
Abstract
Purpose
Synchronised volume-targeted ventilation (SIPPV + VTV) attempts to reduce lung injury by standardising volume delivery to the preterm lung. The aim of this study is to describe the regional distribution and variability of ventilation within the preterm lung during SIPPV + VTV.
Methods
Twenty-seven stable, supine, preterm infants with <32 weeks gestation receiving SIPPV + VTV were studied. From each infant, the anterior-to-posterior impedance change due to tidal ventilation (∆Z VT; countless units) was determined during every breath from three, 30-s, electrical impedance tomography recordings. ∆Z VT within the anterior, middle and posterior thirds of the chest were compared using area under the curve analysis. The coefficient of variation (CV) of ∆Z VT in the anterior and posterior hemithoraces, inflation pressure and, where available, V T at airway opening were compared. Infants were sub-grouped by age (≤7 and >7 days), supplemental oxygen requirement and set tidal volume.
Results
In all sub-groups, the middle third of the chest accounted for the greatest ∆Z VT [p < 0.0001, repeated-measures analysis of variance (ANOVA)]. The middle third of the chest constituted a greater relative ∆Z VT in infants aged >7 days compared with ≤7 days (p < 0.0001, repeated-measures ANOVA). Set tidal volume and oxygen requirement did not significantly influence the regional distribution of ∆Z VT. The mean (standard deviation, SD) CV of ∆Z VTANT and ∆Z VTPOST were 30.6% (14.0%) and 31.9% (12.7%). ∆Z VTANT and ∆Z VTPOST expressed greater breath-to-breath variability than the variation in inflation pressure and V T at airway opening (p = 0.012 and p < 0.0001, respectively, paired t-tests).
Conclusion
During SIPPV + VTV the preterm infant exhibits marked breath-to-breath variability in regional ventilation which is influenced by age.
Similar content being viewed by others
Introduction
Preterm lungs are particularly susceptible to ventilator-induced lung injury (VILI) [1, 2], a major contributor to chronic lung disease. VILI is multi-factorial and includes barotrauma, volutrauma, atelectotrauma and biotrauma, all processes exacerbated by ventilation inhomogeneity [3, 4]. Lung-protective ventilation strategies aim to reduce exposure to these factors [5, 6]. Recently, time-cycled, pressure-limited ventilation modes using volume-targeted ventilation (VTV) and synchronised with spontaneous inspiratory effort (SIPPV) have been advocated as a method of reducing volutrauma [7, 8].
During SIPPV + VTV, positive inspiratory pressure (PIP) is automatically adjusted after each inflation to achieve a constant, operator-determined tidal volume, generally derived from measurement of expiratory flow at the airway opening [9]. This method adapts to rapid compliance change but assumes the lung behaves as a single compartment with uniform mechanics [1]. In animal studies, the diseased lung exhibits regional variations in compliance [3, 4, 10, 11]. The resultant pattern of ventilation inhomogeneity can alter on a breath-by-breath basis, leading to regional asynchrony of tidal inflations [12, 13] such that delivered PIP may not be optimal for all regions. This may partly explain the relatively small reductions in morbidity when using SIPPV + VTV in preterm lung disease [7].
Electrical impedance tomography (EIT) is a technique that may overcome some of the practical difficulties of measuring regional lung mechanics at the bedside [14–17]. EIT is simple to use, non-invasive and independent of flow and has been validated against computed tomography, scintigraphy and gas wash-out techniques as a method for determining the relative distribution of ventilation [18–22]. EIT exploits differences in electrical impedance generated by changes in lung tissue conductivity due to tidal variations of gas volume during respiration [15, 18, 21, 23, 24] and has previously been used to describe regional ventilation characteristics in spontaneously breathing [16, 25] and mechanically ventilated infants [22]. Understanding the distribution of ventilation in the preterm lung may improve SIPPV + VTV, thereby reducing respiratory morbidity.
This study aims to describe the gravity-dependent regional distribution and variability of ventilation within the preterm lung during SIPPV + VTV.
Methods
A detailed description can be found in the Electronic Supplementary Material.
Study population
This study was performed in the Neonatal Unit, The Royal Women’s Hospital, Melbourne and was approved by the institution’s Ethics Committee. Informed parental consent was obtained for each infant.
