
Abstract
Purpose
Treatment-related symptom burden varies significantly among patients undergoing radiotherapy or chemoradiotherapy, yet such variation is typically not reflected in the results from single-group studies. We applied group-based trajectory modeling (GBTM) to describe the heterogeneity of symptom burden among patients with head and neck cancer and to identify subgroups with distinct symptom-development trajectories.
Methods
Patients (n = 130) were recruited pretherapy and rated multiple symptoms weekly for 10 weeks via the M. D. Anderson Symptom Inventory. With the mean of five most severe symptoms over time as an outcome measure, GBTM was used to identify patient subgroups with distinct symptom trajectories. Linear mixed-effects modeling (LMM) was applied to compare with GBTM’s ability to describe the longitudinal symptom data.
Results
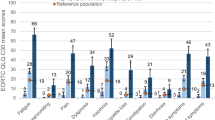
The five most severe symptoms were problems with taste, difficulty swallowing or chewing, problems with mucus, fatigue, and dry mouth. A two-group GBTM model identified 68 % of patients as having high symptom burden, associated with older age, worse baseline performance status, and chemoradiotherapy treatment. A four-group GBTM model generated one stable group (4 % of patients) and three groups varying in symptom severity with both linear and quadratic functions over time. LMM revealed symptom-change patterns similar to that produced by GBTM but was inferior in identifying risk factors for high symptom burden.
Conclusions
For cancer patients undergoing aggressive therapy, GBTM is capable of identifying various symptom-burden trajectories and provides severity groupings that will aid research and may be of clinical utility. These results may be generalizable to other cancer types and treatments.

Similar content being viewed by others


References
Haigentz, M, Jr, Corry, J., Strojan, P., & Ferlito, A. (2012). Easing acceleration of head and neck chemoradiotherapy. Lancet Oncology, 13(2), 113–115.
Rosenthal, D. I., Mendoza, T., & Cleeland, C. (2009). Identifying head and neck patients at risk for high symptom burden during treatment [abstract]. American society of clinical oncology 2009 annual meeting, Orlando, FL, May 29–Jun 2, 2009. Journal of Clinical Oncology, 27(15 Suppl). Abstract #6066.
Dodd, M. J., Cho, M. H., Cooper, B. A., & Miaskowski, C. (2010). The effect of symptom clusters on functional status and quality of life in women with breast cancer. European Journal of Oncology Nursing, 14(2), 101–110.
Miaskowski, C., Cooper, B. A., Paul, S. M., Dodd, M., Lee, K., Aouizerat, B. E., et al. (2006). Subgroups of patients with cancer with different symptom experiences and quality-of-life outcomes: a cluster analysis. Oncology Nursing Forum, 33(5), E79–E89.
Shi, Q., Smith, T. G., Michonski, J. D., Stein, K. D., Kaw, C., & Cleeland, C. S. (2011). Symptom burden in cancer survivors 1 year after diagnosis: a report from the American Cancer Society’s Studies of Cancer Survivors. Cancer, 117(12), 2779–2790.
Nylund, K., Bellmore, A., Nishina, A., & Graham, S. (2007). Subtypes, severity, and structural stability of peer victimization: what does latent class analysis say? Child Development, 78(6), 1706–1722.
Dodd, M. J., Cho, M. H., Cooper, B. A., Petersen, J., Bank, K. A., Lee, K. A., et al. (2011). Identification of latent classes in patients who are receiving biotherapy based on symptom experience and its effect on functional status and quality of life. Oncology Nursing Forum, 38(1), 33–42.
Wang, X. S., Fairclough, D. L., Liao, Z., Komaki, R., Chang, J. Y., Mobley, G. M., et al. (2006). Longitudinal study of the relationship between chemoradiation therapy for non-small-cell lung cancer and patient symptoms. Journal of Clinical Oncology, 24(27), 4485–4491.
Langford, D. J., Tripathy, D., Paul, S. M., West, C., Dodd, M. J., Schumacher, K., et al. (2011). Trajectories of pain and analgesics in oncology outpatients with metastatic bone pain. Journal of pain, 12(4), 495–507.
Merriman, J. D., Jansen, C., Koetters, T., West, C., Dodd, M., Lee, K., et al. (2010). Predictors of the trajectories of self-reported attentional fatigue in women with breast cancer undergoing radiation therapy. Oncology Nursing Society, 37(4), 423–432.
Klepstad, P., Dale, O., Kaasa, S., Zahlsen, K., Aamo, T., Fayers, P., et al. (2003). Influences on serum concentrations of morphine, M6G and M3G during routine clinical drug monitoring: a prospective survey in 300 adult cancer patients. Acta Anaesthesiologica Scandinavica, 47(6), 725–731.
