
The Bottom Line
In patients with type 2 diabetes mellitus and nephropathy, canagliflozin 100 mg daily reduced the risk of kidney failure when compared with placebo over a mean follow up of 2.6 years.
In patients with type 2 diabetes mellitus and nephropathy, canagliflozin 100 mg daily reduced the risk of kidney failure when compared with placebo over a mean follow up of 2.6 years.
Why is This Important?
-
The global prevalence of end-stage kidney disease is increasing, mainly because of the increase in the number of patients diagnosed with diabetes mellitus (DM). Currently, more than 3 million people worldwide are receiving treatment for kidney failure, and it is predicted that this number will increase to more than 5 million people by 2035. [1, 2]
-
The only currently approved treatment for renoprotection in patients with type 2 diabetes is renin–angiotensin system blockade, which was first shown to be effective 18 years ago. [2]
-
Previous studies suggested a trend for patients with type 2 diabetes and chronic kidney disease in that the use of a sodium–glucose cotransporter 2 (SGLT2) inhibitor reduces the risk of chronic kidney disease progression [3], but none of the previous studies were powered to show a difference.
Facts
-
CREDENCE [4] is a randomized, double blind, placebo-controlled, multicenter trial. A total of 4401 patients with type 2 diabetes and albuminuric chronic kidney disease (urine microalbumin to creatinine ratio > 300 mg/g, eGFR 30–90 ml/min/1.73 m) on maximum tolerated dose of ACEI or ARBs were randomized to receive 100 mg canagliflozin (an oral SGLT2 inhibitor) daily or placebo and were followed for 2.62 years. The average age of participants was 63 years, 33.9% females, 66.6% white, mean duration T2DM 15.8 years, and HgA1c 8.3%, with mean baseline eGFR 56.2 ml/min/1.73 m.
-
Patients with type 1 diabetes, immunosuppression for kidney disease, or a history of dialysis or kidney transplant were excluded.
-
The primary composite outcome (doubling of serum creatinine level, end-stage kidney disease, renal death, or cardiovascular death) was significantly lower in the canagliflozin group than in the placebo group (HR 0.70; 95% CI 0.59 to 0.82, p = 0.00001) NNT = 22 over 2.62 years (95% CI 15–38) (see Fig. 1). Other secondary outcomes, including a composite cardiovascular event outcome, renal outcomes, and hospitalizations for heart failure, were all significantly less frequent in the canagliflozin group.
-
The trial was stopped early for benefit at a planned interim analysis, after 2.62 years of follow-up out of 5.5 years planned.
-
Subgroup analysis showed no significant difference based on patients’ GFR or albumin-to-creatinine ratio at baseline
-
Amputation rates were similar between the groups, with 12.3 versus 11.2 events/1000 person years in the canagliflozin group versus the placebo group. CANVAS-R [3] previously showed increased risk of amputations with 6.3 events in the canagliflozin group versus 3.4 events/1000 patient-years in the placebo group.
Fig. 1 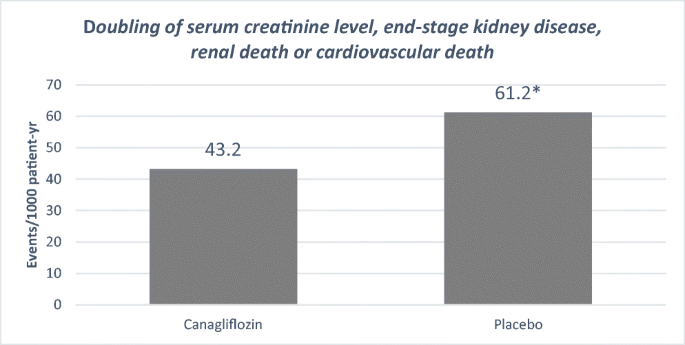
Primary composite outcome

Study Quality and Applicability Considerations
Study internal validity was preserved because of the randomization concealment and blinding of patients and clinicians. Both groups received the same follow-up visits and treatments which minimized performance bias or any other bias that could have potentially been introduced during the study period. The trial was stopped early for benefit based on predefined criteria when the sample size was already achieved. There was low risk of bias potentially introduced by stopping the trial early for benefit. The external validity of the study is preserved as it was a multicenter trial.
References
International Diabetes Federation. IDF diabetes atlas. 8th ed. Brussels: International Diabetes Federation, 2017
Liyanage T, Ninomiya T, Jha V, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet 2015;385:1975-1982
Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017;377:644-657
Perkovic V, Jardine M.J., Neal B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 2019; 380:2295-2306
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The authors have no conflict of interest to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Halalau, A., Fuller, W. & Wheeler, S. Canagliflozin Reduces the Risk of Kidney Failure in Patients with Type 2 Diabetes Mellitus and Nephropathy: The CREDENCE Randomized Trial . J GEN INTERN MED (2021). https://doi.org/10.1007/s11606-020-06216-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11606-020-06216-z