
Abstract
The number of African-born residents living in the United States (US) increased by more than 750 % between 1980 and 2009. HIV diagnosis rates in this population are six times higher than estimated incidence in the general US population. African-immigrants with HIV are also diagnosed at later stages of infection than US-born residents, but they paradoxically have lower mortality after diagnosis. There are higher rates of HIV among women, higher rates of heterosexual transmission, and lower rates of injection-drug-use-associated transmission among African-born residents in the US relative to the general US population. Despite this distinct epidemiologic profile, surveillance reports often group African-born residents with US-born Blacks. The high rates of HIV among African-born residents in the US combined with increasing immigration and incomplete surveillance data highlight the need for more accurate epidemiologic data along with appropriate HIV service programs.
Similar content being viewed by others

Introduction
An estimated 34 million people worldwide were living with HIV at the end of 2010 [1]. Almost 70 % (23 million) reside in sub-Saharan Africa, where only 10 % of the world’s population lives [2]. The scale of the epidemic in Africa, coupled with significant emigration, has significantly impacted HIV epidemiology in other regions. In Europe, African-born residents with HIV account for 16 % of all new diagnoses and 38 % of all heterosexual transmission [3]. In the United States, the HIV diagnosis rates among African-born US residents are six times higher than in the general population [4] and immigration from Africa has increased more than seven fold over the past 30 years [5]. Despite this, the overall contribution of HIV among African-born US residents to the epidemic in the United States is unknown [4].
Overall, Blacks in the US accounted for 51 % of new HIV diagnoses in 2006, while making up only 12 % of the population [6]. However, the proportion of African-born Blacks within this group has not yet been measured [4, 7]. US government agencies have responded to the disproportionate burden sustained by Blacks with numerous research, advocacy, and programmatic initiatives; [8] yet surveillance reports frequently do not distinguish between African- and native-born Blacks [6]. This is in spite of an increase in the number of African-born US residents from 200,000 to more than 1.5 million between 1980 and 2009 [5], concurrent with the amplification of the pandemic in Africa [9].
The African population in the US is primarily concentrated in large urban centers [11], with 11 % of the total US African population in New York City alone [10, 11]. African-born US residents frequently live in close geographic proximity to urban areas with high HIV prevalence [12]. Although African immigrants have historically had higher rates of English proficiency, advanced degrees, and employment than foreign-born US residents overall [13], they also experience a higher poverty rate [5]. More recently, unemployment in this population has begun to rise and rates of English-proficiency are decreasing [5]. The African population in the US is also characterized by a high degree of diversity in terms of geographic origin with 36 % of African-born US residents from West Africa, 28 % from East Africa, 18 % from North Africa, 6 % from Southern Africa, 4 % from Central Africa, and 8 % of unspecified regional origin [5]. Each African region is home to dozens to hundreds of distinct ethnic and linguistic subgroups [14].
The main US immigration policy response to HIV historically focused on preventing infected persons from entering the country [15]. From 1987 to 2010, HIV-positive status was grounds for inadmissibility for applicants for short-term non-immigrant visas and for lawful permanent residence, unless granted a waiver [16]. The policy was highly controversial for its human rights implications [17]. Its impact on the epidemiology of HIV was also questioned as it is likely that only a small minority of foreign-born persons entering the US were tested under the terms of the policy [18]. The restrictions were lifted in 2010 when HIV was removed from the list of Communicable Diseases of Public Health Significance [19].
The increase in African immigration to the US, along with high HIV prevalence in sub-Saharan Africa, make a review of the published literature on HIV/AIDS among African-born US residents pertinent. The objectives of conducting this review are to identify gaps in knowledge as well as priorities for research and service provision.
Methods
The authors conducted comprehensive searches of PubMed using all combinations of the following search terms: “HIV,” “AIDS,” “Africans,” “sub-Saharan Africa,” “Immigration,” and “United States,” with both “United States” and either “HIV” or “AIDS,” as required search terms and a minimum of three terms per search. Combinations of three terms yielded 68–537 results per search. Only articles pertaining directly to African-born US residents and HIV/AIDS were retained, and all others were discarded. The reference sections of selected papers were also examined for additional relevant articles missed in the PubMed search.
