
Abstract
To determine whether adiposity assessed by dual-energy X-ray absorptiometry (DXA) compared to simple anthropometric assessments, are more predictive of abdominal aortic calcification (AAC), a risk factor for atherosclerosis. A cross-sectional study of 312 participants (60.3 % female) aged 70.6 ± 5.6 years was conducted in 2010–2011. AAC was assessed by radiography. Adiposity was estimated for whole body, trunk, android, gynoid and visceral regions using DXA in addition to body mass index (BMI), waist circumference (WC) and waist to hip ratio (WHR). WHR [tertile 1 as reference, OR (95 % CI) for tertile 3: 3.62 (1.35–9.72)] and android to gynoid fat ratio [tertile 3: 2.87 (1.03–8.01)] were independent predictors of AAC severity among men. Positive associations with AAC severity were observed for WC [tertile 1 as reference, OR for tertile 3: 2.46 (1.12–5.41)], % trunk fat mass [tertile 2: 3.26 (1.52–7.03)], % android fat mass [tertile 2: 2.42 (1.13–5.18), tertile 3: 2.20 (1.02–4.73)] and visceral fat area [tertile 2: 2.28 (1.06–4.87), tertile 3: 2.32 (1.01–5.34)] among women. Indices of total body composition, BMI and % body fat mass were not associated with AAC severity in either men or women. Simple anthropometric measures, WHR and WC were the best predictors of AAC severity in men and women respectively, although higher android to gynoid fat ratio and central fat, assessed by DXA, were also predictive of higher risks of AAC severity in men and women respectively. Our findings add to existing evidence that relatively inexpensive and easily obtained anthropometric measures can be clinically useful indicators of atherosclerosis risk.
Similar content being viewed by others


Introduction
As a strong marker of atherosclerosis, vascular calcification, especially abdominal aortic calcification (AAC), is an independent predictor of cardiovascular disease (CVD) and vascular morbidity and mortality [1]. Fat accumulation in different body regions may play different roles in mediating cardiovascular and metabolic risk [2, 3]. An increasing number of studies have investigated the associations of anthropometric measures including body mass index (BMI), waist circumference (WC) and waist to hip ratio (WHR) with vascular calcification [4–6]. Some studies reported that BMI, WC, and WHR were independent predictors of AAC [5, 7], whereas others did not find an association [6, 8]. Dual-energy X-ray absorptiometry (DXA) precisely evaluates body composition in different regions including android, gynoid, trunk and whole body [9]. Recently, a newly developed method for precisely evaluating visceral fat using DXA was demonstrated to have comparable reliability to computed tomography (CT), with much lower radiation effective doses and equipment costs [10]. Visceral fat has been demonstrated to be a stronger predictor of cardiovascular risk than traditional anthropometric measures such as BMI and WC [11]. Prior studies examining the association between visceral fat and AAC mostly used CT to measure visceral fat [8, 12]. Trunk fat mass was demonstrated to be a predictor of AAC in univariate models [6, 12], but not in multivariate models [8, 13]. Android adiposity and android to gynoid fat ratio by DXA predict metabolic and CVD risks [14, 15], but their associations with AAC are unknown. Quantifying the association between fat distribution assessed by DXA and AAC is of interest to test the hypothesis that central fat deposits have a greater effect on atherosclerosis in the abdominal aorta.
Whether the accurate measures of adipose tissue by DXA are more closely related to AAC than simple anthropometric measures has important public health implications. We aimed to evaluate whether adiposity measured by DXA was a better predictor of AAC than that measured by anthropometry among community-dwelling older adults by ranking predictors in logistic regression.
Materials and methods
Study population
The present study was based on a subset of the Melbourne Collaborative Cohort Study (MCCS) [16, 17] and the data was collected in 2010–2011. Briefly, the MCCS is a prospective cohort study including 41,514 participants at baseline (1990–1994). The primary aim of the present sub study was to evaluate the impact of low and high dietary calcium intake on bone density, fractures, vascular events, and aortic calcifications. A total of 956 subjects who resided close to Western Hospital, were aged between 45 and 64 years old (at baseline), were fluent in English and had calcium intakes ≤500 mg/day or ≥1300 mg/day were approached to participate in this sub-study. Four hundred and seven participants were eligible for the study after screening; 353 completed DXA scans and 346 completed radiographs at follow-up (2010–2011). Of the participants who completed radiographs, 312 with readable radiographs were included in our data analysis for the association between body composition and AAC severity. Informed consent was obtained from all participants. The study protocol was approved by the Cancer Council Victoria and Melbourne Health Human Research Ethics Committees.
