
Abstract
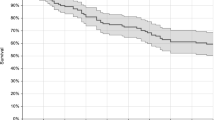
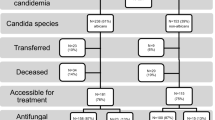
The incidence of Candida bloodstream infections (BSIs) has increased over time, especially in medical wards. The objective of this study was to evaluate the impact of different antifungal treatment strategies on 30-day mortality in patients with Candida BSI not admitted to intensive care units (ICUs) at disease onset. This prospective, monocentric, cohort study was conducted at an 1100-bed university hospital in Rome, Italy, where an infectious disease consultation team was implemented. All cases of Candida BSIs observed in adult patients from November 2012 to April 2014 were included. Patients were grouped according to the initial antifungal strategy: fluconazole, echinocandin, or liposomal amphotericin B. Cox regression analysis was used to identify risk factors significantly associated with 15-day and 30-day mortality. During the study period, 130 patients with candidemia were observed (58 % with C. albicans, 7 % with C. glabrata, and 23 % with C. parapsilosis). The first antifungal drug was fluconazole for 40 % of patients, echinocandin for 57.0 %, and liposomal amphotericin B for 4 %. During follow-up, 33 % of patients died. The cumulative mortality 30 days after the candidemia episode was 30.8 % and was similar among groups. In the Cox regression analysis, clinical presentation was the only independent factor associated with 15-day mortality, and Acute Physiology and Chronic Health Evaluation (APACHE) II score and clinical presentation were the independent factors associated with 30-day mortality. No differences in 15-day and 30-day mortality were observed between patients with and without C. albicans candidemia. In patients with candidemia admitted to medical or surgical wards, clinical severity but not the initial antifungal strategy were significantly correlated with mortality.

Similar content being viewed by others

References
Bassetti M, Merelli M, Righi E et al (2013) Epidemiology, species distribution, antifungal susceptibility, and outcome of candidemia across five sites in Italy and Spain. J Clin Microbiol 51:4167–4172
Hsu DI, Nguyen M, Nguyen L et al (2010) A multicentre study to evaluate the impact of timing of caspofungin administration on outcomes of invasive candidiasis in non-immunocompromised adult patients. J Antimicrob Chemother 65:1765–1770
Parkins MD, Sabuda DM, Elsayed S et al (2007) Adequacy of empirical antifungal therapy and effect on outcome among patients with invasive Candida species infections. J Antimicrob Chemother 60:613–618
Garey KW, Rege M, Pai MP et al (2006) Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: a multi-institutional study. Clin Infect Dis 43:25–31
Bassetti M, Righi E, Ansaldi F et al (2014) A multicenter study of septic shock due to candidemia: outcomes and predictors of mortality. Intensive Care Med 40:839–845
Puig-Asensio M, Pemán J, Zaragoza R et al (2014) Impact of therapeutic strategies on the prognosis of candidemia in the ICU. Crit Care Med 42:1423–1432
González de Molina FJ, León C, Ruiz-Santana S et al (2012) Assessment of candidemia-attributable mortality in critically ill patients using propensity score matching analysis. Crit Care 16:R105
Falagas ME, Apostolou KE, Pappas VD (2006) Attributable mortality of candidemia: a systematic review of matched cohort and case–control studies. Eur J Clin Microbiol Infect Dis 25:419–425
Pappas PG, Kauffman CA, Andes D et al (2009) Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis 48:503–535
Cornely OA, Bassetti M, Calandra T et al; ESCMID Fungal Infection Study Group (2012) ESCMID* guideline for the diagnosis and management of Candida diseases 2012: non-neutropenic adult patients. Clin Microbiol Infect 18:19–37
Scudeller L, Viscoli C, Menichetti F et al (2014) An Italian consensus for invasive candidiasis management (ITALIC). Infection 42:263–279
Fantoni M, Murri R, Scoppettuolo G et al (2015) Resource-saving advice from an infectious diseases specialist team in a large university hospital: an exportable model? Future Microbiol 10:15–20
Knaus WA, Draper EA, Wagner DP et al (1985) APACHE II: a severity of disease classification system. Crit Care Med 13:818–829
Levy MM, Fink MP, Marshall JC et al (2003) 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med 29:530–538
Wisplinghoff H, Ebbers J, Geurtz L et al (2014) Nosocomial bloodstream infections due to Candida spp. in the USA: species distribution, clinical features and antifungal susceptibilities. Int J Antimicrob Agents 43:78–81
Tortorano AM, Prigitano A, Lazzarini C et al (2013) A 1-year prospective survey of candidemia in Italy and changing epidemiology over one decade. Infection 41:655–662
Blot SI, Vandewoude KH, Hoste EA et al (2002) Effects of nosocomial candidemia on outcomes of critically ill patients. Am J Med 113:480–485
Reboli AC, Rotstein C, Pappas PG et al (2007) Anidulafungin versus fluconazole for invasive candidiasis. N Engl J Med 356:2472–2482
Kett DH, Shorr AF, Reboli AC et al (2011) Anidulafungin compared with fluconazole in severely ill patients with candidemia and other forms of invasive candidiasis: support for the 2009 IDSA treatment guidelines for candidiasis. Crit Care 15:R253
Ortega M, Marco F, Soriano A et al (2010) Candida spp. bloodstream infection: influence of antifungal treatment on outcome. J Antimicrob Chemother 65:562–568
Tumbarello M, Fiori B, Trecarichi EM et al (2012) Risk factors and outcomes of candidemia caused by biofilm-forming isolates in a tertiary care hospital. PLoS One 7:e33705
Reboli AC, Shorr AF, Rotstein C et al (2011) Anidulafungin compared with fluconazole for treatment of candidemia and other forms of invasive candidiasis caused by Candida albicans: a multivariate analysis of factors associated with improved outcome. BMC Infect Dis 11:261
Nucci M, Anaissie E, Betts RF et al (2010) Early removal of central venous catheter in patients with candidemia does not improve outcome: analysis of 842 patients from 2 randomized clinical trials. Clin Infect Dis 51:295–303
Kollef M, Micek S, Hampton N et al (2012) Septic shock attributed to Candida infection: importance of empiric therapy and source control. Clin Infect Dis 54:1739–1746
Dannaoui E, Desnos-Ollivier M, Garcia-Hermoso D et al; French Mycoses Study Group (2012) Candida spp. with acquired echinocandin resistance, France, 2004–2010. Emerg Infect Dis 18:86–90
Alexander BD, Johnson MD, Pfeiffer CD et al (2013) Increasing echinocandin resistance in Candida glabrata: clinical failure correlates with presence of FKS mutations and elevated minimum inhibitory concentrations. Clin Infect Dis 56:1724–1732
Acknowledgments
We are grateful to Leonida Passeri for his technical assistance in the data management.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
The present manuscript was revised by San Francisco Edit, which was supported by internal funding.
Rights and permissions
About this article

Cite this article
Murri, R., Scoppettuolo, G., Ventura, G. et al. Initial antifungal strategy does not correlate with mortality in patients with candidemia. Eur J Clin Microbiol Infect Dis 35, 187–193 (2016). https://doi.org/10.1007/s10096-015-2527-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-015-2527-2