
Abstract
Purpose
To describe injuries and outcomes of casualties of Beirut Port Blast treated at a large tertiary care center in Beirut, Lebanon.
Methods
A retrospective observational study assessing the spectrum of injuries, treatment, and medical outcome among casualties of the Beirut Port Blast, immediately after the blast and up to 1 week from the blast to the emergency department of the American University of Beirut Medical Center (AUBMC).
Results
A total of 359 patients were included. Most (n = 343, 95.6%) were adults (> 19 years), and males (56%) with a mean age of 42 ± 20 years. The most frequent mechanism of injury was a penetrating injury (45.7%), followed by other blast-related injuries (30.4%), and blunt injuries (23.4%). The most affected anatomical location were the limbs. Most (n = 217, 60.4%) patients required imaging. The most frequently administered medication was analgesics (38%), followed by anesthetics (35%), antibiotics (31%), tetanus vaccine (31%), and fluids (28%). Blood and blood products were administered in 3.8% of cases. Emergent procedures included endotracheal intubation (n = 18, 5%), surgical airway (n = 3, 0.8%), chest tube insertion (n = 4, 1.1%), thoracotomy (n = 1, 0.3%), and CPR (n = 5, 1.4%). A quarter of patients required surgical operations in the operating room (n = 85, 23.6%) and 18% required noncritical care admissions, 5.3% required critical care admissions, and 2.8% were dead on arrival.
Conclusion
Casualties from this event had significant injuries requiring lifesaving interventions, surgical procedures, and admission to critical care units. High utilization of imaging modalities and of medications from existing stockpiles was also observed.
Similar content being viewed by others

Introduction
On August 4 2020, at precisely at 6:07 pm, a cache of 2750 tons of ammonium nitrate exploded at the Beirut Port minutes after a fireworks warehouse had caught fire, making it the largest non-nuclear explosion of modern times [1]. It was estimated that the blast intensity was equivalent to the detonation of 1000–1500 tons of TNT, about one-tenth the intensity of Hiroshima’s nuclear disaster [2]. This explosion was heard in Syria, Turkey, and Cyprus and it was detected by the United States Geological Survey as a seismic event of 3.3 in magnitude [3].
Ammonium Nitrate (AN) is a detonable substance but is mainly used worldwide for agricultural purposes. It is manufactured as small beads that are cheap and surprisingly safe to handle. During storage, the beads absorb moisture and become clumped together. When the compacted compound is exposed to heat; for instance, a fire, it could result in an explosion [4]. There have been many large accidents, as well as terrorist attacks associated with AN over the last century [5, 6]. One of the most notable explosions before that of the Beirut Port was in 2015 in Tianjin, China where 800 tons of AN lead to the death of 173 people [4].
In Beirut, the devastating catastrophe left behind an even more devastating impact: over 200 fatalities, more than 6000 injured, and 300,000 people displaced with 40% of Beirut city residences shattered [1, 8,9,10]. The World Bank reported over $8 billion in physical and economic losses, all happening in the context of other major crises in the country, on top of ongoing civil unrest, currency devaluation, economic near-collapse, and a COVID-19 pandemic [11, 12].
Sadly, Lebanon has a poorly structured, non-unified EMS and disaster systems even though it is prone to mass casualty incidents being in a zone of conflict and constant political and economic instability. Three major hospitals in the capital were within a 5 mile radius from the explosion and were destroyed, becoming nonfunctional which was equivalent to the loss of almost 500 hospital bed capacity according to the WHO [13]. Other hospitals were overwhelmed with injured patients and The American University of Beirut Medical Center (AUBMC) which is located at 3.4 miles from the Beirut Port was no exception. AUBMC emergency department has a well-established disaster plan and was able to accommodate more than 500 casualties in the first 6 h after the blast. The aim of the study is to describe the blast-related injuries, with an emphasis on initial presentation, medical management, and outcome after hospital discharge.
Materials and methods
Study design and setting
This study is a retrospective observational study that assesses the spectrum of injuries including management, and medical outcomes of casualties of the Beirut Port Blast, who presented on August 4th 2020, immediately after the blast and up to 1 week from the blast to the emergency department of AUBMC.