Information including country of birth, marital status, education level, employment status, and physical activity were obtained. Physical activity was evaluated using the Community Health Activities Model Program for Seniors (CHAMPS) questionnaire for older adults [18]. CHAMPS is a 41-item self-administered questionnaire that captures usual weekly “amounts” and “intensities” of different types of activity during the past 4 weeks in older adults. According to the assigned metabolic values for each specified activity, energy expenditure per week from physical activity was calculated [18].
Anthropometric measurements
Height, weight, waist and hip circumferences, as well as blood pressure, were measured as per standard protocols [19]. Weight was measured in light clothing without shoes using an electronic digital scale to the nearest 50 g. Standing height was measured using a stadiometer to the nearest 0.1 cm. BMI was calculated as weight in kilograms divided by the square of height in metres. Waist circumference was measured to the nearest 0.1 cm using an inelastic plastic fibre measuring tape. The measuring tape was placed at the mid-point between the lowest floating rib and the top of the iliac crest. Hip circumference was measured in the same standing position with the measuring tape around the maximum circumference of the buttocks. WHR was calculated as WC in centimetres divided by hip circumference in centimetres. Resting blood pressure and heart rate were measured for each participant in a seated position with the level of the cuff at the level of the heart using an automatic blood pressure monitor. Two readings of blood pressure were measured separated by a 5 min interval.
Body composition was measured using a Hologic bone densitometer (QDR 4500 W, Hologic Inc., Bedford, Massachusetts), which uses a fan-beam based DXA. Participants were asked to lie straight in a supine position on the scanner table with their feet slightly internally rotated and held fixed in that position using a tape throughout the duration of the scan. Before commencing the scanning procedure, it was ensured that no part of the body was outside the boundary lines marked on the table top and hands were not beneath the body. Based on the degree of attenuation caused by different mass and types of tissue when the fan-beam energy passes through the body [20], scans obtained were analysed to calculate fat mass and lean mass at arms, legs, android and gynoid regions, trunk, and the whole body. We calculated % body fat mass as total fat mass divided by total body mass; percentage fat mass in different regions including % trunk fat mass, % gynoid fat mass, and % android fat mass were calculated in the same way, i.e. mass of fat as a percentage of total mass for the region. By recognizing the subcutaneous fat ring, inner abdominal muscle wall, and visceral cavity, a model was used to estimate subcutaneous fat in the abdominal region, and visceral fat area was calculated by subtracting this estimate from the total abdominal fat area [10]. Visceral fat area has been considered as a valuable marker for predicting CVD [21]. Daily quality control tests were performed using a standardized phantom, and longitudinal quality control data did not indicate any significant shifts or drifts in scanner performance during the period of the study.
Plasma lipid test
Fasting blood samples were obtained by the Melbourne Pathology Collection Centre. Total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides (TG) were measured using an automatic biochemistry analyzer (Roche Cobas 8000 modular analyzer Series C701).
Assessment of abdominal aortic calcification
AAC was assessed by using a semi-quantitative visually based technique [22] with the use of lateral thoraco-lumbar radiography. The score was assessed by BK and confirmed by a trained radiologist (NK) who has worked in the Department of Radiology of an Imaging Research Centre for many years. If scores between assessors were inconsistent, a further assessment by both assessors together was performed to achieve agreement. The severity of calcific deposits in anterior and posterior walls of the abdominal aorta anterior to the first four lumbar vertebrae was scored from 0 to 3 (0 = no calcification, 1 = one-third or less of the aortic wall in that vertebral segment was calcified, 2 = between one-third to two-thirds or less of the aortic wall was calcified-2, or 3 = more than two-thirds of the aortic wall was calcified). The score of the eight segments were summed as the AAC score (AACS range 0–24) [17]. Accordingly, participants were categorized into groups as “no calcification” (AACS = 0), “moderate calcification” (AACS between 1 and 5) and “high calcification” (AACS ≥6) [23].
Statistical analysis
Continuous variables were expressed as mean ± SD and categorical variables were summarised as frequency (percentage). Ordinal logistic regression was used to evaluate the associations between body composition measurement and AAC severity (three categories as stated above set as 0, 1 and 2). Since there were significant interactions with gender for % body fat mass (P value = 0.004), % trunk fat mass (P value = 0.037), % android fat mass (P value = 0.039) and android to gynoid fat ratio (P value = 0.0009), the analyses were stratified by gender. P values for trend were calculated for AAC severity across tertiles of body composition measurements. We tested following models: (1) adjusted for age; (2) adjusted for Model 1 plus smoking and physical activity; (3) adjusted for Model 2 plus diastolic blood pressure, systolic blood pressure, high-density lipoprotein cholesterol and low-density lipoprotein cholesterol.