Stable infants with <32 weeks completed gestation at birth, between 24 h and 10 weeks old and receiving SIPPV + VTV (Dräger Babylog 8000+; Drägerwerk, Lübeck, Germany) were eligible for inclusion. Ventilator settings, including the set tidal volume, were determined by the treating clinician and not altered during the study. Infants who were unstable during handling, with fragile skin, fractional inspired oxygen concentration (FiO2) >0.9, refractory hypotension, active air leak syndrome, evolving abdominal pathology, congenital cardiac disease or chromosomal anomaly were excluded.
Measurements and method
Relative impedance change (∆Z) during tidal inflations was measured in supine position using EIT (GeoMFII EIT system; Cardinal Health, Hoechberg, Germany) sampling at 44 Hz [26, 27]. This involved placing 16 pre-trimmed EIT electrodes equidistant around the thorax at nipple level. During a period of quiet rest, and at least 20 min since electrode application, three 2-min recordings, separated by at least 2-min intervals, were taken. The sequence was repeated 20 min later. Airway pressure was simultaneously recorded from the ventilator by the EIT unit. Tidal volume (V T) at the airway opening was integrated from the flow signal acquired from the ventilator at 200 Hz using separate software. During each recording the infant’s chest was video-recorded to detect movement artefact.
Data analysis
The six unfiltered EIT recordings were reviewed in reverse order (accounting for improved electrode conductance with time) using a custom-built program (MatLAB Mathworks Inc., Natick, MA, USA). The first three, 30-s, artefact-free periods were selected, each from separate recordings. To determine ∆Z due to ventilation (∆Z VT), a low-pass filter was applied to the impedance signal at 10 breaths/min above the respiratory rate to eliminate signal noise and cardiac-associated impedance changes [15, 16, 22, 23].
Distribution of tidal ventilation
A functional EIT (fEIT) image was generated from each 30-s recording using the standard deviation of the impedance time course of each individual pixel within the 32 × 32 matrix [26, 28, 29]. The relative ∆Z VT within each of the 32 anterior-to-posterior (gravity-dependent) chest slices was determined by summing all the pixel values within each slice [25, 30]. To simplify interpretation, the area under the curve (AUC) for the slices occupying the anterior, middle and posterior thirds of the chest, and the geometric centre of ventilation within the chest, was calculated [15, 25].
Regional variability of tidal ventilation
In each 30-s period, the PEEP to PIP amplitude (∆P) for all inflations, and the corresponding ∆Z VT amplitude in the anterior (∆Z VTANT) and posterior (∆Z VTPOST) hemithoraces, were determined. To compare the variability of ∆P, ∆Z VTANT and ∆Z VTPOST, the coefficient of variation (CV) in each recording was calculated. The CV of V T at the airway opening within each 30-s recording was also determined if synchrony of the EIT and flow sensor signals could be confirmed for all inflations.
The study population was analysed overall and by the following subgroups: postnatal age (≤7 versus >7 days to delineate differences from pathological or maturational factors), inspired oxygen concentration (FiO2; air versus FiO2 >0.21) and by set VTV (≤3.0 versus >3.0 mL, 3 mL being the median value). A convenience sample of 30 infants was chosen, as differences in ∆Z VT are not known. Data were analysed with t-test or repeated-measures ANOVA with Tukey post-test as appropriate using GraphPad Prism version 4.02 (Graphpad Software, San Diego, CA, USA).
Results
Demographics
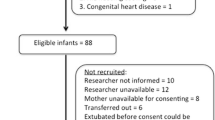
During the study period 325 infants with <32 weeks completed gestation were admitted to our unit. Sixty-three were eligible for study. Twenty-three infants were not approached to participate for the following reasons: investigators unavailable (15), language/social barriers (5), death of a twin (2), severe intracranial pathology (1). Ten families declined consent. One infant died unexpectedly prior to being studied, and equipment failure rendered data unsuitable in a further two instances. Study protocol was completed for 27 clinically stable infants. From the resultant 81 complete sets of EIT data, 3,410 inflations were available for analysis. Artefact rendered 71 inflations unsuitable for analysis within the posterior hemithorax (total 3,339 inflations).
