
Abstract
Background
Peroral cholangioscopy-directed lithotripsy (PC-directed lithotripsy) has been successfully used for the treatment of difficult bile duct stones, including Mirizzi syndrome (MS). However, long-term outcome and risk factors for stone recurrence after PC-directed lithotripsy have not yet been elucidated. The aim of this study was to assess the outcomes of long-term follow-up after PC-directed lithotripsy and to clarify risk factors predicting stone recurrence.
Methods
One hundred twenty-two consecutive patients with difficult bile duct stones, including MS type II (McSherry classification system), were included in the study.
Results
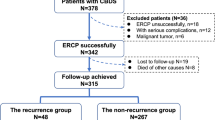
Successful stone removal was achieved in 117 (95.9%) of the 122 patients treated with PC-directed lithotripsy. Of these 117 patients, reliable follow-up information for a median period of 5.5 years (range = 0.19–16.6) was obtained for 111 patients (94.9%) in whom stone type was classified into one of the following three categories: (1) MS type II (47 patients); (2) impacted stones (45 patients); and (3) large stones (≥20 mm in short diameter, 19 patients). Bile duct stone recurrence was observed in 18 patients (16.1%), of whom 4 had MS type II, 9 had impacted stones, and 5 had large stones. Statistical analysis showed that dilated bile duct diameter greater than or equal to 20 mm was the only risk factor for stone recurrence.
Conclusions
PC-directed lithotripsy used for the treatment of difficult bile duct stones, including MS type II and impacted stones, and is found to be safe at long-term follow-up. Dilated bile duct diameter is the only risk factor for stone recurrence. Careful follow-up is indispensable, particularly for patients with dilated bile ducts.






Similar content being viewed by others


Abbreviations
- PC:
-
Peroral cholangioscopy
- MS:
-
Mirizzi syndrome
- ML:
-
Mechanical lithotripsy
- ERCP:
-
Endoscopic retrograde cholangiopancreatography
References
Chang WH, Chu CH, Wang TE, Chen MJ, Lin CC (2005) Outcome of simple use of mechanical lithotripsy of difficult common bile duct stones. World J Gastroenterol 11(4):593–596
Pramod KG, Rakesh KT, Ahuja V, Govind KM, Batra Y (2004) Predictors of unsuccessful mechanical lithotripsy and endoscopic clearance of large bile duct stones. Gastrointest Endosc 59(6):601–605
Chung SC, Leung JW, Leong HT, Li AK (1991) Mechanical lithotripsy of large common bile duct stones using a basket. Br J Surg 78(12):1448–1450
Cipolletta L, Costamagna G, Bianco MA, Rotondano G, Piscopo R, Mutignani M, Marmo R (1997) Endoscopic mechanical lithotripsy of difficult common bile duct stones. Br J Surg 84:1407–1409
Arya N, Nelles SE, Haber GB, Kim YI, Kortan PK (2004) Electrohydraulic lithotripsy in 111 patients: a safe and effective therapy for difficult bile duct stones. Am J Gastroenterol 99:2330–2334
Neuhaus H, Hoffmann W, Zillinger C, Classen M (1993) Laser lithotripsy of difficult bile duct stones under direct visual control. Gut 34:415–421
England RE, Martin DF (1997) Endoscopic management of Mirizzi’s syndrome. Gut 40:272–276
Binmoeller KF, Thonke F, Soehendra N (1993) Endoscopic treatment of Mirizzi’s syndrome. Gastrointest Endosc 39:532–536
McSherry CK, Festenberg H, Virshup M (1982) The Mirizzi syndrome: suggested classification and surgical therapy. Surg Gastroenterol 1:219–225
Tsuyuguchi T, Saisho H, Ishihara T, Yamaguchi T, Onuma EK (2000) Long-term follow-up after treatment of Mirizzi syndrome by peroral cholangioscopy. Gastrointest Endosc 52(5):639–644
Piraka C, Shah RJ, Awadallah NS, Langer DA, Chen YK (2007) Transpapillary cholangioscopy-directed lithotripsy in patients with difficult bile duct stones. Clin Gastroenterol Hepatol 5:1333–1338
Ando T, Tsuyuguchi T, Okugawa T, Saito M, Ishihara T, Yamaguchi T, Saisho H (2003) Risk factors for recurrent bile duct stones after endoscopic papillotomy. Gut 52:116–121
Hintze RE, Adler A, Veltzke W, Ramani NV, Abou-Rebyeh H (1997) Management of traction wire fracture complicating mechanical basket lithotripsy. Endoscopy 29(9):883–885
Binmoeller KF, Bruckner M, Thonke F, Soehendra N (1993) Treatment of difficult bile duct stones using mechanical, electrohydraulic and extracorporeal shock wave lithotripsy. Endoscopy 25(3):201–206
Adamek HE, Maier M, Jakobs R, Wessbecher FR, Neuhauser T, Riemann JF (1996) Management of retained bile duct stones: a prospective open trial comparing extracorporeal and intracorporeal lithotripsy. Gastrointest Endosc 44(1):40–47
Chen YK, Pleskow DK (2007) SpyGlass single-operator peroral cholangiopancreatoscopy system for the diagnosis and therapy of bile-duct disorders: a clinical feasibility study (with video). Gastrointest Endosc 65:832–841
Hui CK, Lai KC, Ng M, Wong WM, Yuen MF, Lam SK, Lai CL, Wong BC (2003) Retained common bile duct stones: a comparison between biliary stenting and complete clearance of stones by electrohydraulic lithotripsy. Aliment Pharmacol Ther 17:289–296
Leung JW, Chung SC, Mok SD, Li AK (1988) Endoscopic removal of large common bile duct stones in recurrent pyogenic cholangitis. Gastrointest Endosc 34:238–241
Johnson LW, Sehon JK, Lee WC, Zibari GB, McDonald JC (2001) Mirizzi’s syndrome: experience from a multi-institutional review. Am Surg 67:11–14
Kwon AH, Inui H (2007) Preoperative diagnosis and efficacy of laparoscopic procedures in the treatment of Mirizzi syndrome. J Am Coll Surg 204:409–415
Disclosures
Drs. Tsuyuguchi, Sakai, Sugiyma, Ishihara, and Yokosuka have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tsuyuguchi, T., Sakai, Y., Sugiyama, H. et al. Long-term follow-up after peroral cholangioscopy-directed lithotripsy in patients with difficult bile duct stones, including Mirizzi syndrome: an analysis of risk factors predicting stone recurrence. Surg Endosc 25, 2179–2185 (2011). https://doi.org/10.1007/s00464-010-1520-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-010-1520-1