Adequacy and Akaike Information Criterion (AIC) statistical methods were used to rank predictors of AAC for women and men separately to examine which of the adiposity measures by anthropometry and DXA were more predictive of AAC [24].
P values <0.05 by two tailed test were considered significant. All statistical analyses were performed with the SAS 9.3 for Windows (SAS Institute Inc, Cary, NC).
Results
Fat distribution differences between men and women
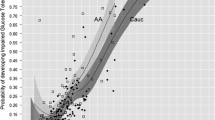
Three hundred and twelve participants (124 men and 188 women) aged 70.6 ± 5.6 years were included in the analysis. Men had higher ratio of android to gynoid fat than women (P < 0.001). Higher android fat mass (P = 0.02) but lower gynoid fat mass (P < 0.001) were found in men compared with women (Table 1). The frequency distribution of AACS by sex is shown in Fig. 1.

Frequency distribution of abdominal aortic calcification score by sex
The associations between adiposity and AAC severity in older men
Of the three anthropometric measures, only WHR was a significant predictor of AAC severity among men after adjustment for age, smoking, self-reported physical activity, blood pressure, serum TG, HDL and LDL. Amongst DXA measures, a higher ratio of android to gynoid fat but not higher percentages of whole body, trunk, android, and gynoid fat mass or visceral fat area was associated with higher risk of AAC severity in men (Table 2).
The associations between adiposity and AAC severity in older women
Among women, BMI was positively associated with AAC severity and the association was attenuated after adjustment for confounders. WC, but not WHR, was also a significant predictor of AAC severity after adjustment for confounders in women. Percentage of android fat mass was positively associated with AAC severity in women. Women in the second tertile (between 35 and 40 %), but not third tertile (between 41 and 54 %) of % trunk fat mass had higher risk of AAC severity after adjustment for confounders than those in the lowest tertile (<35 %). A significant positive association between visceral fat area and AAC severity was also observed among women after adjustment for confounders. Android to gynoid fat ratio and % whole body fat mass were not significantly associated with AAC severity after adjustment for confounders in women (Table 3).
Ranking predictors in multivariate-adjusted logistic regression model
For men, WHR, WC and android to gynoid fat ratio were the top ranking predictors of AAC by both the Adequacy and AIC statistic methods. WC was the measurement most strongly associated with AAC for women and WHR, visceral fat area and % android fat mass were ranked top two to four by both methods (Table 4).
Discussion
In this study of community-dwelling older adults, indices of total body composition, BMI and % body fat mass were not independently associated with AAC severity in either men or women. Simple anthropometric measures of body fat distribution, WHR and WC were significant independent predictors of AAC severity among men and women respectively. A higher ratio of android to gynoid fat mass assessed by DXA was associated with higher risk of AAC severity among men. DXA measures, % android fat mass, % trunk fat mass and visceral fat area were positively associated with the risk of AAC severity among women. Compared with the DXA measures, simple anthropometry appeared to be a similar or better measure for predicting AAC severity.
Central fat distribution assessed by WHR but not WC or BMI was a significant predictor of AAC severity among men with a mean age of 71 years in our study. Although BMI was an independent predictor of coronary artery calcification in middle-aged men (40–49 years), BMI and total fat mass were not associated with aortic calcification severity in elderly men with a mean age of 59 years [6]. As an index of total body composition, BMI might not be a good marker of AAC severity in the elderly [25], given that BMI has limited ability to assess regional fat distribution or muscle tissue. WHR was previously shown to be positively associated with coronary artery calcification, but sex-specific associations were not examined [4]. One study examined the association of the inflammatory marker, C-reactive protein with BMI, WC and WHR, and found the strongest correlation for men was for WHR [26]. Amongst DXA measures of adiposity, we found only android to gynoid fat ratio was an independent predictor of AAC severity in men. Walton et al. evaluated the relationship between android to gynoid fat ratio and CVD risks and reported a positive association with TG and an inverse association with HDL-C in men [27]. Our findings and the literature reviewed here suggest that for men, ratios that assess central adiposity relative to lower body adiposity were the most closely associated with a range of CVD risk factors.