Demographics and ventilation characteristics of the study population are summarised in Table 1. There were 16 infants aged ≤7 days, 15 requiring supplemental oxygen [mean (SD) FiO2 0.36 (0.15)] and 12 whose set VTV was ≤3.0 mL. Fifteen had a PDA considered significant by the attending clinicians. This did not influence the results. No infants had an active air leak, although this had previously occurred in two infants. The mean (SD) endotracheal tube leak was 5.7% (11.6%), with a leak of >10% (maximum 45%) recorded in six infants. The mean set VTV was 2.6 (0.3) mL in the low-V T group and 4.4 (1.5) mL in the high-V T group (p = 0.0005, t-test). There was no significant difference in set VTV by age or need for supplemental oxygen.
Regional distribution of ventilation
Figure 1 illustrates the relative distribution of ventilation in the 32 anterior-to-posterior regions of the chest. In all subgroups the pattern of distribution was similar, with the middle third of the chest accounting for the greatest proportion of tidal ventilation (Table 2). Overall, the mean (SD) AUC of ∆Z VT within the middle third of the chest was 21.3 (10.3) cu compared with 7.3 (2.9) cu and 7.6 (5.0) cu within the anterior and posterior thirds (p < 0.0001, repeated-measures ANOVA). Within each sub-group there was no difference in ∆Z VT within the anterior and posterior thirds of the chest (ANOVA with Tukey post-test).

Relative distribution of tidal ventilation (∆Z VT in countless units; cu) within 32 anterior-to-posterior slices through the thorax (expressed as percentage distance from the most anterior aspect, the sternum). a Data for those infants aged ≤7 days (open diamonds) and >7 days (closed circles) at the time of study. Relative prominence of ∆Z VT in the middle third of the chest was significantly greater in those infants aged >7 days; *p < 0.001, repeated-measures ANOVA with Tukey post-test. There was no difference in ∆Z VT within the anterior and posterior thirds of the chest. b By need for supplemental oxygen (closed circles) and air (open diamonds). c By set V T ≤3.0 mL (open diamonds) and >3.0 mL (closed circles). For oxygen requirement and set V T the pattern of regional distribution of ∆Z VT did not differ between each group. In all sub-groups, ∆Z VT was greatest in the middle third, with no difference in the anterior and posterior thirds; all p < 0.0001, repeated-measure ANOVA post-test analysis. All data mean and standard error of mean (SEM)
Between sub-groups, only age altered the regional distribution pattern of ∆Z VT. There was a relatively greater weighting of ∆Z VT within the middle third of the chest in those infants aged >7 days compared with those ≤7 days; mean [95% CI] difference in ∆Z VT AUC within the middle third was 7.3 [3.1, 11.5] cu (ANOVA with Tukey post-test). These results were not altered by limiting analysis to an equal number of outer pixels in each third of the chest, accounting for the greater inherent pixel weighting in the middle third of the chest and the influence of the large airways in the central regions.
The mean (SD) geometric centre of ventilation was located slightly more anterior in those infants aged ≤7 days at mean (SD) of 49.1% (2.8%) of the distance between the anterior and posterior chest walls compared with 50.6% (3.5%) in those infants aged >7 days with mean [95% CI] difference −1.5% [−2.9%, 0.0%] (p = 0.043, t-test). The geometric centre of ventilation was located a mean [95% CI] 1.7% [0.3%, 3.0%] (t-test) more anterior in the low-set-VTV group compared with high: mean (SD) 48.8% (2.6%) and 50.5% (3.5%), respectively. There was no difference in the geometric centre of ventilation for those infants requiring air or supplemental oxygen: 49.3% (3.4%) and 49.9% (3.0%), respectively.
Breath-to-breath variability of regional tidal ventilation
There was considerable breath-to-breath variability in ∆Z VT in both hemithoraces. The mean (SD) ∆Z VTANT and ∆Z VTPOST CV was 30.6% (14.0%) and 31.9% (12.7%). There was no difference in the CV in each hemithorax (p = 0.302, paired t-test). The corresponding mean (SD) ∆P CV of 23.3% (21.4%) was significantly less than ∆Z VTANT (p = 0.012) and ∆Z VTPOST (p = 0.003), suggesting regional variations in breath-to-breath compliance. Age, inspired oxygen concentration and VTV did not influence the CV of ∆Z VTANT and ∆Z VTPOST.