AUBMC has 358 inpatient beds and receives approximately 55,000 Emergency Department (ED) visits and approximately 25,000 inpatient admissions annually. Pediatric patients account for up to 20% of the ED visits and 17% of hospital admissions. Most ED patients (75%) are covered through private insurance, whereas 23% pay out of pocket, and 2% are covered through governmental insurance.
Selection of participants
All adult and pediatric patients who presented on August 4th 2020, and several days after, and who were flagged as casualties of the Beirut Port Blast were identified through the electronic health system (Epic Systems, Verona, WI, USA), and were included in the study. Patients were excluded if they presented during the same period of the study for complaints that are unrelated to the blast.
Study measures
Demographic data on all adult and pediatric casualties were collected, including age, gender, nationality, and marital status. Information on the patient’s past medical history, including pre-existing disability prior to the blast were also collected. Additionally, all detailed medical information related to the ED presentation, including vital signs, Glasgow coma score, physical exam findings, and treatments provided (fluids, analgesics, anaesthetics, tetanus vaccine, blood, and blood products) were collected. Information on airway management and other procedures that were performed in the ED and the operating room were also retrieved. Information on ED disposition and cause of death were also collected from medical records. To assess injury severity and disability, the modified Rankin score on discharge was calculated.
Statistical analysis
The Statistical Package for Social Sciences (IBM SPSS 25.0) was used for statistical analysis. Frequency and percentage tables represented categorical variables, while means and standard deviations (mean ± SD) were used for continuous variables.
Results
Patient characteristics
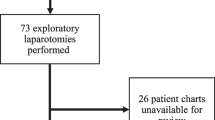
A total of 571 patients were flagged as Beirut blast casualties and their information retrieved from epic. Out of these 212 were excluded due to empty charts with no documentation (42), suture removal [7], wound check [2], cancelled visit [2], incomplete service [2], left without being seen [13], ED visit unrelated to blast (144). The total number of included patients with available documentation was 359.
Most casualties were adults (n = 343, 95.6%), while pediatrics (≥ 19 years of age) accounted for 4.4% (n = 16). The mean age at presentation was 42 ± 20 years, with a median of 39 years (Q1–Q3; 28–53). The vast majority were males (n = 201, 56%), of Lebanese nationality (n = 265, 73.8%), and single (n = 212, 59.1%). Initial vital signs were normal on all patients. Median (Q1–Q3) Systolic Blood Pressure was 126 mmHg (117–136); median diastolic blood pressure was 73 mmHg (67–80); median heart rate was 85 beats per minute (73–97); median respiratory rate is 18 breaths/min [16], and median temperature is 37 C (36.7–37.1).
Injury epidemiology, body system classification, and transport mode
The most frequent mechanism of injury encountered was a penetrating injury, accounting for 45.7% of presentations. This was followed by other blast-related injuries (30.4%) and blunt injuries (23.4%). The most affected anatomical location were the limbs, with the upper extremities more affected than the lower extremities (35.7 vs. 27.6%). This was followed by head and face injuries which accounted for about 20% each, thoracic injuries (8.4%), skin (7%), abdominal and pelvic injuries (5%), and neck injuries (3.1%). Observed injuries were cuts/open wounds (35.1%) and bruises (34.3%) as well as fractures (18.9%) and sprains, strains, and dislocations (6.1%) (Table 1).
Out of those with a known arrival mode (n = 181), 6.5% only were brought to the ED by emergency medical services (EMS), while 31% arrived by non-ems vehicles, and 13.4% came walking. About 13% of patients who arrived at our ED had some sort of prehospital care (3.9% by EMT, 3.3% by nurses and 5.6% of physicians). Two patients were transferred from other hospitals to our facility, but most arrived primarily at our ED (82.7%) (Table 1).
By body system classification, reported injuries were musculoskeletal (56); skin lacerations/foreign bodies (25); head (24) where patients had skull fractures, subarachnoid hemorrhage, brain herniation, and epidural hematoma; Eye Ear Nose and Throat (EENT) (24) where injuries included tympanic membrane rupture, globe rupture, complex facial fractures, others; lung/chest wall injuries [16], Abdominal [9], cardiac [2], Obstetric [2], and spine [4] (Table 2).
