
Abstract
Objective
To study the value of objective pressure-volume characteristics for predicting optimal airway pressures and the development of atelectasis and overstretching during a structured lung volume recruitment procedure with subsequent reduction in airway pressures.
Methods
We used a mathematical model of a lung with adjustable characteristics of acute respiratory distress syndrome (ARDS) characteristics. Simulations were performed in five grades of ARDS in the presence of pure alveolar or combined alveolar-small airway closure as well complete or incomplete lung volume recruitability. For each simulation optimal end-expiratory pressure was determined. A static pressure-volume curve was constructed and objective characteristics of this curve calculated. The predictive value of these characteristics for end-expiratory atelectasis, overstretching, and optimal end-expiratory pressure was assessed.
Results
Simultaneous alveolar recruitment and overstretching during inflation were more pronounced than alveolar derecruitment and overstretching during deflation. End-expiratory pressure needed to prevent significant alveolar collapse in severe ARDS resulted in maximal safe tidal volumes that may be insufficient for adequate ventilation using conventional mechanical ventilatory modes. Plateau pressures well below the “upper corner point” (airway pressure where compliance decreases) resulted in significant alveolar overstretching.
Conclusions
A recruitment maneuver followed by subsequent reduction in airway pressure limits end-expiratory atelectasis, overstretching, and pressure. None of the objective characteristics of the pressure-volume curve was predictive for end-expiratory atelectasis, overstretching, or optimal airway pressure.
Similar content being viewed by others


Introduction
The application of positive end-expiratory pressure (PEEP) is aimed at preventing end-expiratory collapse of diseased pulmonary areas to reverse severe hypoxemia resulting from pulmonary shunting, a hallmark of acute respiratory distress syndrome (ARDS). Alveolar and systemic inflammatory responses can be attenuated in patients with ARDS by minimizing overinflation and cyclic recruitment/derecruitment of the lung via a reduction in tidal volume and an increase in PEEP [1]. The pressure-volume (P-V) curve of the respiratory system has long been used as an orientation for setting optimal PEEP in patients with acute lung injury and ARDS [2, 3, 4]. Analysis of the P-V curve has generally been performed by eye, a method shown to be affected by inter- and intraobserver variability [5]. Further confusion has arisen due to the lack of rigorous definitions of terms such as (upper and lower) inflection point. This makes it difficult to compare the results of different studies. Since the inflection of a curve is a mathematical term referring to the point of a function where concavity changes direction, the use of uniform, objective and reproducible parameters to describe a P-V curve has been advocated (Fig. 1) [5, 6].

Example of pressure-volume loop characteristics. (Adapted from [6])
The objective of this study was to gain insight into the physiological implication of the P-V curve, using a mathematical model. We hypothesized that objective and reproducible parameters for describing the P-V curve could be used to define optimal airway pressure during mechanical ventilation.
Methods
The model
We used the mathematical ARDS lung model as described by Hickling [7], which we modified to include air trapping, degree of alveolar recruitability, degree of ARDS severity, and chest wall characteristics. The lungs of a supine patient (15 cm ventrodorsal diameter) were modeled as multiple lung units or “alveoli,” each with an exponential P-V relationship resulting in a progressively decreasing lung compliance with increasing lung volume [8]. The model consisted of 30 compartments, representing “horizontal slices” of lung. Each compartment consisted of 9,000 lung units, which encountered a gravitational superimposed pressure (Ps) from 0 in the ventral compartment (nondependent zone) to a maximal value in the dorsal compartment (dependent zone). Each lung unit was assigned an individual threshold closing pressure (TCP) to simulate either alveolar or small airway collapse and a threshold opening pressure (TOP) to simulate reopening. A transmural pressure (Ptm) below TCP led to the total loss of volume in the case of alveolar collapse and to volume maintenance (air trapping) in the case of small airway collapse.
We performed simulations with alveolar closure only, as well as with 25% of airway closure and 75% of alveolar closure. Small airway volume was ignored. The mechanical characteristics of the chest wall were included in the model, by calculation of chest wall recoil pressure (Pcw) at the instantaneous total lung volume (V), assuming chest wall characteristics adopted from Grassino et al. [9]. Airway pressure was computed (under no-flow conditions) as: Paw=Ptm+Ps+Pcw. The extent of atelectasis (proportional atelectasis) and overstretching (proportional overstretching) was determined at each static lung condition. Proportion atelectasis was determined from the proportion of closed units to total recruitable units. An alveolus was assumed to be overstretched when its volume exceeded 98% of its volume at infinite pressure (achieved at Ptm 23.3 cmH2O). The sequential steps of each simulation were: Ptm was fed into the computer model; the status (open/closed) was determined per alveolus; individual alveolar volume was computed and summed to total lung volume; Pcw and subsequently Paw were determined. Finally, the degree of atelectasis and overstretching were computed.
