
Abstract
Background
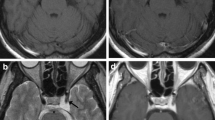
Cavernous sinus hemangiomas (CaSHs) are rare vascular lesions in the cavernous sinus(CS). Gamma Knife radiosurgery (GKS) provides a treatment modality alternative to microsurgery. This study was conducted to describe a new classification of CaSHs based on their magnetic resonance (MR) imaging findings and determine the efficacy and safety of GKS in a large series of CaSH patients.
Methods
From April 2007 to November 2012, 53 patients harboring CaSHs were treated using Leksell Gamma Knife model C (before April 2012) or Perfexion (from May 2012 ) at the Gamma Knife Center of Huashan Hospital. Of the 53 patients, 15 with definitive histopathologic diagnoses after surgery, 38 were diagnosed based on their MR imaging findings. There were 15 male and 38 female patients with a mean age of 52 (range, 25–76) years old. The characteristics of MR images of CaSHs were their extremely high homogeneous intensity on T2-weighted and FLAIR images: as bright as cerebrospinal fluid signal. According to the relationship between the carotid line and their location, CaSHs were classified into three types: the intrasellar, parasellar and mixed type. The mean volume of the tumors was 13.2 ± 8.2 cm3 (range, 1–41 cm3). A mean marginal dose of 13.3 Gy (range, 8–15 Gy) was directed to the 49 %–64 % isodose line (mean 53 %).
Results
Of the 53 tumors, 6 (11 %) were classified as intrasellar type. Eight (15 %) were parasellar type and the other 39 cases(74 %) mixed type. The mean radiological and clinical follow-up time of this study was 24 (range, 2–67 months) and 34 months (range, 2–73 months), respectively. The tumor control rate was 100 %. The mean tumor volume reduction was 79.5 % (range, 16.5 %–100 %) compared with the pre-GKS volume. Six months after GKS, MR imaging revealed an average of 60.2 % tumor volume reduction (range, 16.5 %–89.2 %). Twenty-nine cases (55 %) showed a >80 % tumor volume decrease. Neurologically, only two of these patients showed clinical deterioration, and 33 patients demonstrated an obvious improvement in ocular or endocrine disorders. At last follow-up, there were no more complications related to GKS, and none of the tumors progressed.
Conclusions
Our study showed that GKS is a useful and safe therapeutic method for CaSHs as both a primary and adjuvant treatment. The new classification of CaSHs may help predict their clinical course during tumor development and treatment response after GKS. Further studies with long-term follow-up and larger numbers of cases are necessary to optimize the treatment conditions and verify the benefit of this treatment.





Similar content being viewed by others


References
Anqi X, Zhang S, Jiahe X, Chao Y (2014) Cavernous sinus cavernous hemangioma: imaging features and therapeutic effect of Gamma Knife radiosurgery. Clin Neurol Neurosurg 127:59–64
Chou CW, Wu HM, Huang CI, Chung WY, Guo WY, Shih YH, Lee LS, Pan DH (2010) Gamma Knife surgery for cavernous hemangiomas in the cavernous sinus. Neurosurgery 67:611–616, discussion 616
Flickinger JC, Kondziolka D, Lunsford LD (1999) Dose selection in stereotactic radiosurgery. Neurosurg Clin N Am 10:271–280
Fraser JF, Mass AY, Brown S, Anand VK, Schwartz TH (2008) Transnasal endoscopic resection of a cavernous sinus hemangioma: technical note and review of the literature. Skull Base 18:309–315
Gliemroth J, Missler U, Sepehrnia A (2000) Cavernous angioma as a rare neuroradiologic finding in the cavernous sinus. J Clin Neurosci 7:554–557
Gonzalez LF, Lekovic GP, Eschbacher J, Coons S, Porter RW, Spetzler RF (2006) Are cavernous sinus hemangiomas and cavernous malformations different entities? Neurosurg Focus 21:e6