Results
We found 15 articles that specifically address HIV among African immigrants living in the United States (Table 1). Of these, two present a general picture of HIV epidemiology through analyses of surveillance data [4, 7], and the remaining 13 are case studies of specific cohorts [18, 20–31]. The findings from these papers are discussed below.
High Diagnosis Rates Among Africans in the US
The heavy burden of HIV in sub-Saharan Africa is reflected in high diagnosis rates among African-born US residents [4, 7]. An analysis of surveillance data in the eight metropolitan statistical areas where African-born US residents make up more than 0.5 % of the population found a crude diagnosis rate among African-born US residents of 120.6 per 100,000 persons per year [4]. This rate is six times higher than estimated incidence in the general US population [32], 12 times higher than estimated incidence among White US-born persons [33], and two-thirds higher than crude diagnosis rates among Black US-born persons [7] (Table 2). The crude diagnosis rate among African-born US residents [4] is also two-thirds higher than rates among all Black foreign-born persons in the US [7] (Table 2), likely reflecting lower HIV incidence in the Caribbean [34] relative to sub-Saharan Africa, as well as the comparatively large number of Black Caribbean immigrants in the US [35]. Although higher than other US groups, the diagnosis rate among African-born immigrants is half of estimated incidence in Africa [1] (Table 2). The reasons for this difference are unknown, but may be due to the predominance of immigrants from West Africa (where HIV prevalence is lower than East, Central, or Southern Africa [2]), the healthy immigrant effect (lower rates of chronic-disease-related mortality in first generation immigrants [36]), HIV underdiagnosis among African-born US residents, and the different statistical measures available (crude diagnosis rate vs estimated incidence).
Disproportionate Burden Born by African-Born Black Women
The difference in the burden of HIV between African- and US-born US residents is magnified among women. The available data show that crude diagnosis rates among African-born women [4] are 12 times higher than estimated incidence among women in the general US population [32], 36 times higher than estimated incidence among White US-born women [33], three times higher than crude diagnosis rates among Black US-born women [7], and almost two times higher than crude diagnosis rates among Black foreign-born women [7] (Table 2). Crude diagnosis rates among African-born women are also a third higher than among African-born men in the US [4], which is similar to the gender distribution of estimated new infections in sub-Saharan Africa [1] (Table 2). Other smaller studies have also found higher rates of infection among African-born women than African-born men [21, 26], or higher rates among African-born women in the US than other groups [31].
Higher Rates of Heterosexual Transmission
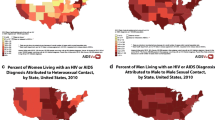
The excess burden of HIV among African-born women points to different transmission risk distributions between African-born US residents and US-born US residents. HIV transmission in sub-Saharan Africa [1] and among Africans in Europe [37] is predominantly heterosexual, and this appears to also be true among African-born US residents. The proportion of new infections attributable to heterosexual transmission is four times higher among African-born US residents than the general US population (92 vs 23 %) [4]. In contrast, 53 % of new infections in 2006 in the general US population were among men who have sex with men [38]. Another analysis similarly identified heterosexual contact as the primary risk factor among three times as many foreign as US-born Blacks (75 vs 28 %)[7], and studies with smaller samples have reported similar findings [23, 26, 31].
Lower Rates of Transmission Associated with Injection Drug Use and with Younger Age
In addition to a higher rate of heterosexual transmission, injection drug use-associated transmission is almost three times lower among foreign-born Blacks than among US-born persons (7 vs 19 %) [7]. Surveillance data also suggests that foreign-born Blacks living with HIV are slightly older than US-born Blacks with a lower percentage in the 13–29 age range (22 vs 29 %), and a higher percentage in the 30–59 age range (34 vs 29 %) [7].
Geographic Location of Infection
Only one study addressed whether African-born US residents living with HIV are infected in their countries of origin or in the United States [21]. The authors of this study found that African-born US residents living with HIV and receiving care at public clinics in Los Angeles had entered the US more recently and at older ages than other immigrant groups, and hypothesize based on this finding that African-born US residents are most often infected in their country of origin.
