
Abstract
Sixty patients with the diagnosis of idiopathic growth hormone deficiency have been followed till final height was reached, after hGH treatment lasting between 2 and 15 (average 5.4) years. Twenty-six had ‘total’ and 13 ‘partial’ isolated growth hormone deficiency (IGHD); 10 had GHD plus gonadotrophin deficiency (GnD); six had multiple pituitary hormone deficiency (MPHD) and five, labelled ‘transient prepubertal GHD’, had normal responses in the insulin tolerance test when retested after the end of treatment.
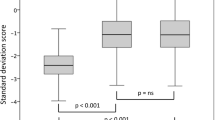
The final height of the patients with IGHD averaged 2.3 SD below the population mean, or 2.0SD below their midparent mean. Half the boys, but only 15% of the girls, ended above the population 3rd centile. There was no difference in final height between those with ‘total’ and ‘partial’ deficiency nor between patients treated prepubertally and those in whom treatment started in early puberty. In the 39 patients with IGHD the correlation of final height with midparent height was 0.72, a figure identical to that occurring in the normal population. Though final height was chiefly influenced by parental height, it was also affected by the degree of smallness when treatment began being lowered by an average of 2.5 cm for every SD that the patient's height at beginning of treatment lay below the average of all IGHD children, parents' heights being allowed for.
Since untreated patients end at about 6 SD below the mean, treatment during the age span represented in these patients recovered 4SD, but failed to recover the remainder. The lost 2 SD may be due to the late start of treatment (averaging 11 years of age even in our prepubertal patients). Our findings emphasise the importance of early diagnosis, so that future patients never drop to 4 or 5 SD below mean height for age, but only to 2 or 3.
Patients with IGHD plus GnD had final heights averaging 1.5 SD below the population mean and those with MPHD 1.0 SD below. This was entirely due to their developing longer legs than the patients with IGHD, the final sitting heights being the same. The long legs were due to treatment with sex steroids being started relatively late. Patients with IGHD who entered puberty spontaneously did so late in time and in the boys pubertal development was normal. In the girls there was a disturbance in the normal relationship of pubertal events and in two menarche never occurred.
Similar content being viewed by others


References
Brook CGD, Gasser T, Werder EA, Prader A, Vanderschueren-Lodewyk MA (1977) Height correlations between parents and mature offspring in normal subjects and in subjects with Turner's, Klinefelter's and other syndromes. Ann Hum Biol 4:17–22
Burns EC, Tanner JM, Preece MA, Cameron N (1981) Growth hormone treatment in children with craniopharyngioma: final growth status in 30 patients. Clin Endocrinol 14: 587–595
Eastman CJ, Lazarus L, Stuart MC, Casey JH (1971) The effect of puberty on growth hormone secretion in boys with short stature and delayed adolescence. Austr New Zealand J Med 2:154–159
Gourmelen M, Pham-Huu-Trung MT, Girard F (1979) Transient partial hGH deficiency in prepubertal children with delay of growth. Paediatr Res 13:221–224
Hartree AS (1966) Separation and partial purification of the protein hormone from human pituitary glands. Biochem J 100:745–761
Hartree AS (1973) Preparation and properties of human growth hormone. In: Stuart Mason A (ed) Human growth hormone. Heinemann, London, pp 1–24
Laron Z, Sarel R, Pertzelan A (1980) Puberty in Laron type dwarfism. Eur J Pediatr 134:79–84
Milner RDG, Preece MA, Tanner JM (1980) Growth in height compared with advancement in skeletal maturity in patients treated with human grwoth hormone. Arch Dis Child 55: 461–466
Penny R, Blizzard RM (1972) The possible influence of puberty on the release of growth hormone in three males with apparent growth hormone deficiency. J Clin Endocrinol Metab 34:82–84
Ranke M, Weber B, Bierich JR (1979) Long-term response to human growth hormone in 36 children with idiopathic growth hormone deficiency. Eur J Pediatr 132:221–238
Rimoin DL, Merimee TJ, Rabinowitz D, McKusick VA (1968) Genetic aspects of clinical endocrinology Rec Prog Horm Res 24:365–437
Tanner JM (1962) Growth at adolescence, 2nd edn Blackwell Scientific Publ. Oxford, pp 28–39
Tanner JM (1978a) Physical growth and development. In: Forfar JO, Arneil GC (eds) Textbook of paediatrics, 2nd edn. Livingstone, Edinburgh, pp 287–290
Tanner JM (1978b) Foetus into man. Open Books, London and Harvard University Press, Cambridge (Mass), pp 167–170
Tanner JM, Whitehouse RH (1975) A note on the bone age at which patients with true isolated growth hormone deficiency enter puberty. J Clin Endocrinol Metab 41:788–790
Tanner JM, Whitehouse RH, Marshall WA, Healy MJR, Goldstein H (1975) Assessment of skeletal maturity and prediction of adult height. Academic Press, London
Tanner JM, Whitehouse RH, Takaishi M (1966) Standards from birth to maturity for height, weight, height velocity and weight velocity: British children, 1965. Arch Dis Child 41:454–471; 613–635
Tanner JM, Whitehouse RH, Hughes PCR, Vince FP (1971) The effects of human growth hormone treatment for 1 to 7 years on the growth of 100 children with growth hormone deficiency, low birthweight, inherited smallness, Turner's syndrome and other complaints. Arch Dis Child 46:745–782
Tanner JM, Whitehouse RH, Hughes PCR, Carter BS (1976) Relative importance of growth hormone and sex steroids for the growth at puberty of trunk length, limb length and muscle width in grwoth hormone deficient children. J Pediatr 89:1000–1008
Zachman M, Prader A, Kind HP, Haflinger H, Budlinger H (1974) Testicular volume during adolescence. Helv Paediatr Acta 29:61–72
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Burns, E.C., Tanner, J.M., Preece, M.A. et al. Final height and pubertal development in 55 children with idiopathic growth hormone deficiency, treated for between 2 and 15 years with human growth hormone. Eur J Pediatr 137, 155–164 (1981). https://doi.org/10.1007/BF00441309
Received:
Issue Date:
DOI: https://doi.org/10.1007/BF00441309