Grosu AL, Nieder C (2006) Stereotactic fractionated radiotherapy for recurrent capillary hemangioma of the cavernous sinus. Strahlenther Onkol 182:179–182
He K, Chen L, Zhu W, Mao Y (2014) Magnetic resonance standard for cavernous sinus hemangiomas: proposal for a diagnostic test. Eur Neurol 72:116–124
Ivanov P, Chernov M, Hayashi M, Nakaya K, Izawa M, Murata N, Kubo O, Ujiie H, Muragaki Y, Nakamura R, Iseki H, Hori T, Takakura K (2008) Low-dose Gamma Knife radiosurgery for cavernous sinus hemangioma: report of 3 cases and literature review. Minim Invasive Neurosurg 51:140–146
Iwai Y, Yamanaka K, Nakajima H, Yasui T (1999) Stereotactic radiosurgery for cavernous sinus cavernous hemangioma–case report. Neurol Med Chir (Tokyo) 39:288–290
Jamjoom AB (1996) Response of cavernous sinus hemangioma to radiotherapy: a case report. Neurosurg Rev 19:261–264
Jinhu Y, Jianping D, Xin L, Yuanli Z (2008) Dynamic enhancement features of cavernous sinus cavernous hemangiomas on conventional contrast-enhanced MR imaging. AJNR Am J Neuroradiol 29:577–581
Khan AA, Niranjan A, Kano H, Kondziolka D, Flickinger JC, Lunsford LD (2009) Stereotactic radiosurgery for cavernous sinus or orbital hemangiomas. Neurosurgery 65:914–918, discussion 918
Kida Y, Kobayashi T, Mori Y (2001) Radiosurgery of cavernous hemangiomas in the cavernous sinus. Surg Neurol 56:117–122, discussion 122–113
Kuo JS, Chen JC, Yu C, Zelman V, Giannotta SL, Petrovich Z, MacPherson D, Apuzzo ML (2004) Gamma Knife radiosurgery for benign cavernous sinus tumors: quantitative analysis of treatment outcomes. Neurosurgery 54:1385–1393, discussion 1393–1384
Li P, Ren H, Zhang S, Wang W (2012) Clinical results of Gamma Knife surgery for cavernous sinus hemangiomas. J Neurosurg 117(Suppl):89–95
Linskey ME, Sekhar LN (1992) Cavernous sinus hemangiomas: a series, a review, and an hypothesis. Neurosurgery 30:101–108
Lombardi D, Giovanelli M, de Tribolet N (1994) Sellar and parasellar extra-axial cavernous hemangiomas. Acta Neurochir (Wien) 130:47–54
Mendonca JL, Viana SL, Matsumine M, Silva RF, Viana MA, Freitas FM (2004) Cavernous angioma of the cavernous sinus: imaging findings. Arq Neuropsiquiatr 62:1004–1007
Meyer FB, Lombardi D, Scheithauer B, Nichols DA (1990) Extra-axial cavernous hemangiomas involving the dural sinuses. J Neurosurg 73:187–192
Nakamura N, Shin M, Tago M, Terahara A, Kurita H, Nakagawa K, Ohtomo K (2002) Gamma Knife radiosurgery for cavernous hemangiomas in the cavernous sinus. Report of three cases. J Neurosurg 97:477–480
Namba S (1983) Extracerebral cavernous hemangioma of the middle cranial fossa. Surg Neurol 19:379–388
Ohata K, El-Naggar A, Takami T, Morino M, El-Adawy Y, El-Sheik K, Inoue Y, Hakuba A (1999) Efficacy of induced hypotension in the surgical treatment of large cavernous sinus cavernomas. J Neurosurg 90:702–708
Peker S, Kilic T, Sengoz M, Pamir MN (2004) Radiosurgical treatment of cavernous sinus cavernous haemangiomas. Acta Neurochir (Wien) 146:337–341, discussion 340
Puca A, Colosimo C, Tirpakova B, Lauriola L, Di Rocco F (2004) Cavernous hemangioma extending to extracranial, intracranial, and orbital regions. Case report. J Neurosurg 101:1057–1060
Sawamura Y, de Tribolet N (1990) Cavernous hemangioma in the cavernous sinus: case report. Neurosurgery 26:126–128
Shi J, Wang H, Hang C, Pan Y, Liu C, Zhang Z (1999) Cavernous hemangiomas in the cavernous sinus. Case reports. Surg Neurol 52:473–478, discussion 478–479
Song SW, Kim DG, Chung HT, Paek SH, Han JH, Kim YH, Kim JW, Kim YH, Jung HW (2014) Stereotactic radiosurgery for cavernous sinus hemangiomas. J Neurooncol 118:163–168
