
Abstract
Purpose
The effect of capacity strain in an ICU on the timing of end-of-life decision-making is unknown. We sought to determine how changes in strain impact timing of new do-not-resuscitate (DNR) orders and of death.
Methods
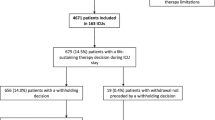
Retrospective cohort study of 9891 patients dying in the hospital following an ICU stay ≥72 h in Project IMPACT, 2001–2008. We examined the effect of ICU capacity strain (measured by standardized census, proportion of new admissions, and average patient acuity) on time to initiation of DNR orders and time to death for all ICU decedents using fixed-effects linear regression.
Results
Increases in strain were associated with shorter time to DNR for patients with limitations in therapy (predicted time to DNR 6.11 days for highest versus 7.70 days for lowest quintile of acuity, p = 0.02; 6.50 days for highest versus 7.77 days for lowest quintile of admissions, p < 0.001), and shorter time to death (predicted time to death 7.64 days for highest versus 9.05 days for lowest quintile of admissions, p < 0.001; 8.28 days for highest versus 9.06 days for lowest quintile of census, only in closed ICUs, p = 0.006). Time to DNR order significantly mediated relationships between acuity and admissions and time to death, explaining the entire effect of acuity, and 65 % of the effect of admissions. There was no association between strain and time to death for decedents without a limitation in therapy.
Conclusions
Strains in ICU capacity are associated with end-of-life decision-making, with shorter times to placement of DNR orders and death for patients admitted during high-strain days.

Similar content being viewed by others
References
Garland A, Connors AF (2007) Physicians’ influence over decisions to forego life support. J Palliat Med 10:1298–1305
Turnbull AE, Krall JR, Ruhl AP, Curtis JR, Halpern SD, Lau BM, Needham DM (2014) A scenario-based, randomized trial of patient values and functional prognosis on intensivist intent to discuss withdrawing life support. Crit Care Med 42:1455–1462
Barnato AE, Berhane Z, Weissfeld LA, Chang CC, Linde-Zwirble WT, Angus DC, Robert Wood Johnson Foundation ICU End-of-Life Peer Group (2006) Racial variation in end-of-life intensive care use: a race or hospital effect? Health Serv Res 41:2219–2237
Quill CM, Ratcliffe SJ, Harhay MO, Halpern SD (2014) Variation in decisions to forgo life-sustaining therapies in US ICUs. Chest 146:573–582
Hart JL, Harhay MO, Gabler NB, Ratcliffe SJ, Quill CM, Halpern SD (2015) Variability among US intensive care units in managing the care of patients admitted with preexisting limits on life-sustaining therapies. JAMA Intern Med 175:1019–1026
Halpern SD (2011) ICU capacity strain and the quality and allocation of critical care. Curr Opin Crit Care 17:648–657
Wagner J, Gabler NB, Ratcliffe SJ, Brown SE, Strom BL, Halpern SD (2013) Outcomes among patients discharged from busy intensive care units. Ann Intern Med 159:447–455
Gabler NB, Ratcliffe SJ, Wagner J, Asch DA, Rubenfeld GD, Angus DC, Halpern SD (2013) Mortality among patients admitted to strained intensive care units. Am J Respir Crit Care Med 188:800–806
Brown SE, Rey MM, Pardo D, Weinreb S, Ratcliffe SJ, Gabler NB, Halpern SD (2014) The allocation of intensivists’ rounding time under conditions of intensive care unit capacity strain. Am J Respir Crit Care Med 190:831–834
Nelson JE, Angus DC, Weissfeld LA, Puntillo KA, Danis M, Deal D, Levy MM, Cook DJ, Critical Care Peer Workgroup of the Promoting Excellence in End-of-Life Care Project (2006) End-of-life care for the critically ill: a national intensive care unit survey. Crit Care Med 34:2547–2553
Cremer R, Hubert P, Grandbastien B, Moutel G, Leclerc F, GFRUP’s study group on forgoing treatments (2011) Prevalence of questioning regarding life-sustaining treatment and time utilisation by forgoing treatment in francophone PICUs. Intensive Care Med 37:1648–1655
Jensen HI, Ammentorp J, Erlandsen M, Ording H (2011) Withholding or withdrawing therapy in intensive care units: an analysis of collaboration among healthcare professionals. Intensive Care Med 37:1696–1705
Wagner J, Halpern SD (2012) Deferred admission to the intensive care unit: rationing critical care or expediting care transitions? Arch Intern Med 172:474–476
Strauss MJ, LoGerfo JP, Yeltatzie JA, Temkin N, Hudson LD (1986) Rationing of intensive care unit services. An everyday occurrence. JAMA 255:1143–1146
