1128–33.
Spitz FR, Abbruzzese JL, Lee JE, et al. Preoperative and postoperative chemoradiation strategies in patients treated with pancreaticoduodenectomy for adenocarcinoma of the pancreas. J Clin Oncol. 1997;15:928–37.
Winter JM, Cameron JL, Campbell KA, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: a single-institution experience. J Gastrointest Surg. 2006;10:1199–210.
Raut CP, Tseng JF, Sun CC, et al. Impact of resection status on pattern of failure and survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Ann Surg. 2007;246:52–60.
de Geus S, Kasumova G, Eskander M, et al. Neoadjuvant therapy affects margins and margins affect all: perioperative and survival outcomes in resected pancreatic adenocarcinoma. HPB. 2017;19:S61.
Katz MHG, Ou FS, Herman JM, et al. Alliance for clinical trials in oncology (ALLIANCE) trial A021501: preoperative extended chemotherapy vs. chemotherapy plus hypofractionated radiation therapy for borderline resectable adenocarcinoma of the head of the pancreas. BMC Cancer. 2017;17:505.
Shaikh T, Ruth K, Scott WJ, et al. Increased time from neoadjuvant chemoradiation to surgery is associated with higher pathologic complete response rates in esophageal cancer. Ann Thorac Surg. 2015;99:270–6.
Kalady MF, de Campos-Lobato LF, Stocchi L, et al. Predictive factors of pathologic complete response after neoadjuvant chemoradiation for rectal cancer. Ann Surg. 2009;250:582–9.
Sloothaak DAM, Geijsen DE, van Leersum NJ, et al. Optimal time interval between neoadjuvant chemoradiotherapy and surgery for rectal cancer. Br J Surg. 2013;100:933–9.
Garcia-Aguilar J, Smith DD, Avila K, et al. Optimal timing of surgery after chemoradiation for advanced rectal cancer: preliminary results of a multicenter, nonrandomized phase II prospective trial. Ann of Surg. 2011;254:97–102.
Verbeke CS. Resection margins in pancreatic cancer. Surg Clin North Am. 2013;93:647–62.
Ethun CG, Kooby DA. The importance of surgical margins in pancreatic cancer. J Surg Oncol. 2016;113:283–8.
Campbell F, Smith RA, Whelan P, et al. Classification of R1 resections for pancreatic cancer: the prognostic relevance of tumour involvement within 1 mm of a resection margin. Histopathology. 2009;55:277–83.
Osipov A, Nissen N, Rutgers J, et al. Redefining the positive margin in pancreatic cancer: impact on patterns of failure, long-term survival and adjuvant therapy. Ann Surg Oncol. 2017;24:3674–82.
Chun YS, Cooper HS, Cohen SJ, et al. Significance of pathologic response to preoperative therapy in pancreatic cancer. Ann Surg Oncol. 2011;18:3601–7.
Murphy JE, Wo JY, Ryan DP, et al. Total neoadjuvant therapy with FOLFIRINOX followed by individualized chemoradiotherapy for borderline resectable pancreatic adenocarcinoma: a phase 2 clinical trial. JAMA Oncol. 2018;4:963–9.
Tachezy M, Gebauer F, Petersen C, et al. Sequential neoadjuvant chemoradiotherapy (CRT) followed by curative surgery vs. primary surgery alone for resectable, non-metastasized pancreatic adenocarcinoma: NEOPA- a randomized multicenter phase III study. BMC Cancer. 2014;14:411 (NCT01900327, DRKS00003893, ISRCTN82191749).
Van Tienhoven G, Versteijne E, Suker M, et al. Preoperative chemoradiotherapy versus immediate surgery for resectable and borderline resectable pancreatic cancer (PREOPANC-1): A randomized, controlled, multicenter phase III trial. J Clin Oncol. 2018;36:LBA4002.
Jang J-Y, Han Y, Lee H, et al. Oncological benefits of neoadjuvant chemoradiation with gemcitabine versus upfront surgery in patients with borderline resectable pancreatic cancer: a prospective, randomized, open-label, multicenter phase 2/3 trial. Ann Surg. 2018;268:215–22.
Acknowledgment
The authors would like to express their gratitude to the patients and caregivers who made this study possible.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
The Fox Chase Cancer Center institution is supported by NCI grant number P30 CA006927. Elizabeth Handorf is supported by a Pfizer grant, unrelated to the current research, and Efrat Dotan has received research support, paid to the institution and unrelated to this published work, from Pfizer, Incyte, Lilly, Merck, Boston Biomedical, GSK, AstraZeneca, Immunomedics, Oncomed, Bayer. Eddie Zhang, Lora Wang, Talha Shaikh, J. Karen Wong, John P. Hoffman, Sanjay Reddy, Harry S. Cooper, Steven J. Cohen, and Joshua E. Meyer have no disclosures to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhang, E., Wang, L., Shaikh, T. et al. Neoadjuvant Chemoradiation Impacts the Prognostic Effect of Surgical Margin Status in Pancreatic Adenocarcinoma. Ann Surg Oncol 29, 354–363 (2022). https://doi.org/10.1245/s10434-021-10219-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-10219-3