For women, we found central fat distribution assessed by WC was a significant predictor of AAC severity and positive associations with AAC severity were also seen for DXA measures including % trunk fat mass, % android fat mass and visceral fat area. Compared with BMI, WC has previously been shown to be more strongly associated with coronary atherosclerosis independent of traditional CVD risk factors [28]. In comparison with BMI, the greater ability of WC to predict CVD health risks may be attributed to its stronger prediction of abdominal fat [29]. In a prospective study of 316 women aged 50–76 years followed up over 7.7 years, baseline trunk fat mass including both the subcutaneous and the visceral fat of this region was not independently correlated with the progression of aortic calcification [30]. Absolute trunk fat mass might not be a good marker of CVD risk because of its dependence on body size (height) of individuals as seen in our study (data not shown). Although, data on the associations of % android fat mass with vascular calcification are limited, evidence from previous studies is supportive of our findings, indicating a positive association between absolute android fat mass and metabolic risks [14, 15]. Few data exist evaluating the association between visceral fat area assessed by the newly developed DXA method and AAC severity in women. However, consistent with our observation, a previous cross-sectional study of 1160 participants which used electron beam CT to evaluate AAC and visceral fat [12] reported that visceral fat volume was positively associated with AAC only in women [OR (95 % CI) for third tertile vs. first tertile: 1.90 (1.09–3.22)]. In contrast to the findings in men, for women the associations with AAC appeared to be stronger for measures of central adiposity that did not include a measure of lower body fat.
When comparing different measures of adiposity, WHR and WC were the strongest predictors of AAC severity in men and women respectively. A limitation of the adequacy method for ranking predictors in logistic regression models is that the adequacy value can be large, even if the predictor is weakly associated with the outcome [24]. However, WC, WHR, visceral fat area and % android fat mass were ranked the top four predictors of AAC by both the Adequacy and AIC methods in women, corresponding to the results in Table 3 that showed WC, visceral fat area and % android fat mass were significantly and WHR was marginally associated with AAC severity. For men, WHR and android to gynoid fat ratio that were positively associated with AAC severity in multivariate-adjusted models were ranked the top one and three predictors of AAC severity by both methods. Our findings suggested that the Adequacy and AIC methods might be effective in ranking predictors of AAC severity.
We found that a higher ratio of central fat to lower body fat was associated with increased risk of AAC severity in men whereas central fat was a significant predictor of AAC severity in women. Consistent with previous studies [31], android obesity was more common in men while women tended to demonstrate gynoid obesity in our study. The sexual dimorphism of fat distribution pattern may be an explanation for why risk factors for AAC severity in men differ from those in women. In addition, sex differences in hormones such as testosterone and oestrogen may contribute to the sex differences in the association between fat distribution pattern and AAC, due to the fact that these hormones are associated with both adiposity and chronic disease [32]. Meanwhile, metabolic risk factors including dyslipidemia, elevated blood pressure and elevated glucose could have an impact on the associations between body fat distribution and atherosclerotic CVD [33] and these effects in men might differ from women [34]. Therefore, metabolic risk factors may be a mediator for the gender specific differences in the association between adiposity and AAC severity.
The limitations of our study include that it is a cross-sectional study and does not allow for inference of a causal relationship. In addition, non-English speaking participants were excluded, so our results cannot be generalized to the whole population. Finally, the exclusion of participants with calcium intake between 500 and 1300 mg/day might also influence our results, even though further adjustment for calcium intake in the multi-variate model did not modify the association between body composition and AAC (data not shown).
Conclusion
Our findings are consistent with the hypothesis that excess fat in the abdominal region is associated with increased risk of CVD in comparison with gynoid obesity where excess fat is stored in hip and buttock areas [35, 36]. Simple anthropometric measures, WHR and WC were the best predictors of AAC severity in men and women respectively, although higher android to gynoid fat ratio and central fat, assessed by DXA, were also predictive of higher AAC score in men and women respectively. Central fat relative to lower body fat appears to be more relevant in men while total central fat may be more important for women in predicting AAC. Our findings add to existing evidence that relatively inexpensive and easily obtained anthropometric measures can be clinically useful indicators of atherosclerosis risk.