Late Stage of Infection at Diagnosis
Africans with HIV in the US face particular challenges accessing screening services. They are diagnosed with lower CD4 counts and higher rates of Acquired Immunodeficiency Syndrome (AIDS) (markers of late diagnosis) than US-born persons and most other foreign-born groups [7, 12, 26, 31]. Pregnancy presents an important opportunity for diagnosis [22, 29], but overall low rates of insurance among Africans in the US [39] along with other barriers limit opportunities for early antenatal care and HIV screening. One analysis found that foreign-born Blacks are more likely to develop AIDS within 12 months of an HIV diagnosis compared to US-born Blacks (45 vs 37 %) [7]. Late presentation for screening was also reported in New York City where more Africans presented with AIDS than did US-born persons (30 vs 22 %) and had a lower mean CD4 count at diagnosis (257 vs 352 cells/mm3) [12]. Other studies among smaller samples corroborate late presentation among African-born persons in the US [26, 31].
Outcomes
Although African-born US residents present later in the course of infection, they appear to initiate care earlier after diagnosis and also to have lower mortality and lengthier survival compared to US-born groups with HIV. African-born US residents in New York City were found to be more likely than US-born persons to initiate care within 3 months after diagnosis (76 vs 72 %) although this difference was not statistically significant (p = 0.27); and to have lower mortality than US-born persons with HIV (7.1/1,000/year vs 19.5/1,000/year), which was statistically significant (p < 0.001) [12]. Other analyses have found slightly higher survival among foreign- compared to US-born Blacks at 1 year (87 vs 85 %) and 3 years (82 vs 75 %) after an AIDS diagnosis [7].
Thus, although African-born US residents are diagnosed at later stages of infection [7, 12, 31], they paradoxically appear to have longer survival after diagnosis compared to US-born persons [7, 12]. Possible hypotheses for this discrepancy include the healthy immigrant effect persisting even in the presence of HIV/AIDS, along with a high degree of engagement and retention in care. It is important to note that these hypotheses rest on the presupposition that they outweigh social and structural barriers to screening and care identified in the studies described below.
Social Context of HIV Among Africans in the US
Six studies have explored the social context of HIV in African communities in the US [18, 22, 25, 27, 28, 30]. These studies are primarily qualitative and uncover themes that include high levels of stigma within African communities against persons living with HIV, structural barriers to screening and care, discordant beliefs and behaviors associated with misperceptions of risk and treatment, fears of deportation, and gender inequality in accessing health care resources.
The first theme, perceived stigma against people living with HIV within African communities, is described as manifesting through communal fear, avoidance of persons with HIV [18], and the belief that HIV/AIDS is a sign of moral failure and a divine punishment or “curse” [22, 25, 27, 28]. Several studies also describe how this stigma can lead to a consuming concern for privacy culminating in extreme social isolation [22, 28].
Besides stigma, several studies describe structural barriers to screening and care, including requirements for proof of residence at medical facilities, ineligibility for care due to undocumented status, language barriers, discrimination in the medical setting [22], and lack of access to education and information [27, 28].
Other studies describe how structural barriers to care are compounded by misperceptions of risk factors and treatment options. These included beliefs that HIV is transmissible through mosquito bites, coughing, sneezing, or other forms of casual contact, that treatment does not exist, and that HIV is universally a “death sentence” [25, 28]. These studies also describe how lack of knowledge of treatment is closely linked with fatalistic attitudes towards testing and seeking care [28]. Two of the studies stand out in that they surveyed well-educated immigrant groups and found a high level of knowledge of HIV/AIDS, accompanied by paradoxically elevated rates of high-risk behaviors such as unprotected sex or sexual concurrency [18, 30].
Finally, several studies report increased vulnerability for women, who described themselves as being dependent on their husbands for resources [22], handicapped by unequal access to education and information [25], and subject to more severe stigma around infection and imputed promiscuity relative to men [27].
It is relevant to note that these studies do not compare barriers to screening and care between African-born US residents and other groups. For this reason, inferences of causality cannot be drawn between these barriers and the possible earlier initiation of care and increased survival of African-born US residents described above. Additionally, these studies’ findings cannot be generalized due to their primarily qualitative nature, but they do suggest avenues for further investigations and future interventions.