Nagin, D. S. (2005). Group-based modeling of development. Cambridge, MA: Harvard University Press.
Nagin, D. S., & Tremblay, R. E. (2001). Analyzing developmental trajectories of distinct but related behaviors: a group-based method. Psychological Methods, 6(1), 18–34.
Brame, B., Nagin, D. S., & Tremblay, R. E. (2001). Developmental trajectories of physical aggression from school entry to late adolescence. Journal of Child Psychology and Psychiatry, 42(4), 503–512.
Côté, S. M., Boivin, M., Liu, X., Nagin, D. S., Zoccolillo, M., & Tremblay, R. E. (2009). Depression and anxiety symptoms: onset, developmental course and risk factors during early childhood. Journal of Child Psychology and Psychiatry, 50(10), 1201–1208.
Modi, A. C., Cassedy, A. E., Quittner, A. L., Accurso, F., Sontag, M., Koenig, J. M., et al. (2010). Trajectories of adherence to airway clearance therapy for patients with cystic fibrosis. Journal of Pediatric Psychology, 35(9), 1028–1037.
Cleeland, C. S., Mendoza, T. R., Wang, X. S., Woodruff, J. F., Palos, G. R., Richman, S. P., et al. (2011). Levels of symptom burden during chemotherapy for advanced lung cancer: differences between public hospitals and a tertiary cancer center. Journal of Clinical Oncology, 29(21), 2859–2865.
Rosenthal, D. I., Asper, J. A., Barker, J. L, Jr, Garden, A. S., Chao, K. S., Morrison, W. H., et al. (2006). Importance of patient examination to clinical quality assurance in head and neck radiation oncology. Head and Neck, 28(11), 967–973.
Cleeland, C. S., Mendoza, T. R., Wang, X. S., Chou, C., Harle, M. T., Morrissey, M., et al. (2000). Assessing symptom distress in cancer patients: the M.D. Anderson Symptom Inventory. Cancer, 89(7), 1634–1646.
Rosenthal, D. I., Mendoza, T. R., Chambers, M. S., Asper, J. A., Gning, I., Kies, M. S., et al. (2007). Measuring head and neck cancer symptom burden: the development and validation of the M. D. Anderson symptom inventory, head and neck module. Head and Neck, 29(10), 923–931.
Jones, B. L. (2005). TRAJ: group-based modeling of longitudinal data. http://www.andrew.cmu.edu/user/bjones/. Accessed 22 May 2012.
Lo, Y. T., Mendell, N. R., & Rubin, D. B. (2001). Testing the number of components in a normal mixture. Biometrika, 88(3), 767–778.
Rosenthal, D. I., Mendoza, T. R., Chambers, M. S., Burkett, V. S., Garden, A. S., Hessell, A. C., et al. (2008). The M. D. Anderson symptom inventory-head and neck module, a patient-reported outcome instrument, accurately predicts the severity of radiation-induced mucositis. International Journal of Radiation Oncology Biology Physics, 72(5), 1355–1361.
Budach, W., Hehr, T., Budach, V., Belka, C., & Dietz, K. (2006). A meta-analysis of hyperfractionated and accelerated radiotherapy and combined chemotherapy and radiotherapy regimens in unresected locally advanced squamous cell carcinoma of the head and neck. BMC Cancer, 6, 28.
Muthén, B. (2003). Statistical and substantive checking in growth mixture modeling: Comment on Bauer and Curran (2003). Psychological Methods, 8(3), 369–377.
Muthén, B. (2004). Latent variable analysis: growth mixture modeling and related techeniques for longitudinal data. In D. Kaplan (Ed.), The SAGE handbook of quantitative methodology for the social sciences (pp. 345–368). Thousand Oaks, CA: Sage Publications, Inc.
Tarpey, T., Yun, D., & Petkova, E. (2008). Model misspecification: finite mixture or homogeneous? Statistical Modelling, 8(2), 199–218.
Bauer, D. J., & Curran, P. J. (2003). Distributional assumptions of growth mixture models: Implications for overextraction of latent trajectory classes. Psychological Methods, 8(3), 338–363.
Acknowledgments
The project described was supported by awards from the National Institutes of Health: Award Number CA016672, a Cancer Center Support Grant to The University of Texas MD Anderson Cancer Center, and Award Number CA026582 to Charles S. Cleeland, PhD. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health. The authors acknowledge the editorial assistance of Jeanie F. Woodruff, BS, ELS.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shi, Q., Mendoza, T.R., Gunn, G.B. et al. Using group-based trajectory modeling to examine heterogeneity of symptom burden in patients with head and neck cancer undergoing aggressive non-surgical therapy. Qual Life Res 22, 2331–2339 (2013). https://doi.org/10.1007/s11136-013-0380-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-013-0380-2