References
Wilson PW, Kauppila LI, O’Donnell CJ, Kiel DP, Hannan M, Polak JM, Cupples LA (2001) Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation 103:1529–1534
Yudkin JS, Eringa E, Stehouwer CD (2005) “Vasocrine” signalling from perivascular fat: a mechanism linking insulin resistance to vascular disease. Lancet 365:1817–1820
de Vos AM, Prokop M, Roos CJ, Meijs MF, van der Schouw YT, Rutten A, Gorter PM, Cramer MJ, Doevendans PA, Rensing BJ, Bartelink ML, Velthuis BK, Mosterd A, Bots ML (2008) Peri-coronary epicardial adipose tissue is related to cardiovascular risk factors and coronary artery calcification in post-menopausal women. Eur Heart J 29:777–783
Cassidy AE, Bielak LF, Zhou Y, Sheedy PF 2nd, Turner ST, Breen JF, Araoz PA, Kullo IJ, Lin X, Peyser PA (2005) Progression of subclinical coronary atherosclerosis: does obesity make a difference? Circulation 111:1877–1882
Canepa M, Ameri P, AlGhatrif M, Pestelli G, Milaneschi Y, Strait JB, Giallauria F, Ghigliotti G, Brunelli C, Lakatta EG, Ferrucci L (2014) Role of bone mineral density in the inverse relationship between body size and aortic calcification: results from the Baltimore Longitudinal Study of Aging. Atherosclerosis 235:169–175
Alexandersen P, Tanko LB, Bagger YZ, Jespersen J, Skouby SO, Christiansen C (2006) Associations between aortic calcification and components of body composition in elderly men. Obesity (Silver Spring) 14:1571–1578
Hughes-Austin JM, Wassel CL, Jimenez J, Criqui MH, Ix JH, Rasmussen-Torvik LJ, Budoff MJ, Jenny NS, Allison MA (2014) The relationship between adiposity-associated inflammation and coronary artery and abdominal aortic calcium differs by strata of central adiposity: the Multi-Ethnic Study of Atherosclerosis (MESA). Vascular 19:264–271
Liu J, Musani SK, Bidulescu A, Carr JJ, Wilson JG, Taylor HA, Fox CS (2012) Fatty liver, abdominal adipose tissue and atherosclerotic calcification in African Americans: the Jackson Heart Study. Atherosclerosis 224:521–525
Rossner S, Bo WJ, Hiltbrandt E, Hinson W, Karstaedt N, Santago P, Sobol WT, Crouse JR (1990) Adipose tissue determinations in cadavers—a comparison between cross-sectional planimetry and computed tomography. Int J Obes 14:893–902
Kaul S, Rothney MP, Peters DM, Wacker WK, Davis CE, Shapiro MD, Ergun DL (2012) Dual-energy X-ray absorptiometry for quantification of visceral fat. Obesity (Silver Spring) 20:1313–1318
Vega GL, Adams-Huet B, Peshock R, Willett D, Shah B, Grundy SM (2006) Influence of body fat content and distribution on variation in metabolic risk. J Clin Endocrinol Metab 91:4459–4466
Ditomasso D, Carnethon MR, Wright CM, Allison MA (2010) The associations between visceral fat and calcified atherosclerosis are stronger in women than men. Atherosclerosis 208:531–536
Alvey NJ, Pedley A, Rosenquist KJ, Massaro JM, O’Donnell CJ, Hoffmann U, Fox CS (2014) Association of fat density with subclinical atherosclerosis. J Am Heart Assoc 3:e000788
Peterson MD, Al Snih S, Serra-Rexach JA, Burant C (2015) Android adiposity and lack of moderate and vigorous physical activity are associated with insulin resistance and diabetes in aging adults. J Gerontol A Biol Sci Med Sci 70(8):1009–1117
Kang SM, Yoon JW, Ahn HY, Kim SY, Lee KH, Shin H, Choi SH, Park KS, Jang HC, Lim S (2011) Android fat depot is more closely associated with metabolic syndrome than abdominal visceral fat in elderly people. PLoS One 6:e27694
Giles GG, English DR (2002) The Melbourne Collaborative Cohort Study. Int Agency Res Center Sci Publ 156:69–70
Shang X, Sanders KM, Scott D, Khan B, Hodge A, Khan N, English DR, Giles GG, Ebeling PR (2015) Dietary alpha-linolenic acid and total omega-3 fatty acids are inversely associated with abdominal aortic calcification in older women, but not in older men. J Nutr 145:1778–1786
Stewart AL, Mills KM, King AC, Haskell WL, Gillis D, Ritter PL (2001) CHAMPS physical activity questionnaire for older adults: outcomes for interventions. Med Sci Sports Exerc 33:1126–1141
Lohman TJ, Roche AF, Martorell R (1992) Anthropometric standardization reference manual. Med Sci Sports Exerc 24(8):p952