Discussion
Immigration from Africa to the United States has increased more than 750 % since 1980 [5], during which time HIV/AIDS spread from a localized area in Central Africa [9] to pandemic proportions throughout the continent and beyond [1]. Despite this, surveillance reports in the US often do not include country of origin, rendering an accurate picture of the epidemic in the African-born population difficult to obtain. The available epidemiologic data [4, 7] are based on state and municipality surveillance programs and are limited in geographic scope or by a lack of demographic specificity in including either Caribbean-born Blacks [7] or Africans of Arab descent [4].
Despite the limitations of the available data, several conclusions can be drawn from the information presented above with fair confidence. First, high diagnosis rates set African-born US residents apart from the general US population. Second high rates among women, predominantly heterosexual transmission, and minimal injection-drug-use-associated transmission set African-born US residents apart from US-born Blacks [4, 7]. Third, HIV diagnosis rates among African-born US residents are half those of estimated incidence in sub-Saharan Africa. It is not known whether this is due to a predominance of immigrants from West Africa where HIV prevalence is lower than other regions of Africa, the healthy immigrant effect, underdiagnosis in the US, or differences in the statistical measures (crude diagnosis rate vs estimated incidence). African-born US residents are also diagnosed later in the course of infection than are patients from the general US population, but paradoxically appear to survive longer after diagnosis. The factors responsible for the increased survival and lower mortality among African-born US residents with HIV have not been identified, but potential hypotheses include their more rapid initiation of care after diagnosis [12], or the healthy immigrant effect (lower rates of chronic-disease-related mortality in first generation immigrants) [39–41] persisting even in the setting of HIV and AIDS [36]. Whatever the cause, late diagnosis, coupled with relatively lower mortality after diagnosis, suggests that increasing screening rates currently poses the greater public health challenge among African-born groups in the US, than do linkage and retention of diagnosed African patients in care.
Efforts to increase screening rates among African-born US residents will have to take into account the complex social and structural barriers African immigrants face in accessing care. Immigrant and undocumented status are associated with fear of health facilities [28, 42], low acculturation and unfamiliarity navigating complex health care systems [22], social and economic marginalization [43], fear of deportation [42], fatalistic views of HIV [28, 42], and a lower rate of health insurance [39], all of which pose further barriers to accessing screening services. For those aware of their status and those considering testing, the challenges of being both an African immigrant in the US and a person living with HIV in a tight-knit community can render screening, initiating, and staying in care a daunting prospect [22, 27–29].
Conclusion
Although it is clear that the number of Africans living in the US is increasing rapidly and that they carry a greater burden of HIV/AIDS than the general US population, many gaps remain in the knowledge of the epidemiology of HIV in this population [4, 7]. Africans living in the US experience higher overall HIV diagnosis rates, especially higher rates among women, and higher rates of heterosexual transmission than the general US population [4, 7]. Africans with HIV are also diagnosed at a later stage of infection than US-born persons, although they appear to survive longer after diagnosis. Meeting the distinct needs of Africans in the US with respect to HIV is further complicated by structural barriers to care, including undocumented status, language, and a low level of acculturation [18, 22, 25, 27, 28, 30]. Social barriers, such as stigma against people living with HIV within highly cohesive communities, fatalistic attitudes towards testing and treatment, unequal access to health services between genders, and high levels of diversity between the many different African communities, all highlight the difficulty of increasing access to diagnosis and care [18, 22, 25, 27, 28, 30]. But while the growing population, the lack of accurate estimates of incidence, and the distinct set of social and structural barriers all illustrate the complexity of improving HIV screening and care services for this population, they also highlight the importance of further research and public health programming to address it.
References
UNAIDS. World AIDS day report. Geneva; 2011.
UNAIDS. UNAIDS report on the global AIDS epidemic. Geneva: United Nations; 2010.
Europe. ECfDPaCWROf. HIV/AIDS surveillance in Europe 2009. Stockholm: European Centre for Disease Prevention and Control; 2010.
Kerani RP, Kent JB, Sides T, et al. HIV among African-born persons in the United States: a hidden epidemic? J Acquir Immune Defic Syndr. 2008;49(1):102–6.