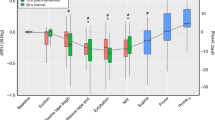
In 15 infants a complete set of synchronised breath-to-breath ∆Z VTANT and ∆Z VTPOST, V T and ∆P data could be collected. In these infants, the variability of V T at the airway opening was less than ∆P, ∆Z VTANT and ∆Z VTPOST (Fig. 2). The mean (SD) CV for V T was 17.0% (8.4%), compared with 23.7% (18.7%) for ∆P (p < 0.0001), 35.3% (15.6%) and 35.2% (14.0%) for ∆Z VTANT and ∆Z VTPOST (p < 0.0001, all paired t-tests). Similar to the entire data set, the variability of ∆Z VTANT and ∆Z VTPOST was not different but both exhibited significantly more breath-to-breath variability than ∆P (p < 0.0001, paired t-tests).

Breath-to-breath variability in tidal ventilation within the anterior (∆Z VTANT; grey bar) and posterior (∆Z VTPOST; dotted bar) hemithoraces, as measured by EIT, compared with tidal volume at the airway opening (V T; black bar) and pressure amplitude (∆P; white bar). Variability of each parameter expressed as the coefficient of variation within each 30-s recording (n = 45). † p = 0.0069 ∆P compared with V T; ‡ p < 0.0001 ∆Z VTANT and ∆Z VTPOST; *p < 0.0001 V T compared with ∆Z VTANT and ∆Z VTPOST (all paired t-tests). All bars mean and SD
Discussion
This study found that describing regional ventilation using EIT was possible in the stable, mechanically ventilated, extremely preterm infant receiving SIPPV + VTV. Ventilation was greatest in the middle third of the chest, with only a slight preference for distribution of ventilation towards the non-dependent lung. We also identified marked breath-to-breath variability in the regional behaviour of tidal ventilation. These findings suggest a complexity in the regional volumetric behaviour of the preterm lung that may not be adequately described by measures of global lung mechanics. Investigating regional variations in ventilation may help in better understanding the mechanics of respiration in the vulnerable extremely preterm lung.
Management of respiratory disease in preterm infants remains challenging. Despite advances in ventilatory techniques, a universally accepted method for optimising ventilation whilst reducing the risk of VILI proves elusive. In part, this is due to difficulties at the bedside in describing the regional interaction between heterogeneous, diseased lung and the mechanical ventilator, which uses algorithms based upon a single compartment, or homogeneous, lung model. EIT is a relatively novel technique, validated against computed tomography and inert gas wash-out methods, for describing regional lung volume in animals and adults [18–21]. It has been used to describe regional ventilation in small cohorts of spontaneously breathing [16, 25] and ventilated infants [30–32]. We have shown that EIT is both feasible and practical for individual assessment of regional ventilation in ventilated extremely preterm infants.
There was marked regional variability in breath-to-breath ∆Z VT in all infants despite using a ventilation modality that aims to adapt to rapid compliance changes and achieve a standardised V T delivery at the airway opening. This was greater than the variability in measured V T at the airway opening and the 5.5 ± 1.5% error of the pneumotachograph [33]. Whether these findings represent rapid regional compliance changes within the lung, inconsistent respiratory effort, untriggered spontaneous inflations or the inherent limitation of the ventilator in correctly predicting an inflation pressure based on a previous breath’s V T measurement [33, 34] cannot be determined from this study. The observation that, in some infants, inflation pressure varied considerably whilst in others it did not, despite regional changes in ∆Z VT, suggests that a combination of all is occurring. Future studies should attempt to assess the infant’s individual breath-by-breath contribution to trans-pulmonary pressures using oesophageal pressure manometry. The regional variability in ∆Z VT has important clinical implications as the preterm lung is particularly vulnerable to VILI from atelectasis, volutrauma and shear forces [35, 36]. Animal studies have shown that rapid changes in regional ventilation and volume state are particularly injurious [3, 4]. Our study suggests that lung mechanics within the mechanically ventilated preterm lung are more complex than described by global measures of expiratory flow at the airway opening [10, 37–40]. In part, this may explain the relatively small reduction in short-term morbidity using SIPPV + VTV [7] and highlights the importance of delivering ventilation targeted to the individual regional mechanical properties present at that point in time.
