
Abstract
Background
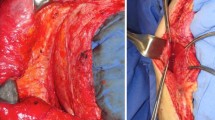
The ideal surgical treatment for complicated ventral hernias remains elusive. Traditional component separation provides local advancement of native tissue for tension-free closure without prosthetic materials. This technique requires an extensive subcutaneous dissection, with the division of perforating vessels predisposing to skin flap necrosis and complicated wound infections. The laparoscopic separation of components provides a minimally invasive alternative to open techniques, while eliminating the potential space and subsequent complications of large skin flaps. We report our initial experience with a minimally invasive component separation with early postoperative outcomes.
Methods
We retrospectively reviewed the medical records of all patients who underwent a minimally invasive component separation for abdominal wall reconstruction during the resection of an infected prosthetic. Pertinent details included baseline demographics, reason for contamination, operative technique and details, postoperative morbidity, mortality, and recurrence rates.
Results
Between August 2006 and January 2007, seven patients were identified who underwent a laparoscopic component separation. There were four males and three females, with a mean age of 54 years (range 34–84), mean American Society of Anesthesiologist (ASA) score of 3.2 (range 3–4), and mean body mass index (BMI) of 37 kg/m2 (range 30–45). The reason for contamination included exposed non-healing mesh (6) and contaminated fluid collection around the mesh (1). Residual defect size following the removal of all prosthetics was 338 cm2 (range 187–450). The mean operative time was 185 min (range 155–220). Laparoscopic component separation enabled tension-free primary fascial reapproximation in all patients. Three postoperative complications occurred, including superficial surgical site infection (1), respiratory failure (1), and hematoma (1). There was no mortality in this series. During an average follow-up period of 4.5 months, no recurrences were identified.
Conclusions
This study shows that a minimally invasive component separation is feasible and can result in minimal postoperative wound morbidity in these complex patients. Long-term follow-up is necessary to evaluate the outcomes with respect to recurrence rates.


Similar content being viewed by others

References
Burger JW, Luijendijk RW, Hop WC, Halm JA, Verdaasdonk EG, Jeekel J (2004) Long-term follow-up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann Surg 240:578–583; discussion 583–585
Millikan KW (2003) Incisional hernia repair. Surg Clin North Am 83:1223–1234
Sauerland S, Schmedt CG, Lein S, Leibl BJ, Bittner R (2005) Primary incisional hernia repair with or without polypropylene mesh: a report on 384 patients with 5-year follow-up. Langenbecks Arch Surg 390:408–412
Luijendijk RW, Hop WCJ, van den Tol MP, de Lange DCD, Braaksma MMJ, Ijzermans JNM, Boelhouwer RU, de Vries BC, Salu MKM, Wereldsma JCJ, Bruijninckx CMA, Jeekel J (2000) A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med 343:392–398
Lomanto D, Iyer SG, Shabbir A, Cheah WK (2006) Laparoscopic versus open ventral hernia mesh repair: a prospective study. Surg Endosc 20:1030–1035
Novitsky YW, Porter JR, Rucho ZC, Getz SB, Pratt BL, Kercher KW, Heniford BT (2006) Open preperitoneal retrofascial mesh repair for multiply recurrent ventral incisional hernias. J Am Coll Surg 203:283–289
Cobb WS, Harris JB, Lokey JS, McGill ES, Klove KL (2003) Incisional herniorrhaphy with intraperitoneal composite mesh: a report of 95 cases. Am Surg 69:784–787
van Geffen HJAA, Simmermacher RKJ, van Vroonhoven TJM, van der Werken C (2005) Surgical treatment of large contaminated abdominal wall defects. J Am Coll Surg 201:206–212
Ramirez OM, Ruas E, Dellon AL (1990) “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg 86:519–526
Alaedeen DI, Lipman J, Medalie D, Rosen MJ (2007) The single-staged approach to the surgical management of abdominal wall hernias in contaminated fields. Hernia 11:41–45
DiBello JN Jr, Moore JH Jr (1996) Sliding myofascial flap of the rectus abdominus muscles for the closure of recurrent ventral hernias. Plast Reconstr Surg 98:464–469
Lowe JB, Garza JR, Bowman JL, Rohrich RJ, Strodel WE (2000) Endoscopically assisted “components separation” for closure of abdominal wall defects. Plast Reconstr Surg 105:720–729; quiz 730
de Vries Reilingh TS, van Goor H, Rosman C, Bemelmans MH, de Jong D, van Nieuwenhoven EJ, van Engeland MI, Bleichrodt RP (2003) “Components separation technique” for the repair of large abdominal wall hernias. J Am Coll Surg 196:32–37
Shestak KC, Edington HJ, Johnson RR (2000) The separation of anatomic components technique for the reconstruction of massive midline abdominal wall defects: anatomy, surgical technique, applications, and limitations revisited. Plast Reconstr Surg 105:731–738; quiz 739
Girotto JA, Ko MJ, Redett R, Muehlberger T, Talamini M, Chang B (1999) Closure of chronic abdominal wall defects: a long-term evaluation of the components separation method. Ann Plast Surg 42:385–394; discussion 394–395
Cohen M, Morales R Jr, Fildes J, Barrett J (2001) Staged reconstruction after gunshot wounds to the abdomen. Plast Reconstr Surg 108:83–92
Saulis AS, Dumanian GA (2002) Periumbilical rectus abdominis perforator preservation significantly reduces superficial wound complications in “separation of parts” hernia repairs. Plast Reconstr Surg 109:2275–2280; discussion 2281–2282
Maas SM, de Vries RS, van Goor H, de Jong D, Bleichrodt RP (2002) Endoscopically assisted “components separation technique” for the repair of complicated ventral hernias. J Am Coll Surg 194:388–390
Lowe JB 3rd, Lowe JB, Baty JD, Garza JR (2003) Risks associated with components separation for closure of complex abdominal wall defects. Plast Reconstr Surg 111:1276–1283; quiz 1284–1285; discussion 1286–1288
Girotto JA, Chiaramonte M, Menon NG, Singh N, Silverman R, Tufaro AP, Nahabedian M, Goldberg NH, Manson PN (2003) Recalcitrant abdominal wall hernias: long-term superiority of autologous tissue repair. Plast Reconstr Surg 112:106–114
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rosen, M.J., Jin, J., McGee, M.F. et al. Laparoscopic component separation in the single-stage treatment of infected abdominal wall prosthetic removal. Hernia 11, 435–440 (2007). https://doi.org/10.1007/s10029-007-0255-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-007-0255-y