
Abstract
Introduction
The optimal management of high risk WHO grade II gliomas after surgery is debated including the role of initial temozolomide to delay radiotherapy and risk of cognitive defects.
Methods
A post-hoc analysis of a phase II multicenter study on high risk WHO grade II gliomas, receiving initial temozolomide alone, has re-evaluated the long-term results within the molecular subgroups of WHO 2016. The primary endpoint of the study was response according to RANO, being seizure response, PFS and OS secondary endpoints.
Results
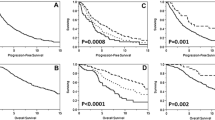
Response rate among oligodendrogliomas IDH-mutant and 1p/19q codeleted (76%) was significantly higher than that among diffuse astrocytomas either mutant (55%) or wild-type (36%). A reduction of seizure frequency > 50% was observed in 87% of patients and a seizure freedom in 72%. The probability of seizure reduction > 50% was significantly associated with the presence of an IDH mutation. Median PFS, PFS at 5 and 10 years, median OS and OS at 5 and 10 years were significantly longer in oligodendrogliomas IDH-mutant and 1p/19q codeleted. Sixty-seven percent of patients with oligodendroglioma IDH mutant and 1p/19q codeleted did not recur with a median follow up of 9.3 years, while 59% did not receive radiotherapy at recurrence with a median follow up of 8.2 years.
Conclusions
The beneficial effects of initial temozolomide prevail in oligodendrogliomas IDH-mutant and 1p/19q codeleted: thus, these tumors, when incompletely resected or progressive after surgery alone, or with intractable seizures, should receive temozolomide as initial treatment with salvage radiotherapy and/o reoperation and/or second-line chemotherapy at recurrence.

Similar content being viewed by others


Change history
05 November 2019
The third and fourth authors' affiliation was incorrectly specified in the original publication. It is correctly shown here.
References
van den Bent MJ, Afra D, de Witte O et al (2005) Long-term efficacy of early versus delayed radiotherapy for low-grade astrocytoma and oligodendroglioma in adults: the EORTC 22845 randomised trial. Lancet 366(9490):985–990
Buckner JC, Shaw EG, Pugh SL et al (2016) Radiation plus procarbazine, CCNU, and vincristine in low-grade glioma. N Engl J Med 374(14):1344–1355
Douw L, Klein M, Fagel SS et al (2009) Cognitive and radiological effects of radiotherapy in patients with low-grade glioma: long-term follow-up. Lancet Neurol 8(9):810–818
Brada M, Viviers L, Abson C et al (2003) Phase II study of primary temozolomide chemotherapy in patients with WHO grade II gliomas. Ann Oncol 14(12):1715–1721
Wahl M, Phillips JJ, Molinaro AM et al (2017) Chemotherapy for adult low-grade gliomas: clinical outcomes by molecular subtype in a phase II study of adjuvant temozolomide. Neuro-Oncology 19(2):242–251
Pouratian N, Gasco J, Sherman JH et al (2007) Toxicity and efficacy of protracted low dose temozolomide for the treatment of low grade gliomas. J Neurooncol 82(3):281–288
Kesari S, Schiff D, Drappatz J et al (2009) Phase II study of protracted daily temozolomide for low-grade gliomas in adults. Clin Cancer Res 15(1):330–337
Baumert BG, Hegi ME, van den Bent MJ et al (2016) Temozolomide chemotherapy versus radiotherapy in high-risk low-grade glioma (EORTC 22033–26033): a randomised, open-label, phase 3 intergroup study. Lancet Oncol 17(11):1521–1532
Pellerino A, Franchino F, Pace A et al. (2017) Temozolomide (TMZ) 1 week on/1 week off as initial treatment for high risk low grade oligodendroglial tumors: a phase II AINO (Italian Association for Neuro-Oncology) study. Neuro Oncol 19(suppl_3):iii21