Hua M, Halpern SD, Gabler NB, Wunsch H (2015) Effect of ICU strain on time to death in the intensive care unit. B105. Improving patient experience in critical care. Am J Respir Crit Care Med 191:A3764–A3764
Cook SF, Visscher WA, Hobbs CL, Williams RL, Project IMPACT Clinical Implementation Committee (2002) Project IMPACT: results from a pilot validity study of a new observational database. Crit Care Med 30:2765–2770
Higgins TL, Teres D, Copes WS, Nathanson BH, Stark M, Kramer AA (2007) Assessing contemporary intensive care unit outcome: an updated mortality probability admission model (MPM0-III). Crit Care Med 35:827–835
Zimmerman JE, Kramer AA, McNair DS, Malila FM (2006) Acute physiology and chronic health evaluation (APACHE) IV: hospital mortality assessment for today’s critically ill patients. Crit Care Med 34:1297–1310
Kerlin MP, Harhay MO, Vranas KC, Cooney E, Ratcliffe SJ, Halpern SD (2014) Objective factors associated with physicians’ and nurses’ perceptions of intensive care unit capacity strain. Ann Am Thorac Soc 11:167–172
Prendergast TJ, Claessens MT, Luce JM (1998) A national survey of end-of-life care for critically ill patients. Am J Respir Crit Care Med 158:1163–1167
Sprung CL, Cohen SL, Sjokvist P, Baras M, Bulow HH, Hovilehto S, Ledoux D, Lippert A, Maia P, Phelan D, Schobersberger W, Wennberg E, Woodcock T, Ethicus Study Group (2003) End-of-life practices in European intensive care units: the Ethicus Study. JAMA 290:790–797
Preacher KJ, Hayes AF (2004) SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput 36:717–731
Krull JL, MacKinnon DP (2001) Multilevel modeling of individual and group level mediated effects. Multivar Behav Res 36:249–277
Imai K, Keele L, Tingley D (2010) A general approach to causal mediation analysis. Psychol Methods 15:309–334
Quenot JP, Rigaud JP, Prin S, Barbar S, Pavon A, Hamet M, Jacquiot N, Blettery B, Herve C, Charles PE, Moutel G (2012) Impact of an intensive communication strategy on end-of-life practices in the intensive care unit. Intensive Care Med 38:145–152
Curtis JR, Treece PD, Nielsen EL, Gold J, Ciechanowski PS, Shannon SE, Khandelwal N, Young JP, Engelberg RA (2016) Randomized trial of communication facilitators to reduce family distress and intensity of end-of-life care. Am J Respir Crit Care Med 193:154–162
Garrouste-Orgeas M, Tabah A, Vesin A, Philippart F, Kpodji A, Bruel C, Gregoire C, Max A, Timsit JF, Misset B (2013) The ETHICA study (part II): simulation study of determinants and variability of ICU physician decisions in patients aged 80 or over. Intensive Care Med 39:1574–1583
Stelfox HT, Hemmelgarn BR, Bagshaw SM, Gao S, Doig CJ, Nijssen-Jordan C, Manns B (2012) Intensive care unit bed availability and outcomes for hospitalized patients with sudden clinical deterioration. Arch Intern Med 172:467–474
Uy J, White DB, Mohan D, Arnold RM, Barnato AE (2013) Physicians’ decision-making roles for an acutely unstable critically and terminally ill patient. Crit Care Med 41:1511–1517
Dzeng E, Colaianni A, Roland M, Chander G, Smith TJ, Kelly MP, Barclay S, Levine D (2015) Influence of institutional culture and policies on do-not-resuscitate decision making at the end of life. JAMA Intern Med 175:812–819
Acknowledgments
Dr. Hua is supported by a Mentored-Training Research Grant from the Foundation in Anesthesia Education and Research. Dr. Halpern is supported by a grant from The Otto Haas Charitable Trust. Nicole B. Gabler: None. Dr. Wunsch is supported by Award Number K08AG038477 from the National Institute On Aging.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest. The funding sources played no role in the design and conduct of the study, collection, management, analysis, and interpretation of the data, or preparation, review, or approval of the manuscript.
Additional information
Take-home message: Increases in ICU strain are associated with shorter time to placement of treatment limitations and shorter time to death for patients dying in the ICU. These data suggest that physicians are capable of performing more efficiently and expediting the delivery of end-of-life care for critically ill patients.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hua, M., Halpern, S.D., Gabler, N.B. et al. Effect of ICU strain on timing of limitations in life-sustaining therapy and on death. Intensive Care Med 42, 987–994 (2016). https://doi.org/10.1007/s00134-016-4240-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-016-4240-8