Simulation of ARDS severity
The degree of ARDS severity was simulated on a linear scale from 0 (healthy lungs) to 100 (severe ARDS). Ps increased with ARDS severity [10]. TOP and TCP had a Gaussian distribution, with mean and standard deviation depending on ARDS severity (Table 1). Values for TOP and TCP were adopted from Crotti et al. [11]. In addition, the degree of lung volume recruitability ranged from 60% to 100%. A nonrecruitable lung unit remained closed at all time. Further details on simulation of ARDS severity are presented in S. 1 of the Electronic Supplementary Material.
Static pressure-volume curve
Starting with all recruitable lung units open, zero end-expiratory pressure (ZEEP) was applied. Then Paw was increased in small steps to 50 cmH2O, and subsequently decreased to ZEEP to determine the static P-V relationship of the model lung. Functional residual capacity (FRC) was determined. The P-V curve shape was characterized by fitting the P-V curve to a predefined sigmoid equation and using this equation to extract the following characteristic points for both inflation and deflation limbs [5, 6]: the lower corner pressure (Pcl), where compliance increased significantly; the pressure at the inflection point (Pinf), where the curve changes from convex to concave; and the upper corner pressure (Pcu), where compliance substantially decreased (Fig. 1).
Sustained inflation and tidal inflation
Safe airway pressures were determined where atelectasis and overstretching were limited. From ZEEP, Paw was increased to the sustained inflation pressure (Psi) when the lungs were deemed adequately recruited (proportional atelectasis less than 2.5%). From Psi the minimal safe end-expiratory pressure (PEEPmin: proportional atelectasis less than 5%) was determined. A tidal inflation was then simulated, increasing Paw to the maximal safe plateau pressure (Pplat,max), defined as the Paw where overstretching was maximal 5%, or where more than 50% of the atelectatic lung units at PEEPmin had been recruited. The volume increase between PEEPmin and Pplat,max was the maximal acceptable tidal volume (VTmax).
Prediction of safe airway pressures
The predictive value of the P-V characteristics obtained from the inflation (I) and deflation (D) limbs as potential determinants of safe airway pressures was investigated in accordance to the atelectasis and overstretching criteria. The inflation characteristics were compared to the obtained Psi. Both inflation and deflation P-V characteristics were compared to the safe minimal (PEEPmin) and maximal (Pplat,max) pressures for tidal ventilation.
Data analysis
Data are presented as means ± standard deviation or as median with interquartile range (IQR) when data were not normally distributed. Means were compared with the Wilcoxon signed rank test; the relationship between variables was assessed by Pearson’s bivariate correlation test. Differences of p<0.05 were considered statistically significant. Precision and bias of P-V characteristics as estimators of safe airway pressures were calculated according to Bland and Altman [12].
Results
Static P-V curve
Figure 2 displays the pressure-volume relationship of the chest wall and lungs in the case of healthy and severely injured lungs. A static P-V curve with an inflation and deflation limb was obtained for all 20 simulations, and the P-V characteristics were calculated (examples in Fig. 3). FRC decreased significantly with increasing ARDS severity (p<0.01, r=−0.98). Average values for Pcl, Pinf, and Pcu for both inflation and deflation limbs are presented in Table 2. These characteristics were found at significantly (p<0.05) lower values on the deflation limb than on the inflation limb, showing the hysteresis of the modeled lungs. There was a positive correlation with ARDS grade for most variables: Pcl of both inflation and deflation limbs, Pinf,I and Pcu,I increased with ARDS grade. Degree of recruitability changed some of the characteristic pressures: with decreasing recruitability, Pcu,D and Pinf,D decreased (r=0.52 and 0.84, respectively) while Pcl,I increased (r=−0.46). Airway closure did not significantly influence the P-V characteristics included in our analysis, although it did affect P-V slope and FRC. With increasing Paw, atelectasis decreased (Table 2). Recruitment of alveolar volume coincided with increased proportional overstretching at Pcu,I. Overstretching was reduced but significant atelectasis appeared as Paw decreased from Pcu,D to Pinf,D with further increased proportional atelectasis and decreased proportional overstretching from Pinf,D to Pcl,D (Table 2). P-V characteristics were also assessed for the transpulmonary pressure (Plungs)−volume curve. Pinf,I for the Plungs-V curve did not differ from the Paw-V curve while Pcl,I was slightly higher. All other Plungs-V characteristics were at slightly lower Paw than their Paw-V counterparts (p<0.05, Table 2). A more detailed presentation of results is given in S. 2 of the Electronic Supplementary Material.