Regional ventilation has previously been shown to be preferentially distributed to the non-dependent (uppermost) lung in infants and children with abnormal lungs [41] and in animal models of neonatal lung disease [10]. Our study found that most of the ∆Z VT occurred in the middle third of the anterior-posterior axis, with little difference between the most anterior and posterior regions. This was unexpected but may be explained by limitations of EIT. Firstly, EIT is unable to differentiate between the ∆Z VT within alveoli and the large airways. Secondly, EIT creates a single-slice cross-sectional grid of the chest of equally sized pixels, a technique that has been validated against volumetric magnetic resonance imaging (MRI) recordings in an adult [42]. Whether our findings hold true at other levels throughout the preterm thorax cannot be determined by this study. By virtue of the circular chest shape, the middle third contains more pixels than the anterior and posterior thirds and therefore carries a greater weighting of ∆Z VT. Accounting for these limitations did not alter patterns of distribution. Additionally, the geometric centre of ventilation was located near 50% in all subgroups, with the statistical differences identified unlikely to be of clinical significance. The infants in our study had considerably less lung disease than in animal [10, 43] and adult studies [39, 40, 44] that have previously described a gravity-dependent distribution of ventilation and benefits of alveolar recruitment manoeuvres. This may explain our distribution findings but, as illustrated by the high breath-to-breath variability in regional ∆Z VT identified in many infants, does not exclude gravity-dependent ventilation during many of the individual breaths documented. In this observational study, the PEEP was held constant and, in some cases, may have been inadequate for maintenance of alveolar recruitment. Currently, clinicians have few tools to guide optimal PEEP delivery. EIT may assist in determining whether, and when, an infant may benefit from additional PEEP or alveolar recruitment manoeuvres.
The relative increase in the weighting of ∆Z VT observed within the middle third of the chest in the infants aged >7 days suggests differing lung mechanics from those ≤7 days, as evident by the higher set V T in this older cohort. The age-related medial prominence in the distribution of ∆Z VT is interesting. Whether this represents age-related effects of prolonged ventilation, such as distension of major airways, a more heterogeneous parenchymal lung injury or a combination of many factors, cannot be determined from this study. An increase in set V T with age was noted in a retrospective study of extremely preterm infants requiring SIPPV + VTV [45]. An increase in airway calibre and alveolar dead-space with age was postulated as the explanation. Our findings are consistent with this hypothesis. In newborn animal models, maturational differences in airway development and lung perfusion are known to occur [46]. It was surprising that we did not observe differences in the distribution of ∆Z VT between the air and oxygen cohorts. Oxygen requirement is an accepted proxy for severity of lung disease [47], and in adults and animal models the degree of lung disease has been shown to alter the distribution of lung volume [10, 11, 44]. Our limited sample size precluded more detailed sub-group analysis, but our results suggest that future research in this population should consider the potential for maturational changes in tidal ventilation as well as degree of lung disease.
Previous clinical studies of the infant lung have been limited to healthy, spontaneously breathing infants [16, 25] or small cohorts of infants ventilated using various strategies [32]. Applying the regional ventilation findings of these studies to the ventilated preterm infant may not be appropriate. Our study involved preterm infants who were physiologically stable, recovering from their hyaline membrane disease, ventilated for recurrent apnoea or weaning. Many had minimal lung disease, and much of the potential for severe VILI was likely to have already occurred. Equally, it should not be assumed that our findings readily translate to the early phase of hyaline membrane disease. Rather, our findings should be considered as a description of the behaviour of the ‘normal’ ventilated preterm lung and serve as a reference for future EIT studies during the initial phases of acute preterm lung disease.