McCabe K. African immigrants in the United States. Washington, DC: Migration Policy Institute; 2011.
CDC. HIV prevalence estimates—United States, 2006. MMWR Morb Mortal Wkly Rep. 2008;57(39):1073–6.
Johnson AS, Hu X, Dean HD. Epidemiologic differences between native-born and foreign-born black people diagnosed with HIV infection in 33 U.S. states, 2001–2007. Public Health Rep. 2010;125(Suppl 4):61–9.
Sutton MY, Jones RL, Wolitski RJ, Cleveland JC, Dean HD, Fenton KA. A review of the centers for disease control and prevention’s response to the HIV/AIDS crisis among Blacks in the United States, 1981–2009. Am J Public Health. 2009;99(Suppl 2):S351–9.
Pépin J. The origins of AIDS. Cambridge: Cambridge University Press; 2011.
Terrazas A. African immigrants in the United States. Washington, DC: Migration Policy Institute; 2009.
Census U. American Community Survey. Selected Population Profile in the United States. Subsaharan African. New York City; 2006.
NYCDOHMH. HIV/AIDS in foreign-born New Yorkers. New York: HIV Epidemiology and Field Services Program New York City Department of Health and Mental Hygiene; 2009.
Singh GK, Hiatt RA. Trends and disparities in socioeconomic and behavioural characteristics, life expectancy, and cause-specific mortality of native-born and foreign-born populations in the United States, 1979–2003. Int J Epidemiol. 2006;35(4):903–19.
Heine B, Nurse D. African languages: an introduction. Cambridge: Cambridge University Press; 2000.
Fairchild AL, Tynan EA. Policies of containment: immigration in the era of AIDS. Am J Public Health. 1994;84(12):2011–22.
Neilson V, Masliah N. AILA practice advisory on the end of the HIV ban. Washington, DC: American Immigration Lawyers Association; 2009.
U.S. Congress upholds ban on HIV carriers. Annals of oncology: official journal of the European society for medical oncology/ESMO. 1993;4(8):616.
Rosenthal L, Scott DP, Kelleta Z, et al. Assessing the HIV/AIDS health services needs of African immigrants to Houston. AIDS Educ Prev. 2003;15(6):570–80.
CDC. Final rule removing HIV infection from U.S. immigration screening. 2010; http://www.cdc.gov/immigrantrefugeehealth/laws-regs/hiv-ban-removal/final-rule.html. Accessed 4 Oct 2011.
Jenny-Avital ER, Beatrice ST. Erroneously low or undetectable plasma human immunodeficiency virus type 1 (HIV-1) ribonucleic acid load, determined by polymerase chain reaction, in West African and American patients with non-B subtype HIV-1 infection. Clin Infect Dis. 2001;32(8):1227–30.
Harawa NT, Bingham TA, Cochran SD, Greenland S, Cunningham WE. HIV prevalence among foreign- and US-born clients of public STD clinics. Am J Public Health. 2002;92(12):1958–63.
Foley EE. HIV/AIDS and African immigrant women in Philadelphia: structural and cultural barriers to care. AIDS Care. 2005;17(8):1030–43.
Kent JB. Impact of foreign-born persons on HIV diagnosis rates among Blacks in King County, Washington. AIDS Educ Prev. 2005;17(6 Suppl B):60–7.
Cartwright CP. The changing epidemiology of HIV/AIDS at a Minnesota hospital: impact of demographic change and viral diversity. J Med Virol. 2006;78(Suppl 1):S19–21.
Tompkins M, Smith L, Jones K, Swindells S. HIV education needs among Sudanese immigrants and refugees in the Midwestern United States. AIDS Behav. 2006;10(3):319–23.
Akinsete OO, Sides T, Hirigoyen D, et al. Demographic, clinical, and virologic characteristics of African-born persons with HIV/AIDS in a Minnesota hospital. AIDS Patient Care STDS. 2007;21(5):356–65.
De Jesus M. HIV/AIDS and immigrant Cape Verdean women: contextualized perspectives of Cape Verdean community advocates. Am J Community Psychol. 2007;39(1–2):121–31.
