
Abstract
In control subjects and in subjects with primary Raynaud's disease, sudden sound or a mild cool stimulus evokes the pattern of alerting response that includes cutaneous vasoconstriction but vasodilatation in forearm muscle. In control subjects, response habituates on repetition of these stimuli both within experimental sessions and over successive days. However, in subjects with primary Raynaud's disease, the cutaneous vasoconstriction and the muscle vasodilatation persist. We have now tested whether a similar disparity exists for the cutaneous vasoconstriction evoked by venous stasis, a response considered to be a veno-arteriolar reflex mediated by sympathetic fibers, but not requiring transmission through the spinal cord.
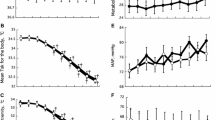
In 10 subjects with primary Raynaud's disease and in 10 matched controls, a sphygmomanometer cuff on the left arm was inflated to 40 mm Hg for 2 minutes, five times on each of three experimental sessions on days 1, 3, and 5. Cutaneous red cell flux (RCF) was recorded from the pulp and dorsum of the left index finger by using a laser Doppler meter; digital vascular conductance (DCVC) was computed as RCF divided by arterial pressure.
The first venous stasis, in session 1, evoked a decrease in pulp and dorsum DCVC in the control and primary Raynaud's subjects. There were no differences between the groups in the magnitudes or durations of these responses. Within session 1, the magnitude of the decrease in DCVC diminished on repetition of venosu stasis in the dorsum in controls and in the pulp in primary Raynaud's subjects. We propose these effects reflected the similar reductions in baseline DCVC over time; there was no change in the duration of the responses.
Repetition of venous stasis had similar effects in both groups of subjects within sessions 2 and 3. Further, judging from the mean of the responses evoked in each Session the decreases evoked in pulp and dorsum DCVC by venous stasis were fully consistent in magnitude and duration over the three sessions in both groups.
These results indicate that the direct constrictor influence of sympathetic fibers upon cutaneous blood vessels is similar in magnitude and similarly reproducible in controls and subjects with primary Raynaud's disease. This reinforces our view that the lack of habituation of the cutaneous vasoconstrictor component of the alerting response in subjects with primary Raynaud's disease reflects impairment of the central neural process of habituation, rather than a peripheral phenomenon, and that this lack of habituation predisposes these subjects to vasospasm.
Similar content being viewed by others


References
Belch JF. The phenomenon, syndrome and disease of Maurice Raynaud.Br J Rheumatol 1990; 29:162–164.
Lewis T. Experiments relating to the peripheral mechanism involved in spasmodic arrest of the circulation in the fingers, a variety of Raynaud's disease.Heart 1929; 15:7–101.
Edwards CM, Marshall JM, Pugh M. Lack of habituation of the pattern of cardiovascular response evoked by sound in subjects with Primary Raynaud's Disease.Clin Sci 1998; 95:249–260.
Edwards CM, Marshall JM, Pugh M. Cardiovascular responses evoked by mid indirect cooling in Primary Raynaud's Disease: the role of Endothelin.Clin Sci 1999, in press.
Henriksen O, Sejrsen P. Local reflex in microcirculation of human cutaneous tissue.Acta Physiol Scand 1976; 98:227–331.
Levick JR, Michel CC. The effects of position and skin temperature on the capillary pressure in the fingers and toes.J Physiol 1978; 274:97–109.
Henriksen O. Local sympathetic reflex mechanism in regulation of blood flow in human subcutaneous adipose tissue.Acta Physiol Scand 1977; Suppl 450:7–45.
Henriksen O, Sejrsen P, Paaske WP, Eickhoff JH. Effect of chronic sympathetic denervation upon the transcapillary filtration rate induced by venous stasis.Acta Physiol Scand 1983; 117:171–176.
Hassan AAK, Tooke JE. Mechanism of the postural vasoconstrictor response in the human foot.Clin Sci 1988; 75:379–387.
Edwards CM, Marshall JM. Cutaneous vascular responsiveness to venous stasis in Primary Raynaud's patients.Clin Autonom Res 1998; 8:72.