This study has several other limitations not previously mentioned. As the absolute regional tidal volumes during each EIT recording are unknown, interpretation of the functional EIT data between subjects should be limited to comparison of the pattern of relative distribution of ventilation within the chest. The EIT unit used was limited to a single analogue input channel, precluding our ability to record ∆Z VT, pressure and flow simultaneously. Due to the small thoracic circumference, ensuring precise, equidistant lead placement around the preterm infant’s chest can be difficult and result in less precise spatial interpretation of the regions of interest. EIT is also extremely sensitive to movement. We attempted to limit the effect of movement artefact by using video, though it is still possible that small movements have not been excluded. All our infants were studied in supine position to standardise any gravitational effects on ventilation. Our results may have been different if these infants had been studied in other positions. Prone positioning is known to improve regional ventilation in adults [48]. In ventilated preterm infants, turning of the head results in left-to-right regional differences in ventilation [32]. Study of the effects of posture on regional ventilation in ventilated preterm infants is warranted.
Conclusions
There appears to be a maturational change in the regional distribution of ventilation, likely due to large airway changes. More importantly, regional lung mechanics in the ventilated preterm lung are complex and often vary significantly between breaths, even with the use of ventilation modalities which attempt to standardise lung mechanics. This variability was not identified by monitoring at the airway opening. Regional lung mechanics should be considered in the development of future lung-protective ventilation strategies.
Abbreviations
- ∆Z :
-
Relative impedance change
- ∆Z VT :
-
Relative impedance change with tidal ventilation
- ∆P :
-
Pressure amplitude
- CI:
-
Confidence interval
- CV:
-
Coefficient of variation
- EIT:
-
Electrical impedance tomography
- FiO2 :
-
Fraction of inspired oxygen
- IQR:
-
Inter-quartile range
- PEEP:
-
Positive end-expiratory pressure
- PIP:
-
Positive inspiratory pressure
- RDS:
-
Respiratory distress syndrome
- SD:
-
Standard deviation
- SIPPV:
-
Synchronised intermittent positive pressure ventilation
- VTV:
-
Volume-targeted ventilation
- V T :
-
Tidal volume
References
Dreyfuss D, Saumon G (1998) Ventilator-induced lung injury: lessons from experimental studies. Am J Respir Crit Care Med 157:294–323
Slutsky AS (1999) Lung injury caused by mechanical ventilation. Chest 116:9S–15S
Halter JM, Steinberg JM, Schiller HJ, DaSilva M, Gatto LA, Landas S, Nieman GF (2003) Positive end-expiratory pressure after a recruitment maneuver prevents both alveolar collapse and recruitment/derecruitment. Am J Respir Crit Care Med 167:1620–1626
Schiller HJ, Steinberg J, Halter J, McCann U, DaSilva M, Gatto LA, Carney D, Nieman G (2003) Alveolar inflation during generation of a quasi-static pressure/volume curve in the acutely injured lung. Crit Care Med 31:1126–1133
Rouby JJ, Ferrari F, Bouhemad B, Lu Q (2007) Positive end-expiratory pressure in acute respiratory distress syndrome: should the ‘open lung strategy’ be replaced by a ‘protective lung strategy’? Crit Care 11:180
Lista G, Colnaghi M, Castoldi F, Condo V, Reali R, Compagnoni G, Mosca F (2004) Impact of targeted-volume ventilation on lung inflammatory response in preterm infants with respiratory distress syndrome (RDS). Pediatr Pulmonol 37:510–514
McCallion N, Davis PG, Morley CJ (2005) Volume-targeted versus pressure-limited ventilation in the neonate. Cochrane Database Syst Rev:CD003666
Abubakar K, Keszler M (2005) Effect of volume guarantee combined with assist/control vs synchronized intermittent mandatory ventilation. J Perinatol 25:638–642
Keszler M, Abubakar K (2004) Volume guarantee: stability of tidal volume and incidence of hypocarbia. Pediatr Pulmonol 38:240–245