Medications, tests, and imaging findings
Most patients (n = 217, 60.4%) required imaging and 64% had positive findings. The most frequently administered medication was analgesics (38%), followed by anesthetics (35%) for rapid sequence intubation, antibiotics (31%), tetanus vaccine (31%), and fluids (28%). Blood and blood products were administered in 3.8% of cases. COVID-19 PCR test was positive in two patients (Table 3).
ED and OR procedures
For patients who underwent an emergent procedure, the most common procedure was endotracheal intubation (n = 18, 5%). Three patients required surgical airway (n = 3, 0.8%). The rest required chest tube insertion for tension pneumothorax decompression (n = 4, 1.1%), one required thoracotomy, and five patients required cardiopulmonary resuscitation. Almost a quarter of patients required surgical operations in the operating room (n = 85, 23.6%), most of which were on the upper extremity, followed by lower extremities, and head/face (Table 4).
ED disposition
Most patients (n = 206, 57.4%) were treated in the ED and discharged home, 18% (n = 65) required noncritical care admissions, 5.3% (n = 19) required critical care admissions, 0.6% (n = 2) transferred to another hospital, and 2.8% (n = 10) were dead on arrival. After admission, 3.6% died in the hospital and 93% of patients were discharged alive.
Injury severity
Most of admitted patients had no pre-existing disability (51%). Upon discharge, 49% had slight disability, 16% moderate disability, and about 0.6% a form of severe disability. There were 0.6% of patients remained in vegetative state. (Table 5).
Pediatric casualties
Out of the total casualties, 16 (4.4%) patients were less than 19 years. 3 (18.6%) patients were intubated, 6 (1.6%) had fractures, 7 (1.9%) had minor wounds, and 2 (0.6%) had major penetrating wounds/burns that are more than 10%. All pediatric patients survived to hospital discharge.
Costs
The mean costs of ED care were $216.88 ± 236.6 with a median of $127.4 (81.43–293.5).
Discussion
The Beirut Port explosion caused considerable destruction and resulted in many fatalities (> 200) and casualties (> 6000) that overwhelmed the emergency medical services and neighboring hospitals, including AUBMC. Prior ammonium nitrate tragic incidents have led over 100 years to similar death toll and injuries. The tragic AN-related incident in 1947 in Texas led to 581 fatalities and 5000 injuries [14]. The more recent 2015 AN detonation in Tianjin, China resulted in 173 fatalities and 798 injuries [14]. The 2013 explosion in West Texas in 2013, resulted in 15 fatalities [14]. The 2001 detonation in Toulouse, France resulted in 31 fatalities and 2242 injuries [14].
Our emergency department, a 42-bed capacity unit, received more than 500 casualties on the first day and subsequent days following the blast, the majority of whom were middle aged single Lebanese males. Most of the patients (57%) were treated and released, 18% admitted to regular floors, 5.3% required critical care admissions, 2.8% were dead on arrival, and 23% required surgical operations.
Our study results show that penetrating injury was the most common mechanism of injury with cuts/open wounds as the most common type of injury. The blast took place in Beirut Port which is in a highly dense urban setting. Injuries were mainly from shattered glass and other flying objects like other explosions where injuries result mainly from shattered glass from windows. Abou-Faraj et al. reported that injuries and death in all Beirut casualties were mainly due to glass shards flying and falling from building facades and interiors causing severe lacerations and abrasions [15]. Similarly, investigations revealed that shattered glass lacerated more than 80% of victims of the 1995 bombing attack of the Alfred P. Murrah Federal Building Bombing in Oklahoma City [15]. This highlights the need for additional building security measures in designing new buildings especially in high-risk regions, such as laminating glass to become blast-resistant and architecturally uncompromising. These new standards of glass that were employed in Oklahoma City can help prevent injuries and save lives in the event of blasts.
