
Abstract
Taiwan’s global budgeting for hospital health care, in comparison to other countries, assigns a regional budget cap for hospitals’ medical benefits claimed on the basis of fee-for-service (FFS) payments. This study uses a stays-hospitals-years database comprising acute myocardial infarction inpatients to examine whether the reimbursement policy mitigates the medical benefits claimed to a third-payer party during 2000–2008. The estimated results of a nested random-effects model showed that hospitals attempted to increase their medical benefit claims under the influence of initial implementation of global budgeting. The magnitudes of hospitals’ responses to global budgeting were significantly attributed to hospital ownership, accreditation status, and market competitiveness of a region. The results imply that the regional budget cap superimposed on FFS payments provides only blunt incentive to the hospitals to cooperate to contain medical resource utilization, unless a monitoring mechanism attached with the payment system.





Similar content being viewed by others



Notes
The global budgeting has not changed the payment basis for every individual hospital; hence the claimed numbers of points for all service items listed on the BNHI payment scheme are fixed. Since the “relative prices” for all service items are still unchanged, the global budgeting creates no incentive for healthcare providers by increasing one type of procedure instead of decreasing the other one under the mechanism. Due to this reason, the study could choose a single disease to identify policy effect.
Medical centers and metropolitan hospitals are both large teaching hospitals. Taiwan’s BNHI stipulates that only large teaching hospital can carry out percutaneous coronary angioplasty (PTCA) or coronary artery bypass grafting (CABG) procedures; therefore, the majority of AMI inpatients are admitted to these two levels of hospitals.
The high-competition markets include the Taipei and Central divisions; the middle-competition markets include the Southern and Kaoping divisions; and the low-competition markets include the Northern and Eastern divisions.
Fig. 2 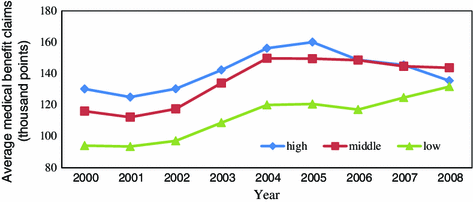
Averge medical claims of AMI inpatients by market competition
AMI is listed as Charlson index = 1; Charlson index of all AMI inpatients are labeled as at least “1”.

References
Benstetter, F., & Wambach, A. (2006). The treadmill effect in a fixed budget system. Journal of Health Economics, 25(1), 146–169.
Bishop, C. E., & Wallack, S. S. (1996). National health expenditure limits: The case for a global budget process. Milbank Quarterly, 74(3), 361–376.
Chen, F. J., Laditka, J. N., Laditka, S. B., & Xirasagar, S. (2007). Providers’ responses to global budgeting in Taiwan: What were the initial effects? Health Services Management Research, 20(2), 113–120.
Cheng, S. H., Chen, C. C., & Chang, W. L. (2009). Hospital response to a global budget program under universal health insurance in Taiwan. Health Policy, 92, 158–164.
Dormont, B., & Milcent, C. (2004). The sources of hospital cost variability. Health Economics, 13(10), 927–939.
Fan, C. P., Chen, K. P., & Kan, K. (1998). The design of payment systems for physicians under global budget—an experimental study. Journal of Economic Behavior & Organization, 34(2), 295–311.
Henke, K. D., Murrary, M. A., & Ade, C. (1994). Global budgeting in Germany: Lessons for the United States. Health Affairs, 13(4), 7–21.
Hurley, J., & Card, R. (1996). Global physician budgets as common-property resources: some implications for physicians and medical associations. Canadian Medical Association Journal, 154(8), 1161–1168.
Hurley, J., Lomas, J., & Goldsmith, L. J. (1997). Physician responses to global physician expenditure budgets in Canada: A common property perspective. Milbank Quarterly, 75(3), 343–364.
Lee, M. C., & Jones, A. M. (2004). How did dentists respond to the introduction of global budgets in Taiwan? An evaluation using individual panel data. International Journal of Health Care Finance and Economics, 4, 307–326.
Lo, J. C., & Chan, V. L. (2007). An exploratory investigation of the effect of hospital global budgeting on payment distribution. Taiwan Journal of Public Health, 26(4), 261–269.
McClellan, M., & Newhouse, J. P. (1997). The marginal cost-effectiveness of medical technology: A panel instrumental variables approach. Journal of Econometrics, 77(1), 39–64.
Mougeot, M., & Naegelen, F. (2005). Hospital price regulation and expenditure cap policy. Journal of Health Economics, 24(1), 55–72.
Redmon, D. P., & Yakoboski, P. J. (1995). The nominal and real effects of hospital global budgets in Finance. Inquiry, 32(2), 174–183.
Rochaix, L. (1993). Financial incentives for physicians: The Quebec experience. Health Economics, 2(2), 163–176.
Shen, Y. C. (2002). The effect of hospital ownership choice on patient outcomes after treatment for acute myocardial infarction. Journal of Health Economics, 21(5), 901–922.
Yakoboski, P. J., Ratner, J., & Gross, D. J. (1994). The effectiveness of budget targets and caps in the German ambulatory care sector. Benefits Quarterly, 10(3), 31–37.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hsu, PF. Does a global budget superimposed on fee-for-service payments mitigate hospitals’ medical claims in Taiwan?. Int J Health Care Finance Econ 14, 369–384 (2014). https://doi.org/10.1007/s10754-014-9149-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10754-014-9149-6