Allen E, Brown G. Raynaud's Disease: a critical review of minimal requisites for diagnosis.Am J Med Sci 1932; 183:187–195.
Fitzgerald O, Hess EV, O'Connor GT, Spencer-Green G. Prospective study of the evolution of Raynaud's phenomenon.Am J Med 1988; 84:718–726.
Kallenberg CGM, Wouda AA, Hoet MH, Van Venrooij WJ. Development of connective tissue disease in patients presenting with Raynaud's phenomenon: a six year follow-up with emphasis on the predictive value of anti-nuclear antibodies as directed by immunoblotting.Ann Rheum Dis 1988; 47:634–641.
Grant RT, Bland ET. Observations on arteriovenous anastomoses in human skin and in the bird's foot with special reference to the reaction to cold.Heart 1931; 15:385–407.
Richardson PW, Honour AJ, Fenton GW, Stott FH, Pickering GW. Variation in arterial pressure throughout the day and night.Clin Sci 1964; 26:445–460.
Mohan JS, Marshall JM, Reid HL, Serjeant GR. Daily variability in resting levels of cardiovascular variables in normal subjects and in those with homozygous sickle cell disease.Clin Auton Res 1995; 5:129–134.
Olsen N, Petring OU, Rossing N. Exaggerated postural vasoconstriction reflex in Raynaud's phenomenon.Br Med J 1987; 294:1186–1188.
Engelhart M, Kristensen JK. Local and Central orthostatic sympathetic reflexes in Raynaud's phenomenon.Scand J Clin Lab Invest 1991; 51:191–196.
Kristensen JK, Engelhart M, Neilson T. Laser doppler measurement of digital blood flow regulation in normals and in patients with Raynaud's phenomenon.Acta Dermatovener 1983; 63:43–47.
Myers H, Honig C. Influence of initial resistance on magnitude of response to vasomotor stimuli.Am J Physiol 1969; 216:1429–1436.
Marshall JM. Cardiovascular changes associated with behavioural alerting. In:Cardiovascular Regulation. Eds: Jordan D, Marshall JM. London: Portland Press; 1995:61–76.
Yanagisawa M, Kurihara H, Kimura S, et al. A novel potent vasoconstrictor peptide produced by vascular endothelial cells.Nature (London) 1988; 332:411–415.
Kourembaras S, Marsden P, McQuillan LP, Faller DV. Hypoxia induces endothelin gene expression and secretion in cultured human endothelium.J Clin Invest 1991; 88:1054–1057.
Khan F, Litchfield SJ, McLaren M, Veale DJ, Littleford RC, Belch JJF. Oral L-arginine supplementation and cutaneous vascular responses in patients with primary Raynaud's phenomenon.Arthr Rheum 1997; 40:352–357.
Edwards CM, Marshall JM. Cutaneous vasodilator responses to sodium nitroprusside but not those to acetylcholine may be impaired in patients with Primary Raynaud's Disease.Clin Auton Res 1999, in press.
Saijonmaa O, Ristimaki A, Fyrquist F. Atrial natriuretic peptide, nitroglycerine and nitroprusside reduces basal and stimulated endothelin production from cultured endothelial cells.Biochem Biophys Res Comm 1990; 173:514–520.
Luscher TF, Young ZH, Tschudi M, et al. Interaction between endothelin-1 and endothelium-derived relaxing factor in human arteries and veins.Circ Res 1990; 66:1088–1094.
Warner TD, Allcock GH, Corder R, Vane JR. Use of the endothelin antagonists BQ-123 and PD-142893 to reveal 3 endothelin receptors mediating smooth muscle contraction and the release of EDRF.Br J Pharmacol 1993; 110:777–782.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Edwards, C.M., Marshall, J.M. & Pugh, M. The cutaneous vasoconstrictor response to venous stasis is normal in subjects with primary Raynaud's disease. Clinical Autonomic Research 9, 255–262 (1999). https://doi.org/10.1007/BF02319455
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF02319455