Louis DN, Perry A, Reifenberger G et al (2016) The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol 131(6):803–820
van den Bent MJ, Wefel JS, Schiff D et al (2011) Response assessment in neuro-oncology (a report of the RANO group): assessment of outcome in trials of diffuse low-grade gliomas. Lancet Oncol 12(6):583–593
Hoang-Xuan K, Capelle L, Kujas M et al (2004) Temozolomide as initial treatment for adults with low-grade oligodendrogliomas or oligoastrocytomas and correlation with chromosome 1p deletions. J Clin Oncol 22(15):3133–3138
Avila EK, Chamberlain M, Schiff D et al (2017) Seizure control as a new metric in assessing efficacy of tumor treatment in low-grade glioma trials. Neuro-Oncology 19(1):12–21
Kaloshi G, Benouaich-Amiel A, Diakite F et al (2007) Temozolomide for low-grade gliomas: predictive impact of 1p/19q loss on response and outcome. Neurology 68(21):1831–1836
Sherman JH, Moldovan K, Yeoh HK et al (2011) Impact of temozolomide chemotherapy on seizure frequency in patients with low-grade gliomas. J Neurosurg 114(6):1617–1621
Koekkoek JA, Dirven L, Heimans JJ et al (2015) Seizure reduction in a low-grade glioma: more than a beneficial side effect of temozolomide. J Neurol Neurosurg Psychiatry 86(4):366–373
Rudà R, Magliola U, Bertero L et al (2013) Seizure control following radiotherapy in patients with diffuse gliomas: a retrospective study. Neuro-Oncology 15(12):1739–1749
Stockhammer F, Misch M, Helms HJ et al (2012) IDH1/2 mutations in WHO grade II astrocytomas associated with localization and seizure as the initial symptom. Seizure 21(3):194–197
Liubinas SV, D'Abaco GM, Moffat BM et al (2014) IDH1 mutation is associated with seizures and protoplasmic subtype in patients with low-grade gliomas. Epilepsia 55(9):1438–1443
Donovan LE, Lassman AB (2019) Chemotherapy Treatment and Trials in Low-Grade Gliomas. Neurosurg Clin N Am 30(1):103–109
Jhaveri J, Liu Y, Chowdhary M et al (2018) Is less more? Comparing chemotherapy alone with chemotherapy and radiation for high-risk grade 2 glioma: an analysis of the National Cancer Data Base. Cancer 124(6):1169–1178
Houillier C, Wang X, Kaloshi G et al (2010) IDH 1 or IDH2 mutations predict longer survival and response to temozolomide in low-grade gliomas. Neurology 75(17):1560–1566
Leu S, von Felten S, Frank S et al (2013) IDH/MGMT-driven molecular classification of low-grade glioma is a strong predictor for long-term survival. Neuro-Oncology 15(4):469–479
Bell EH, Zhang P, Fisher BJ et al (2018) Association of MGMT promoter methylation status with survival Outcomes in Patients With High-Risk Glioma Treated With Radiotherapy and Temozolomide: An Analysis From the NRG Oncology/RTOG 0424 Trial. JAMA Oncol 4(10):1405–1409
Johnson BE, Mazor T, Hong C et al (2014) Mutational analysis reveals the origin and therapy-driven evolution of recurrent glioma. Science 343(6167):189–193
Funding
None.
Author information
Authors and Affiliations
Contributions
Conception and design: Roberta Rudà, Alessia Pellerino, Riccardo Soffietti. Provision of study materials or patients: All authors. Collection and assembly of data: Alessia Pellerino, Giulia Marchese. Statistical analysis: Enrica Migliore. Article writing: Roberta Rudà, Alessia Pellerino, Riccardo Soffietti. Final approval of article: All authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Rudà, R., Pellerino, A., Pace, A. et al. Efficacy of initial temozolomide for high-risk low grade gliomas in a phase II AINO (Italian Association for Neuro-Oncology) study: a post-hoc analysis within molecular subgroups of WHO 2016. J Neurooncol 145, 115–123 (2019). https://doi.org/10.1007/s11060-019-03277-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-019-03277-x