Pellicano A, Tingay DG, Mills JF, Fasulakis S, Morley CJ, Dargaville PA (2009) Comparison of four methods of lung volume recruitment during high frequency oscillatory ventilation. Intensive Care Med 35(11):1990–1998
Pelosi P, Goldner M, McKibben A, Adams A, Eccher G, Caironi P, Losappio S, Gattinoni L, Marini JJ (2001) Recruitment and derecruitment during acute respiratory failure: an experimental study. Am J Respir Crit Care Med 164:122–130
Hough JL, Grant CA, Pham TMT, Schibler A (2009) The use of filling indices to determine temporal characteristics of lung filling in ventilated preterm infants. J Paediatr Child Health 45:A23
Grant CA, Fraser JF, Dunster KR, Schibler A (2009) The assessment of regional lung mechanics with electrical impedance tomography: a pilot study during recruitment manoeuvres. Intensive Care Med 35:166–170
Schibler A, Calzia E (2008) Electrical impedance tomography: a future item on the “Christmas Wish List” of the intensivist? Intensive Care Med 34:400–401 (author reply 583)
Frerichs I, Dargaville PA, Dudykevych T, Rimensberger PC (2003) Electrical impedance tomography: a method for monitoring regional lung aeration and tidal volume distribution? Intensive Care Med 29:2312–2316
Frerichs I, Schiffmann H, Oehler R, Dudykevych T, Hahn G, Hinz J, Hellige G (2003) Distribution of lung ventilation in spontaneously breathing neonates lying in different body positions. Intensive Care Med 29:787–794
Putensen C, Wrigge H, Zinserling J (2007) Electrical impedance tomography guided ventilation therapy. Curr Opin Crit Care 13:344–350
Frerichs I, Hinz J, Herrmann P, Weisser G, Hahn G, Dudykevych T, Quintel M, Hellige G (2002) Detection of local lung air content by electrical impedance tomography compared with electron beam CT. J Appl Physiol 93:660–666
Hinz J, Hahn G, Neumann P, Sydow M, Mohrenweiser P, Hellige G, Burchardi H (2003) End-expiratory lung impedance change enables bedside monitoring of end-expiratory lung volume change. Intensive Care Med 29:37–43
Hinz J, Neumann P, Dudykevych T, Andersson LG, Wrigge H, Burchardi H, Hedenstierna G (2003) Regional ventilation by electrical impedance tomography: a comparison with ventilation scintigraphy in pigs. Chest 124:314–322
Victorino JA, Borges JB, Okamoto VN, Matos GF, Tucci MR, Caramez MP, Tanaka H, Sipmann FS, Santos DC, Barbas CS, Carvalho CR, Amato MB (2004) Imbalances in regional lung ventilation: a validation study on electrical impedance tomography. Am J Respir Crit Care Med 169:791–800
Riedel T, Kyburz M, Latzin P, Thamrin C, Frey U (2009) Regional and overall ventilation inhomogeneities in preterm and term-born infants. Intensive Care Med 35:144–151
Adler A, Amyot R, Guardo R, Bates JH, Berthiaume Y (1997) Monitoring changes in lung air and liquid volumes with electrical impedance tomography. J Appl Physiol 83:1762–1767
van Genderingen HR, van Vught AJ, Jansen JR (2004) Regional lung volume during high-frequency oscillatory ventilation by electrical impedance tomography. Crit Care Med 32:787–794
Schibler A, Yuill M, Parsley C, Pham T, Gilshenan K, Dakin C (2009) Regional ventilation distribution in non-sedated spontaneously breathing newborns and adults is not different. Pediatr Pulmonol 44:851–858
Barber DC (1989) A review of image reconstruction techniques for electrical impedance tomography. Med Phys 16:162–169
Brown BH (2003) Electrical impedance tomography (EIT): a review. J Med Eng Technol 27:97–108
Barber DC (1989) A sensitivity method for electrical impedance tomography. Clin Phys Physiol Meas 10:368–371
Hinz J, Gehoff A, Moerer O, Frerichs I, Hahn G, Hellige G, Quintel M (2007) Regional filling characteristics of the lungs in mechanically ventilated patients with acute lung injury. Eur J Anaesthesiol 24:414–424
Frerichs I, Hahn G, Schiffmann H, Berger C, Hellige G (1999) Monitoring regional lung ventilation by functional electrical impedance tomography during assisted ventilation. Ann NY Acad Sci 873:493–505
Dunlop S, Hough J, Riedel T, Fraser JF, Dunster K, Schibler A (2006) Electrical impedance tomography in extremely prematurely born infants and during high frequency oscillatory ventilation analyzed in the frequency domain. Physiol Meas 27:1151–1165