Examples of pressure-volume relationships of the components of the simulated respiratory system for the simulated healthy lung (upper panel) and severe ARDS (lower panel). Dotted line FRC; thick solid line volume above FRC. Pressure for the respiratory system is equivalent to airway pressure, pressure for the modeled lungs is equivalent to transpulmonary pressure, and pressure for the modeled chest wall is equivalent to pleural pressure. In severe ARDS FRC is markedly reduced; the pulmonary P-V curve (Plungs-V) is shifted to the right. The chest wall curve (Pcw-V) had a biphasic shape: exponential at low lung volumes and linear at higher lung volumes. In healthy lungs Pcw-V is linear above FRC, and the nonlinear shape of the total P-V curve (Paw-V) is determined mainly by the lungs component. In severe ARDS the Paw-V curve shape changes, firstly by the nonlinear Pcw-V relationship at low airway pressures on account of the lower FRC, and secondly, by the right-shifted Plungs-V curve

Static pressure-volume curves; healthy lung (left), ARDS grade 50 (center), and grade 100 (right, complete recruitability) with maximal Paw of 60 cmH2O (solid lines). Pressure-volume characteristics (closed circles inflation limb; open circles deflation limb) are determined on this curve. Then from ZEEP inflation is initiated to Psi, with subsequent reduction of Paw to ZEEP (dotted line)
Sustained inflation and tidal inflation
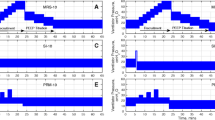
Figure 4 shows the amount of atelectasis and overstretching in three simulations (upper panels) and the course of lung volume (lower panels) during a Paw increase from ZEEP up to Psi and subsequent decrease towards ZEEP. When atelectasis reached the 2.5% criterion at Psi, proportional overstretching was already substantial (12%, IQR 2–28%). Both the volume and atelectasis patterns show the hysteresis of the model lung. Psi (mean Psi=31±12 cmH2O) increased with ARDS grade (p<0.01, r=0.89).

Static pressure-volume curves: healthy lung (left), ARDS grade 50 (center) and grade 100 (right, complete recruitability; lower panel) and development of atelectasis and overstretching (upper panel) during increase in airway pressure from zero to Psi, followed by a reduction in airway pressure to zero. Arrows Direction of pressure change; closed circles PEEPmin, where proportional atelectasis is 5%. In severe ARDS (right) this could not be achieved without marked overstretching; here PEEPmin was defined as the Paw where proportional atelectasis equalled proportional overstretching. With Paw increasing from zeep to Psi, lung volume initially increases as the result of volume increase in alveoli that were open at ZEEP (FRC). With further increase in Paw, increase in lung volume results of a combination of opening of collapsed alveoli and elastic volume increase in open alveoli, at the cost of developing significant overstretching. With decreasing Paw from Psi, initially overstretching is reduced, with further decreasing Paw atelectasis reoccurs. In the example of severe ARDS (right) with increasing Paw during inflation, atelectasis is reduced (A), the volume of reopened lung units abruptly increases toward overstretching (B). When Paw is then decreased, initially alveolar opening is maintained (C) with concomitant overstretching (D). With further Paw reduction some of the lung units collapse (E), while other units reduce their volume but remain open, giving rise to a steep reduction of proportional overstretching (F)
The 5% atelectasis criterion was not achieved without marked overstretching in the most severe ARDS grades. In these cases PEEPmin was defined as the Paw at which proportional atelectasis equaled proportional overstretched. PEEPmin increased with ARDS severity (Fig. 5, upper panel) (p<0.01, r=0.85). Pplat,max initially increased with ARDS severity and subsequently decreased (Fig. 5, upper panel; NS). VTmax decreased with ARDS severity (Fig. 5, lower panel; p<0.01, r=−0.85). In ARDS grades 0 and 25 reopening of end-expiratory collapsed alveoli (maximum 2.5%) was the limiting factor for Pplat,max, whereas in higher ARDS grades Pplat,max was determined by the threshold of overstretching (maximum 5%).