Othieno J. Understanding how contextual realities affect African born immigrants and refugees living with HIV in accessing care in the Twin Cities. J Health Care Poor Underserved. 2007;18(3 Suppl):170–88.
Blood E, Beckwith C, Bazerman L, Cu-Uvin S, Mitty J. Pregnancy among HIV-infected refugees in Rhode Island. AIDS Care. 2009;21(2):207–11.
Mitha K, Yirsalign M, Cherner M, McCutchan A, Langford TD. Risk perception and beliefs regarding HIV infection among Ethiopian immigrants. AIDS Educ Prev. 2009;21(5):484–94.
Page LC, Goldbaum G, Kent JB, Buskin SE. Access to regular HIV care and disease progression among black African immigrants. J Natl Med Assoc. 2009;101(12):1230–6.
Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA. 2008;300(5):520–9.
CDC. Subpopulation estimates from the HIV incidence surveillance system—United States, 2006. MMWR Morb Mortal Wkly Rep. 2008;57(36):985–9.
Voelker R. HIV/AIDS in the Caribbean: big problems among small islands. JAMA. 2001;285(23):2961–3.
Thomas KJ. A demographic profile of Black Caribbean immigrants to the United States. Washington, DC: Migration Policy Institute; 2012.
Venters H, Gany F. African immigrant health. J Immigr Minor Health. 2011;13(2):333–44.
Mocroft A, Vella S, Benfield TL, et al. Changing patterns of mortality across Europe in patients infected with HIV-1. EuroSIDA Study Group. Lancet. 1998;352(9142):1725–30.
Moore RD. Epidemiology of HIV infection in the United States: implications for linkage to care. Clin Infect Dis. 2011;52(Suppl 2):S208–13.
Lucas JW, Barr-Anderson DJ, Kington RS. Health status, health insurance, and health care utilization patterns of immigrant Black men. Am J Public Health. 2003;93(10):1740–7.
Abraido-Lanza AF, Dohrenwend BP, Ng-Mak DS, Turner JB. The Latino mortality paradox: a test of the “salmon bias” and healthy migrant hypotheses. Am J Public Health. 1999;89(10):1543–8.
Kenya S, Brodsky M, Divale W, Allegrante JP, Fullilove RE. Effects of immigration on selected health risk behaviors of Black college students. J Am Coll Health. 2003;52(3):113–20.
Blanas D, Lugg A. Barriers to accessing healthcare among undocumented HIV+ African immigrants in New York City: how fear of disclosure impacts behavior and health. Paper presented at: American Public Health Association Conference 2011; Washington, DC.
Adimora AA, Schoenbach VJ. Social context, sexual networks, and racial disparities in rates of sexually transmitted infections. J Infect Dis. 2005;191(Suppl 1):S115–22.
Bank W. World Population. 2010; http://ddp-ext.worldbank.org/ext/ddpreports/ViewSharedReport?&CF=&REPORT_ID=9147&REQUEST_TYPE=VIEWADVANCED&HF=N/CPProfile.asp&WSP=N. Accessed 21 Apr 2012.
UNAIDS. Report on the global HIV/AIDS epidemic update. Geneva: UNAIDS; 2005.
Acknowledgments
Ellen Wiewel MHS and Andrew Jensen reviewed and commented on the manuscript. Alice Clomegah, Goytia Crispin, Lea Rivera-Todaro provided important insights. This work was supported in part by a grant from the Doris Duke Charitable Foundation to the Mount Sinai School of Medicine to fund Clinical Research Fellow Demetri Blanas, MPH. This work was supported by grant UL1TR000067 from the National Center for Research Resources, National Institutes of Health to fund Carol R Horowitz, MD-MPH.
Conflict of interest
There is no conflict of interest with any of the authors: There are no financial, commercial, or other forms of connection between the authors and any commercial or industrial interest. No party stands to gain financially from the publication of this work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Blanas, D.A., Nichols, K., Bekele, M. et al. HIV/AIDS Among African-Born Residents in the United States. J Immigrant Minority Health 15, 718–724 (2013). https://doi.org/10.1007/s10903-012-9691-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-012-9691-6