The Blast took place in August 2020 during the peak period of the COVID-19 pandemic. Caring for patients during the blast compromised precaution practices that were implemented in most hospitals related to the COVID-19 pandemic, such as removing COVID-19 screening and testing requirements and reduced personal protective equipment (PPE) standards during advanced airway management [16]. Two patients tested positive for covid19 using PCR screening. Around 18.4% of patients had missing PCR results. Nationwide, the COVID-19 positivity rate on August 4, 2020, was 2.7 per 100 tests. One week following the Beirut blast, that positivity rate almost doubled to 5.2 per 100 tests and continued rising till it reached a peak of 10.5 per 100 tests on August 22, 2020, 18 days following the explosion [16]. This reflects both the unexpected nature of disasters and the risks that healthcare providers are faced with during the response to disasters.
The most common primary blast injuries that were observed in casualties included tympanic membrane rupture, globe rupture, pneumothorax, abdominal organ contusion, pericardial tamponade, and brain concussions. These types of primary blast injuries were also observed in casualties in Tianjin and West Texas blasts [14]. Secondary injuries were also common due to the flying debris and fragments resulting in penetrating trauma and injury to head, face, extremity injuries and penetrating eye injuries. Secondary blast injuries were the most observed types of injury (84%) following the Tianjin explosion [14]. Moreover, several victims of the West Texas incident suffered from lacerations and penetrating trauma, with 12% presenting eye injuries [14]. Tertiary blast injuries mainly extremities and pelvic/spine fractures, amputations, concussions, sprains, crush injuries, and open/closed head injuries were also present in casualties treated at out center. This is similar to what occurred in the Tianjin explosion where patients suffered from amputations, fractures, concussions, and sprains [14]. Additionally, 20% of West Texas blast survivors sustained a traumatic head injury or concussion, indicating their high prevalence [14]. Burns and smoke-related inhalational injury were also commonly observed in the Beirut blast.
The vast majority (60%) of patients required X-Ray or computed tomography (CT) imaging. Out of those, 64% had positive findings. Accommodating this large number of patients for imaging and getting results in a timely manner was of paramount importance. This required a close coordination between the radiology department and the ED team to move patients through the radiology suite and to continue to be able to track patients and read studies in a reasonable time. Despite this, some bottlenecks were observed for obtaining imaging studies which required personnel to be dedicated to managing flow of patients to radiology suite. From previous disaster events, the ED had a clear disaster plan and had ready for deployment stockpiles of supplies and medications part of the responses to mass casualty incidents. However, this Beirut blast overwhelmed our resources because of the large influx of casualties. The most used medications included analgesics, tetanus boosters, antibiotics, anesthetics for rapid sequence intubation, fluids, and supplies including suturing kits and splints. Transfusion of blood and blood products was done on 3.8% of our patients. Stockpiling of medications and supplies besides close coordination between the pharmacy, supply department, blood bank, radiology, and other surgical specialties is essential in times of disaster to provide prompt care for casualties in a timely manner and improve survival to hospital discharge.
Our study results show that the estimated ED total costs for caring for casualties in the ED alone exceeded 125,000 USD dollars, which is considered significant during times where the Lebanon’s economy has been struggling due to currency devaluation by 80%, hyperinflation, bank capital control measures, widespread shortage of medications and medical supplies. The cost of Initial World Bank estimates cost the physical damage at US$3·8–4·6 billion and economic losses at $2·9–3·5 billion. The estimated head-count poverty rate in Lebanon increased from 28% in 2019 to 55% in May 2020, with 23% of the population in extreme poverty. These figures increased currently due to continued inflation [12]. Billing practices are usually put on hold during disasters and all casualty care is usually covered by the Ministry of Health at a very low reimbursement rate and in a delayed fashion (after more than 1 year), which reflects the additional financial stress that faced Lebanese hospitals during a COVID-19 pandemic and a financial crisis.
Our study has some limitations. First, it is retrospective and has missing data for collected variables. Data are often missing during disaster events and is largely related to under or lack of documentation. Despite the availability of EHR in our facility, Casualties were registered and immediately treated without requiring computerized order entry or the routine documentation that is done for patient care. Our ED was accustomed to receiving around 120 patients per day and during this blast it received over 300 patients in less than 2 h interval. Another limitation is related to having data on patients from a single center. AUBMC is the largest tertiary care center in Beirut and is within 5 miles from the blast site. It is often the primary receiving hospital for casualties within its catchment area and as such, the study findings reflect patterns of injuries observed at other hospitals during that disaster and expected presentations after a similar blast in a dense urban setting.