Upper panel Calculated PEEPmin (closed circles) and Pplat,opt (open circles) plotted against simulated ARDS severity. Lower panel Calculated VTmax decrease with increasing simulated ARDS severity
Prediction of safe airway pressures
Psi increased with ARDS severity. At Psi in severe ARDS 77±23% of alveoli were overstretched. Pcl, Pinf, or Pcu and the inflation P-V limb were not correlated well with Psi. Psi varied from 2±0.2 cmH2O below Pinf for the healthy lungs to 1±2 cm above Pcu in the severest ARDS grades. Proportional atelectasis and proportional overstretching found at PEEPmin and various characteristic pressures of the P-V curve are given in Table 2. With exception of Pcu,D there was a significant relationship between PEEPmin and each P-V curve characteristic, although the agreement was poor evidenced by the bias and wide limits of agreement (Table 2). If, on the P-V deflation limb, Paw was reduced to a level equivalent to the Pinf,I, this resulted in proportional atelectasis of 0% (IQR 0–8%) and proportional overstretching of 0% (IQR 0–52%), indicating that Pinf,I was sufficient to prevent significant atelectasis but may not be the lowest pressure possible to obtain this goal. Paw, atelectasis, and overstretching were lower at deflation limb Pcl, Pinf, and Pcu than on equivalent inflation limb characteristics (p<0.05). The correlation between P-V characteristics and Pplat,max was weak; maximal correlation was found for Pcu,I of the Paw-V curve (r=0.65, bias of 13, limits of agreement between 2 and 24 cmH2O) and Pcu of the inflation limb of the Plungs-V curve (r=0.65, bias of 11, limits of agreement between 1 and 22 cmH2O). Pcl, Pinf, and Pcu were neither correlated nor agreed well with Pplat,max.
Discussion
The main finding of this study was that analysis of the static P-V curve does not yield robust predictors for either Psi, PEEPmin, or Pplat,max. The pressure needed to recruit a significant number of previously collapsed alveoli (Psi) increased with increasing severity of ARDS, the minimal PEEP needed to avoid significant atelectasis (PEEPmin) increased, while the maximal safe plateau pressure (Pplat,max) tended to decrease. As a result, the maximal safe tidal volume (VTmax) decreased to levels that may be insufficient for adequate ventilation using conventional mechanical ventilatory modes.
The model
The model used was previously described by Hickling [7, 13]. We modified this model in that we added variability of ARDS severity with threshold opening and closing pressures as well as vertical hydrostatic pressure gradients adapted from the literature [10, 11]. In Hickling’s studies the lungs were completely collapsed at zero Ptm and chest wall effects were neglected. To be able to inflate the lung from ZEEP Paw, rather than transmural ZEEP, and to relate volume changes to changes in airway pressures a simulated chest wall with fixed characteristics was added to the model. Impairment of chest wall elastic properties, time dependency, of recruitment and derecuitment, inertia, resistance, and viscoelastic effects were not modeled. Current knowledge of micromechanics of the injured lung is limited. To construct a mathematical model some assumptions had to be made (e.g., distribution of alveolar and small airway closure, the acceptable amounts of atelectasis, reexpansion of collapsed alveoli, and overstretching). A detailed discussion on these limitations of the model is given as S. 3 in the Electronic Supplementary Material.
Static pressure-volume curve
As is illustrated in Fig. 2, changes in the slope of the Plungs-V curve were found at lung volumes at or below FRC at negative airway pressures. Since the Paw-V curve in the diseased lung shows a clear lower corner point around 20 cmH2O, the lower corner point of the Paw-V curve may represent a chest wall property rather than a lung characteristic. The Pcw-V curve is biphasic with a change in curvature at low lung volumes, as can be seen in Fig. 2. The Plungs-V curves above FRC did not display a symmetrical biphasic shape, whereas the used fit method did assume such a pattern. Quantification of the effect on the accuracy of the fit is beyond the scope of this study, but has been addressed by Harris et al. [6]; calculated values that fall outside the range of available data should be disregarded. In all the calculations that we performed Pcl for the Plungs-V curve was found outside the range of available data and below FRC. This warrants care in the use of Pcl for the Plungs-V curve.