Peppler WW, Mazess RB (1981) Total body bone mineral and lean body mass by dual-photon absorptiometry. I. Theory and measurement procedure. Calcif Tissue Int 33:353–359
Nicklas BJ, Penninx BW, Ryan AS, Berman DM, Lynch NA, Dennis KE (2003) Visceral adipose tissue cutoffs associated with metabolic risk factors for coronary heart disease in women. Diabetes Care 26:1413–1420
Bolland MJ, Wang TK, van Pelt NC, Horne AM, Mason BH, Ames RW, Grey AB, Ruygrok PN, Gamble GD, Reid IR (2010) Abdominal aortic calcification on vertebral morphometry images predicts incident myocardial infarction. J Bone Miner Res 25:505–512
Stone NJ (1996) Fish consumption, fish oil, lipids, and coronary heart disease. Circulation 94:2337–2340
Thompson D (2009) Ranking predictors in logistic regression. SAS User Group, Cleveland
Prentice AM, Jebb SA (2001) Beyond body mass index. Obes Rev 2:141–147
Connelly PW, Hanley AJ, Harris SB, Hegele RA, Zinman B (2003) Relation of waist circumference and glycemic status to C-reactive protein in the Sandy Lake Oji-Cree. Int J Obes Relat Metab Disord 27:347–354
Walton C, Lees B, Crook D, Worthington M, Godsland IF, Stevenson JC (1995) Body fat distribution, rather than overall adiposity, influences serum lipids and lipoproteins in healthy men independently of age. Am J Med 99:459–464
Bose S, Krishnamoorthy P, Varanasi A, Nair J, Schutta M, Braunstein S, Iqbal N, Schwartz S, St Clair C, Master SR, Rader DJ, Reilly MP, Mehta NN (2013) Measurement of waist circumference predicts coronary atherosclerosis beyond plasma adipokines. Obesity (Silver Spring) 21:E118–E123
Janssen I, Heymsfield SB, Allison DB, Kotler DP, Ross R (2002) Body mass index and waist circumference independently contribute to the prediction of nonabdominal, abdominal subcutaneous, and visceral fat. Am J Clin Nutr 75:683–688
Tanko LB, Bagger YZ, Alexandersen P, Larsen PJ, Christiansen C (2003) Central and peripheral fat mass have contrasting effect on the progression of aortic calcification in postmenopausal women. Eur Heart J 24:1531–1537
Kissebah AH, Krakower GR (1994) Regional adiposity and morbidity. Physiol Rev 74:761–811
Wells JC (2007) Sexual dimorphism of body composition. Best Pract Res Clin Endocrinol Metab 21:415–430
Grundy SM (2004) Obesity, metabolic syndrome, and cardiovascular disease. J Clin Endocrinol Metab 89:2595–2600
Tonstad S, Sandvik E, Larsen PG, Thelle D (2007) Gender differences in the prevalence and determinants of the metabolic syndrome in screened subjects at risk for coronary heart disease. Metab Syndr Relat Disord 5:174–182
Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L (2004) Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 364:937–952
Casanueva FF, Moreno B, Rodriguez-Azeredo R, Massien C, Conthe P, Formiguera X, Barrios V, Balkau B (2010) Relationship of abdominal obesity with cardiovascular disease, diabetes and hyperlipidaemia in Spain. Clin Endocrinol 73:35–40
Acknowledgments
This study was funded by the Department of Medicine, Western Hospital and the University of Melbourne Research Grant Scheme and a Heart Foundation Grant. The Melbourne Collaborative Cohort Study is funded by VicHealth and Cancer Council Victoria and further supported by Australian NHMRC Grants 209057, 251553 and 504711 and by infrastructure provided by Cancer Council Victoria. We thank the other investigators, staff, and participants of the Melbourne Collaborative Cohort Study cohort for their important contributions.
Author contribution
Dallas R English, Graham G Giles, and Peter R Ebeling conceived and designed the research. Xianwen Shang, Kerrie M Sanders, David Scott, and Allison Hodge conducted data analysis, interpretation, and wrote the initial draft of the manuscript. Belal Khan and Nayab Khan carried out experiments.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Shang, X., Scott, D., Hodge, A. et al. Adiposity assessed by anthropometric measures has a similar or greater predictive ability than dual-energy X-ray absorptiometry measures for abdominal aortic calcification in community-dwelling older adults. Int J Cardiovasc Imaging 32, 1451–1460 (2016). https://doi.org/10.1007/s10554-016-0920-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-016-0920-2