
Abstract
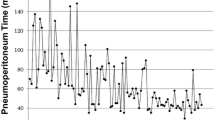
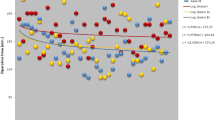
Background: Laparoscopic adrenalectomy (LA) is the procedure of choice for surgical management of most adrenal tumors. LA learning curve (LC) varies among surgeons and may be influenced by factors depending on surgeon, patient, and lesion peculiarities. The aim of this study was to evaluate the LC by multi-dimensional analysis. Methods: Between August 1994 and August 2005, 241 LA were performed in our department. Data were prospectively collected. The pre-operative variables evaluated were patient-related (age, gender, body mass index, co-morbidities) and disease-related (histology, size, and side of lesion). Level of experience of surgical team and surgical approach (anterior, flank, submesocolic routes) were evaluated as well. Flank approached and bilateral procedures were excluded, while submesocolic LA, were collected separately. Operating time (OpT), conversion rate (CR), intra-operative and post-operative complications were evaluated. Patient, surgeon, and procedure-related factors involved in LC were investigated by a multi-factorial logistic regression analysis. Results: Body mass index, side, size, histology, technology improvement, and experience of surgical team, evaluated through the progressive series of surgical procedures, were independent predictors of CR and OpT. The CR for right adrenalectomy was 3% (3 cases) compared to 4.2% for left side (6 cases). The submesocolic approach significantly influenced OpT, but not CR. Mean OpT for right and left LA was 83 and 109 min, respectively. Based on surgical experience increase, the OpT and CR flattened their curves, roughly at 30 and 40 procedures for right and left LA, respectively. Post-operative complications did not change considerably throughout the series. Readmission rate within 30 days was negligible. Conclusions: Manifold factors may affect LC and outcome in LA. Their knowledge may support teaching activities as well as reducing conversion and complication rates.
Similar content being viewed by others

References
Ahlberg G, Kruuna O, Leijonmarck CE, et al. Is the learning curve for laparoscopic fundoplication determined by the teacher or the pupil? Am J Surg 2005, 189: 184–9.
David G, Yoav M, Gross D, Reissman P. Laparoscopic adrenalectomy. Ascending the learning curve. Surg Endosc 2004, 18: 771–3.
Eto M, Harano M, Koga H, Tanaka M, Naito S. Clinical outcomes and learning curve of a laparoscopic adrenalectomy in 103 consecutive cases at a single intitute. Int J Urol 2006, 13: 671–6.
Hunter JG, Sackier JM, Berci G. Training in laparoscopic cholecystectomy. Quantifying the learning curve. Surg Endosc 1994, 8: 28–31.
Schijven MP, Jakimowicz J. The learning curve on the Xitact LS 500 laparoscopy simulator: profiles of performance. Surg Endosc 2004, 18: 121–7.
Tekkis PP, Senagore AJ, Delaney CP, Fazio VW. Evaluation of the learning curve in laparoscpic colorectal surgery: comparison of right-sided and left-sided resections. Ann Surg 2005, 242: 83–91.
Maccabee DL, Jones A, Domreis J, Deveney CW, Sheppard BC. Transition from open to laparoscopic adrenalectomy. The need of advanced training. Surg Endosc 2003, 17: 1566–9.
Lezoche E, Guerrieri M, Feliciotti F, et al. Anterior, lateral and posterior retroperitoneal approaches in endoscopic adrenalectomy. Surg Endosc 2002, 16: 96–9.
Perretta S, Campagnacci R, Guerrieri M, et al. Sub-mesocolic access in laparoscopic left adrenalectomy. Surg Endosc 2005, 19: 977–80.
American Heritage® Dictionary of the English Language, Fourth Edition. New York: Houghton Mifflin Company 2000.
Buchmann P, Dincler S. Learning curve-calculation and value in laparoscopic surgery. Ther Umsch 2005, 62: 69–75.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guerrieri, M., Campagnacci, R., De Sanctis, A. et al. The learning curve in laparoscopic adrenalectomy. J Endocrinol Invest 31, 531–536 (2008). https://doi.org/10.1007/BF03346403
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03346403