With increasing Paw from ZEEP the initial volume increase was the result of elastic alveolar volume increase rather than volume increase due to opening of previously collapsed alveoli (Fig. 4). In general Pcl has been regarded as the opening pressure of noncompliant, dependent alveoli [2]. This is not supported by our results. Pcl or “lower inflection point” is influenced by a number of factors, including chest wall elastic properties [14]. In our model most alveolar recruitment occurred around Pinf,I. In severe ARDS significant recruitment of collapsed alveoli may take place above Pcu,I, which is thought to be the point at which parts of the lungs become overdistended. In our model alveolar overstretching was present throughout the inflation limb of the P-V curve, depending on the severity of disease, and became substantial in all simulations, except the simulation of the healthy lung between Pinf,I and Pcu,I. Alveolar volume and overstretching is related to absolute Plungs. With increasing ARDS severity Pinf and Pcu shift to higher values and thus are not related to the development of alveolar overstretching. The phenomenon of alveolar recruitment and lung overinflation being observed simultaneously in different parts of the lung after PEEP administration has been demonstrated by computed tomography [15]. A decreasing rate of recruitment during inflation can create an “upper inflection point” which is unrelated to overdistension [7]. Our results show that the inflation characteristics of the Paw-V curve are not uniquely related to alveolar recruitment and overdistension.
Following complete alveolar recruitment decreasing Paw resulted in reduction in lung volume, initially with a decrease in alveolar overstretching while alveoli remained open. In other words, not only the P-V relationship but also pressure-atelectasis and pressure-overstretching display hysteresis. As a consequence a procedure aimed at opening collapsed alveoli may facilitate subsequent reduction in Paw with avoidance of atelectasis, overstretching and high Paw.
Sustained inflation and safe tidal volume
We defined Psi as the inflation pressure needed to obtain less than 2.5% (recruitable) atelectasis and PEEPmin as the end-expiratory pressure at which at most 5% recruitable alveoli were collapsed. These criteria were chosen arbitrarily. It is believed that significant end-expiratory atelectasis plays a role in the development of ventilator induced lung injury [16, 17], and there is evidence that sufficient PEEP should be applied to “keep the lung open” and to prevent tidal recruitment [4, 18, 19, 20]. It is not known, however, what threshold of atelectasis to consider acceptable or safe. In our simulations we arbitrarily regarded 5% end-expiratory atelectasis as the upper limit for defining PEEPmin, having previously simulated a sustained inflation to recruit all but 2.5% of recruitable alveoli. There was no benefit in increasing recruitment pressure above this point since alveoli with high opening pressures also had high closing pressures and thus collapsed during tidal deflation unless very high PEEP was applied.
In severe ARDS high PEEP was needed to prevent significant alveolar collapse. When recruited, the increase in alveolar volume was immediate to a value appropriate for that transalveolar pressure, and when pressure was subsequently reduced below the threshold closing pressure, the alveolus abruptly collapsed [8, 13, 21]. As a result in situations with high threshold closing pressures an open alveolus has a high volume; alveoli with excessive threshold closing pressures were either collapsed or overstretched. The safe maximal plateau pressure seems to be related to the hyperinflation pressure that is relatively constant. In our model, with increasing severity of disease, PEEPmin increased, Pplat,max remained constant, and as a result the VTmax decreased (Fig. 5) to a level at which conventional mechanical ventilation may not be adequate. If the assumptions in our model are correct, this finding suggests that a ventilation mode with smaller tidal volumes may be of benefit, such as high frequency oscillatory ventilation, especially in severe ARDS. Clinical trials are needed to clarify whether this hypothesis is correct.
Prediction of safe airway pressures
It has been proposed to use the P-V curve as a guide for optimal ventilatory settings, with the goal of limiting lung damage related to mechanical ventilation [2, 4]. The shape of this curve is described in ARDS as having three main segments; a segment with minimal compliance, an intermediate segment of maximal compliance, and a final segment where compliance is reduced again [3]. We analyzed the limits of each of these segments (Pcl and Pcu) and a point on the segment with maximal compliance (Pinf) on their value as a guide to adjust ventilator settings.
