
Abstract
Purpose
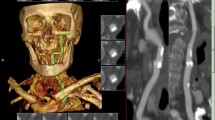
To evaluate the incidence of vascular lesions in the head and neck by magnetic resonance angiography (MRA), and investigate the factors correlated with severe stenosis.
Methods
Elective coronary artery bypass grafting (CABG) was performed in 413 patients at our center between May 1997 and April 2001. We used MRA to detect head and neck vascular lesions, then evaluated the occlusive lesions and determined their prevalence.
Results
Neck MRA was performed in 335 patients and head MRA was performed in 335 patients. We found ≥60% stenosis or total occlusion of the extracranial carotid and vertebral artery in 43 patients (12.8%) and ≥60% stenosis or occlusion of the intracranial carotid and basilar artery, or stenosis accompanied by poor peripheral perfusion or occlusion of the cerebral arteries in 45 patients (13.4%). Occlusive lesions of the neck were significantly correlated with mean age, peripheral vascular disease (PVD), and old myocardial infarction. Occlusive lesions of the brain were significantly correlated with age, hypertension, PVD, and left main trunk disease.
Conclusions
We found an equal incidence of intracranial and extracranial vascular lesions. Thus, searching for intracranial lesions is just as important as searching for extracranial lesions before CABG.
Similar content being viewed by others

Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Ohuchi, S., Kawazoe, K., Izumoto, H. et al. Head and Neck Magnetic Resonance Angiography Before Coronary Artery Bypass Grafting. Surg Today 35, 432–435 (2005). https://doi.org/10.1007/s00595-004-2973-4
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s00595-004-2973-4