Suri A, Ahmad FU, Mahapatra AK (2007) Extradural transcavernous approach to cavernous sinus hemangiomas. Neurosurgery 60:483–488, discussion 488–489
Suzuki Y, Shibuya M, Baskaya MK, Takakura S, Yamamoto M, Saito K, Glazier SS, Sugita K (1996) Extracerebral cavernous angiomas of the cavernous sinus in the middle fossa. Surg Neurol 45:123–132
Thompson TP, Lunsford LD, Flickinger JC (2000) Radiosurgery for hemangiomas of the cavernous sinus and orbit: technical case report. Neurosurgery 47:778–783
Toyoda K, Oba H (2011) Diagnostic imaging of hemangiomas in the brain. Brain Nerve 63:5–15
Wang X, Liu X, Mei G, Dai J, Pan L, Wang E (2012) Phase II study to assess the efficacy of hypofractionated stereotactic radiotherapy in patients with large cavernous sinus hemangiomas. Int J Radiat Oncol Biol Phys 83:e223–e230
Wang X, Mei G, Liu X, Dai J, Pan L, Wang E (2012) The role of stereotactic radiosurgery in cavernous sinus hemangiomas: a systematic review and meta-analysis. J Neurooncol 107:239–245
Yamamoto M, Kida Y, Fukuoka S, Iwai Y, Jokura H, Akabane A, Serizawa T (2010) Gamma Knife radiosurgery for hemangiomas of the cavernous sinus: a seven-institute study in Japan. J Neurosurg 112:772–779
Yao Z, Feng X, Chen X, Zee C (2006) Magnetic resonance imaging characteristics with pathological correlation of cavernous malformation in cavernous sinus. J Comput Assist Tomogr 30:975–979
Zhou LF, Mao Y, Chen L (2003) Diagnosis and surgical treatment of cavernous sinus hemangiomas: an experience of 20 cases. Surg Neurol 60:31–36, discussion 36–37
Acknowledgments
The authors are very grateful to Prof. Ying Mao, Wei Zhu, and Liang Chen, Department of Neurosurgery, Huashan Hospital, for their support in the surgical cases. The authors also thank Dr. Wenjing Cao, Lichen Wei, Hua Jiang, and Yanchao Zhu, Department of Radiology, Shanghai Gamma Hospital, for the pre- and postradiosurgical MR images for most cases. Finally, the authors express their sincere gratitude to Yongyan Ni for her outstanding help with the schematic work in Fig. 2.
Disclosure
All authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this paper.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This comprehensive review of a large cohort of patients harboring cavernous sinus pathology is highly valuable for neurosurgeons. As the authors point out, based on MRI one can be reasonably sure about the pathology, and I would add that in any case the residual uncertainty has only little impact on management. Very large tumors may benefit from partial, latero/superior partial resection, but in case of hemangiomas this is even less attractive than for meningiomas: these highly vascular tumors can pose a surgical challenge even for partial resection attempts.
On the other hand, it is precisely the high vascularity that makes hemangiomas so well suited to Gamma Knife treatment: this has been a well-established experience of radiosurgeons with other tumors, e.g., glomus jugulare tumors. This review underlines the importance of considering radiosurgery as an integral part of the neurosurgical armamentarium and the collaboration between microsurgical and radiosurgical approaches.
Andras Kemeny
Sheffield, UK
Rights and permissions
About this article

Cite this article
Tang, X., Wu, H., Wang, B. et al. A new classification and clinical results of Gamma Knife radiosurgery for cavernous sinus hemangiomas: a report of 53 cases. Acta Neurochir 157, 961–969 (2015). https://doi.org/10.1007/s00701-015-2417-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-015-2417-5