A pressure 2 cmH2O above Pcl,I has been advocated as a predictor of minimal required PEEP [2, 4], but others have found this point to be a poor predictor of alveolar closure [22]. In our experiments we found median PEEPmin 5 cm above Pcl,I, with limits of agreement between 3 cmH2O below and 13 cmH2O above Pcl,I, depending mainly on the severity of ARDS. In general, correcting for the bias can enhance precision of a measurement method or indicator, but accuracy (the limits of agreement) cannot be enhanced by numerical correction since it represents a nonsystematic error. Intuitively it seems that PEEPmin should be related to maintenance of alveolar volume and hence threshold closing pressures. We therefore expected that deflation limb characteristics would be more related to PEEPmin than would inflation limb characteristics, as is supported in the literature [3, 13]. The good correlation between inflation characteristics and PEEPmin reflects the fact that the range of TOP, Ps, and TCP were related to ARDS severity. The inflation characteristics are mainly determined by TOP, and PEEPmin by TCP and Ps. Alterations in the relationships between TOP, TCP and Ps in the model would have altered the relationship between inflation characteristics and PEEPmin.
Since optimal PEEP and tidal volume, especially in severe ARDS are compromises between atelectasis and overstretching, and pulmonary and cardiovascular function, one single value of best PEEP probably does not exist but rather is represented by a range of pressures. Our findings support the finding that neither the “lower” nor the “upper inflection point” provides reliable information to determine safe ventilator settings in ARDS. Recruitment probably continues throughout the inflation P-V curve and studies of the deflation P-V curve, reinflations after partial deflation, or decremental PEEP trials after a recruitment maneuver are needed to determine optimal open-lung PEEP [23]. Other than lung volume, variables such as cardiac output, shunt, arterial oxygenation [22], blood pressure, and lung compliance [22, 24] may yield superior indicators of optimal airway pressures during mechanical ventilation. Systems that can be used at the bedside and that integrate measurement of respiratory system mechanics and cardiovascular effects of ventilation may aid in the determination of optimal ventilator settings [25, 26].
In conclusion, static P-V characteristics in our model proved to be moderately good estimators of Psi, PEEPmin, and Pplat,max. This may be due mainly to the fact that the effects of alveolar recruitment and collapse, elastic volume changes and alveolar overstretching mutually affect the shape of the P-V curve, and that the individual contribution is lost in the shape of these curves. In contrast to our findings, in clinical studies static P-V curve characteristics was considered to reflect optimal PEEP [4]. This may be caused by the fact that these studies were performed on patients suffering from severe ARDS and hence comparable threshold opening and closing pressures. Our study demonstrates that the relationship between PEEPmin and static P-V curve characteristics, however, is not fixed and depends mainly on severity of ARDS.
References
Ranieri VM, Suter PM, Tortorella C, De Tullio R, Dayer JM, Brienza A, Bruno F, Slutsky AS (1999) Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome: a randomized controlled trial. JAMA 282:54–61
Matamis D, Lemaire F, Harf A, Brun-Buisson C, Ansquer JC, Atlan G (1984) Total respiratory pressure-volume curves in the adult respiratory distress syndrome. Chest 86:58–66
Holzapfel L, Robert D, Perrin F, Blanc PL, Palmier B, Guerin C (1983) Static pressure-volume curves and effect of positive end-expiratory pressure on gas exchange in adult respiratory distress syndrome. Crit Care Med 11:591–597
Amato MB, Barbas CS, Medeiros DM, Schettino GP, Lorenzi FG, Kairalla RA, Deheinzelin D, Morais C, Fernandes EO, Takagaki TY, Carvallo CR (1995) Beneficial effects of the “open lung approach” with low distending pressures in acute respiratory distress syndrome. A prospective randomized study on mechanical ventilation. Am J Respir Crit Care Med 152:1835–1846
Venegas JG, Harris RS, Simon BA (1998) A comprehensive equation for the pulmonary pressure-volume curve. J Appl Physiol 84:389–395
Harris RS, Hess DR, Venegas JG (2000) An objective analysis of the pressure-volume curve in the acute respiratory distress syndrome. Am J Respir Crit Care Med 161:432–439