Conclusion
In conclusion, despite all the challenges, the emergency department at AUBMC responded well to the huge influx of casualties from Beirut blast due to past experiences with disasters in Lebanon. It is essential to have a disaster plan that is tailored to common threats and to institution capabilities. After the AN blast, patients presented with injuries that required imaging and management in ED or in the operating room. Close coordination with required services including radiology and operating room staff was needed. Stockpiling disaster kits with essential supplies was also important for prompt intervention. Advanced airway management and operative management of injuries mandated the presence of skilled personnel despite the overwhelming nature of the event as secondary triage between facilities would not have been possible since they were all affected within the Beirut Area. Managing patient flow within the institution was also key to allow for increased surge capacity.
References:
El Sayed MJ. Beirut ammonium nitrate explosion: a man-made disaster in times of the COVID-19 pandemic. Disaster Med Public Health Prep. 2020. https://doi.org/10.1017/dmp.2020.451.
Rigby SE, Lodge TJ, Alotaibi S, et al. Preliminary yield estimation of the 2020 Beirut explosion using video footage from social media. Shock Waves. 2020;30:671–5. https://doi.org/10.1007/s00193-020-00970-z.
Clifton K, (2020, August 5) “Beirut explosion one of the largest non-nulcear blasts in history” Evening Standard https://www.standard.co.uk/news/world/beirut-explosion-one-of-largest-blasts-history-a4517646.html
Guglielmi G. Why Beirut’s ammonium nitrate blast was so devastating. Nature. 2020. https://doi.org/10.1038/d41586-020-02361-x.
G.S. Biasutti, History of Accidents in the Explosives Industry, 1980.
Cook MA. The science of high explosives. In: Cook MA, editor. The science of industrial explosives graphics service and supply for IRECO chemicals. Huntington, NY: Robert E. Krieger Publishing Co., Inc.; 1971. p. 13.
Bennett, D., (3 July 2013). West, Texas: The Town That Blew Up, Business Week https://www.bloomberg.com/news/articles/2013-07-03/west-texas-the-town-that-blew-up
Landry, et al. The 2020 blast in the port of beirut: can the lebanese health system “build back better”? BMC Health Serv Res. 2020;20:1040. https://doi.org/10.1186/s12913-020-05906-y.
Devi S. Lebanon faces humanitarian emergency after blast. Lancet (London, England). 2020;396(10249):456.
Strategy&. Beirut Explosion Impact Assessment. Status update #1. Aug 19, 2020. https://www.strategyand.pwc.com/m1/en/beirut-explosion/beirutimpactsssessment-statusupdate1.pdf (accessed Sept 4, 2020)
World Bank. Beirut rapid damage and needs assessment, August 2020. https://www.worldbank.org/en/country/lebanon/publication/beirut-rapid-damage-and-needs-assessment-rdna---august-2020 (accessed July 17, 2021).
Abouzeid M, Habib RR, Jabbour S, Mokdad AH, Nuwayhid I. Lebanon’s humanitarian crisis escalates after the Beirut blast. Lancet. 2020;396(10260):1380–2.
WHO. Lebanon explosion. Update for partners. Aug 18, 2020. https://www.who.int/emergencies/who-lebanon-partners-update-18august2020. pdf?ua=1 (accessed July 4, 2020).
Al-Hajj S. Beirut ammonium nitrate blast: analysis, review, and recommendations. Front Publi Health. 2021;4(9): 657996.
Z.O. Abu-Faraj, Ph.D. Shattered glass is allegedly blamable for most of the victims of beirut’s blast. LinkedIn Pulse. August 26, 2020.
Fares MY, Musharrafieh U, Bizri AR. The impact of the Beirut blast on the COVID-19 situation in Lebanon. Z Gesundh Wiss. 2021;22:1–7.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None declared.
Rights and permissions
About this article

Cite this article
El Zahran, T., Geha, M., Sakr, F. et al. The Beirut Port Blast: spectrum of injuries and clinical outcomes at a large tertiary care center in Beirut, Lebanon. Eur J Trauma Emerg Surg 48, 4919–4926 (2022). https://doi.org/10.1007/s00068-022-02023-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-022-02023-9