Heinrich S, Schiffmann H, Frerichs A, Klockgether-Radke A, Frerichs I (2006) Body and head position effects on regional lung ventilation in infants: an electrical impedance tomography study. Intensive Care Med 32:1392–1398
Roske K, Foitzik B, Wauer RR, Schmalisch G (1998) Accuracy of volume measurements in mechanically ventilated newborns: a comparative study of commercial devices. J Clin Monit 14:413–420
Jaecklin T, Morel DR, Rimensberger PC (2007) Volume-targeted modes of modern neonatal ventilators: how stable is the delivered tidal volume? Intensive Care Med 33:326–335
Attar MA, Donn SM (2002) Mechanisms of ventilator-induced lung injury in premature infants. Semin Neonatol 7:353–360
Lista G, Castoldi F, Fontana P, Reali R, Reggiani A, Bianchi S, Compagnoni G (2006) Lung inflammation in preterm infants with respiratory distress syndrome: effects of ventilation with different tidal volumes. Pediatr Pulmonol 41:357–363
Hickling KG (1998) The pressure-volume curve is greatly modified by recruitment. A mathematical model of ARDS lungs. Am J Respir Crit Care Med 158:194–202
Downie JM, Nam AJ, Simon BA (2004) Pressure-volume curve does not predict steady-state lung volume in canine lavage lung injury. Am J Respir Crit Care Med 169:957–962
Rouby JJ, Puybasset L, Cluzel P, Richecoeur J, Lu Q, Grenier P (2000) Regional distribution of gas and tissue in acute respiratory distress syndrome. II. Physiological correlations and definition of an ARDS Severity Score. CT Scan ARDS Study Group. Intensive Care Med 26:1046–1056
Puybasset L, Gusman P, Muller JC, Cluzel P, Coriat P, Rouby JJ (2000) Regional distribution of gas and tissue in acute respiratory distress syndrome. III. Consequences for the effects of positive end-expiratory pressure. CT Scan ARDS Study Group. Adult Respiratory Distress Syndrome. Intensive Care Med 26:1215–1227
Davies H, Kitchman R, Gordon I, Helms P (1985) Regional ventilation in infancy. Reversal of adult pattern. N Engl J Med 313:1626–1628
Yang F, Patterson RP (2007) The contribution of the lungs to thoracic impedance measurements: a simulation study based on a high resolution finite difference model. Physiol Meas 28:S153–S161
Frerichs I, Dargaville PA, van Genderingen H, Morel DR, Rimensberger PC (2006) Lung volume recruitment after surfactant administration modifies spatial distribution of ventilation. Am J Respir Crit Care Med 174:772–779
Albaiceta GM, Taboada F, Parra D, Luyando LH, Calvo J, Menendez R, Otero J (2004) Tomographic study of the inflection points of the pressure–volume curve in acute lung injury. Am J Respir Crit Care Med 170:1066–1072
Keszler M, Nassabeh-Montazami S, Abubakar K (2009) Evolution of tidal volume requirement during the first 3 weeks of life in infants <800 g ventilated with volume guarantee. Arch Dis Child Fetal Neonatal Ed 94:F279–F282
Glenny RW, Bernard SL, Luchtel DL, Neradilek B, Polissar NL (2007) The spatial-temporal redistribution of pulmonary blood flow with postnatal growth. J Appl Physiol 102:1281–1288
Tingay DG, Mills JF, Morley CJ, Pellicano A, Dargaville PA (2006) The deflation limb of the pressure-volume relationship in infants during high-frequency ventilation. Am J Respir Crit Care Med 173:414–420
Langer M, Mascheroni D, Marcolin R, Gattinoni L (1988) The prone position in ARDS patients. A clinical study. Chest 94:103–107
Acknowledgments
The authors wish to thank Brenda Argus and Stephanie Tan-Kristanto for their assistance with this study. D.G.T. is supported by a National Health and Medical Research Council Clinical Research Fellowship (Grant ID 491286).
Conflict of interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Armstrong, R.K., Carlisle, H.R., Davis, P.G. et al. Distribution of tidal ventilation during volume-targeted ventilation is variable and influenced by age in the preterm lung. Intensive Care Med 37, 839–846 (2011). https://doi.org/10.1007/s00134-011-2157-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-011-2157-9