Hickling KG (1998) The pressure-volume curve is greatly modified by recruitment. A mathematical model of ARDS lungs. Am J Respir Crit Care Med 158:194–202
Salazar E, Knowles JH (1964) An analysis of pressure-volume relationships in the lung. J Appl Physiol 19:97–104
Grassino AE, Roussos C, Macklem PT 1991 Static properties of the chest wall. In: Crystal RG, West JB (ed) The lung: scientific foundations. New Raven, New York, pp 855–867
Pelosi P, D’Andrea L, Vitale G, Pesenti A, Gattinoni L (1994) Vertical gradient of regional lung inflation in adult respiratory distress syndrome. Am J Respir Crit Care Med 149:8–13
Crotti S, Mascheroni D, Caironi P, Pelosi P, Ronzoni G, Mondino M, Marini JJ, Gattinoni L (2001) Recruitment and derecruitment during acute respiratory failure: a clinical study. Am J Respir Crit Care Med 164:131–140
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet I:307–310
Hickling KG (2001) Best compliance during a decremental, but not incremental, positive end-expiratory pressure trial is related to open-lung positive end-expiratory pressure: a mathematical model of acute respiratory distress syndrome lungs. Am J Respir Crit Care Med 163:69–78
Ranieri VM, Brienza N, Santostasi S, Puntillo F, Mascia L, Vitale N, Giuliani R, Memeo V, Bruno F, Fiore T, Brienza A, Slutsky AS (1997) Impairment of lung and chest wall mechanics in patients with acute respiratory distress syndrome: role of abdominal distension. Am J Respir Crit Care Med 156:1082–1091
Puybasset L, Gusman P, Muller JC, Cluzel P, Coriat P, Rouby JJ (2000) Regional distribution of gas and tissue in acute respiratory distress syndrome. III. Consequences for the effects of positive end-expiratory pressure. CT Scan ARDS Study Group. Adult Respiratory Distress Syndrome. Intensive Care Med 26:1215–1227
Sugiura M, McCulloch PR, Wren S, Dawson RH, Froese AB (1994) Ventilator pattern influences neutrophil influx and activation in atelectasis-prone rabbit lung. J Appl Physiol 77:1355–1365
McCulloch PR, Forkert PG, Froese AB (1988) Lung volume maintenance prevents lung injury during high frequency oscillatory ventilation in surfactant-deficient rabbits. Am Rev Respir Dis 137:1185–1192
Lachmann B (1992) Open up the lung and keep the lung open. Intensive Care Med 18:319–321
Gattinoni L, D’Andrea L, Pelosi P, Vitale G, Pesenti A, Fumagalli R (1993) Regional effects and mechanism of positive end-expiratory pressure in early adult respiratory distress syndrome. JAMA 269:2122–2127
Gattinoni L, Pelosi P, Crotti S, Valenza F (1995) Effects of positive end-expiratory pressure on regional distribution of tidal volume and recruitment in adult respiratory distress syndrome. Am J Respir Crit Care Med 151:1807–1814
Staub N, Nagano H, Pearce ML (1967) Pulmonary edema in dogs, especially the sequence of fluid accumulation in lungs. J Appl Physiol 22:227–240
Maggiore SM, Jonson B, Richard JC, Jaber S, Lemaire F, Brochard L (2001) Alveolar Derecruitment at Decremental Positive End-Expiratory Pressure Levels in Acute Lung Injury. Comparison with the lower inflection point, oxygenation, and compliance. Am J Respir Crit Care Med 164:795–801
Hickling KG (2002) Reinterpreting the pressure-volume curve in patients with acute respiratory distress syndrome. Curr Opin Crit Care 8:32–38
Ward NS, Lin DY, Nelson DL, Houtchens J, Schwartz WA, Klinger JR, Hill NS, Levy MM (2002) Successful determination of lower inflection point and maximal compliance in a population of patients with acute respiratory distress syndrome. Crit Care Med 30:963–968
Karason S, Sondergaard S, Lundin S, Stenqvist O (2001) Continuous on-line measurements of respiratory system, lung and chest wall mechanics during mechanic ventilation. Intensive Care Med 27:1328–1339
Markhorst DG, Genderingen HR, Leenhoven T, van Vught AJ (2003) A system for integrated measurement of ventilator settings, lung volume change and blood gases during high-frequency oscillatory ventilation. J Med Eng Technol 27:128–132
Acknowledgements
The authors thank Dr. Keith Hickling for his insights and the many stimulating discussions during the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic Supplementary Material
Rights and permissions
About this article
Cite this article
Markhorst, D.G., van Genderingen, H.R. & van Vught, A.J. Static pressure-volume curve characteristics are moderate estimators of optimal airway pressures in a mathematical model of (primary/pulmonary) acute respiratory distress syndrome. Intensive Care Med 30, 2086–2093 (2004). https://doi.org/10.1007/s00134-004-2446-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-004-2446-7