
Abstract
Background
For people with diabetes, adherence to prescribed medications is essential. However, the rising prevalence of high-deductible health plans (HDHPs), and prices of diabetes medications such as insulin, could deter adherence.
Objective
To assess the impact of HDHP on cost-related medication non-adherence (CRN) among non-elderly adults with diabetes in the US.
Design
Repeated cross-sectional survey.
Setting
National Health Interview Survey, 2011–2018.
Participants
A total of 7469 privately insured adults ages 18–64 with diabetes who were prescribed medications and enrolled in a HDHP or a traditional commercial health plan (TCP).
Main Measures
Self-reported measures of CRN were compared between enrollees in HDHPs and TCPs overall and among the subset using insulin. Analyses were adjusted for demographic and clinical characteristics using multivariable linear regression models.
Key Results
HDHP enrollees were more likely than TCP enrollees to not fill a prescription (13.4% vs 9.9%; adjusted percentage point difference (AD) 3.4 [95% CI 1.5 to 5.4]); skip medication doses (11.4% vs 8.5%; AD 2.8 [CI 1.0 to 4.7]); take less medication (11.1% vs 8.8%; AD 2.3 [CI 0.5 to 4.0]); delay filling a prescription to save money (14.4% vs 10.8%; AD 3.0 [CI 1.1 to 4.9]); and to have any form of CRN (20.4% vs 15.5%; AD 4.4 [CI 2.2 to 6.7]). Among those taking insulin, HDHP enrollees were more likely to have any CRN (25.1% vs 18.9%; AD 5.9 [CI 1.1 to 10.8]).
Conclusion
HDHPs are associated with greater CRN among people with diabetes, particularly those prescribed insulin. For people with diabetes, enrollment in non-HDHPs might reduce CRN to prescribed medications.
Similar content being viewed by others
INTRODUCTION
Adherence to hypoglycemic medications for people with diabetes is essential for maintaining glycemic control,1,2,3,4 reducing hospitalizations,5,6,7 and preventing long-term complications.3,8 Out-of-pocket costs for prescribed medications are strongly associated with patients taking less medication than prescribed.9,10,11 Such cost-related medication non-adherence (CRN) is common among patients with diabetes,3,12,13,14,15 particularly those with low incomes.14,16,17 Prices for hypoglycemic medications, especially insulin, have been increasing substantially in recent years.18,19,20 Between 2002 and 2013, for example, the mean price of insulin rose by over 200%.18 This price increase has resulted in a substantial rise in out-of-pocket costs for medications to treat diabetes.21
High deductible health plans (HDHPs), which can substantially increase out-of-pocket costs, are increasingly common.22 These plans require potential out-of-pocket spending of $1000 to $7000 per person annually for non-preventive care. For commercially insured patients with diabetes, HDHP enrollment has been associated with increased out-of-pocket medical expenditures23,24,25,26 and reductions in receipt of some forms of outpatient care among lower income individuals, including primary care and specialty visits.16 Additionally, HDHPs are associated with delays in seeking treatment for macrovascular complications of diabetes,27 and with CRN and forgone care among those with other chronic illnesses.28,29 However, to date, no studies have quantified the effect of HDHP enrollment on CRN among patients with diabetes in the US.
We analyzed nationally representative data on non-elderly adults with diabetes enrolled in private health plans to assess (1) the association between HDHP enrollment and multiple measures of CRN among those taking any prescribed medication and the subset taking insulin; (2) the effect of income level on this association; and (3) the relationship between CRN and the risk of experiencing two adverse outcomes, emergency department visits and hospitalizations.
METHODS
Data Source and Study Population
We analyzed the National Health Interview Survey (NHIS) from 2011 to 2018. This is a cross-sectional, household interview survey of a nationally representative sample of the noninstitutionalized US population. The NHIS uses a complex, multistage area probability sample design. The NHIS is conducted annually by the National Center for Health Statistics through in-person interviews with approximately 35,000 families. All family members are invited to participate, and only one adult in each family is randomly selected to complete a more extensive interview. Details of the structure, sampling frame, and survey items have been published previously.30 The total household response rate for the NHIS during the study years ranged from 82.0% in 2011 to 64.2% in 2018.30
The study sample included non-elderly adults (ages 18–64) who reported having a diagnosis of diabetes (an affirmative response to the question: “Have you ever been told by a doctor or other health professional that you have diabetes or sugar diabetes?”) and being enrolled in a commercial health insurance plan. We excluded from the study sample individuals with a commercial plan if they also had any other form of insurance (Medicaid, Medicare, Veterans’ Administration coverage, etc.). Respondents who were 65 years of age or older, and therefore eligible for Medicare, were also excluded. We also excluded the small number of respondents that had missing data for any outcome of the study.
Study Variables
Respondents in the NHIS were deemed to have a HDHP if they indicated that their commercial health plan had an annual individual deductible of $1300 per year or more or a family deductible of $2400 per year or more during the years 2011–2014 and $2600 per year or more during the years 2015–2018. Respondents were considered to have a traditional commercial health plan (TCP) if their annual individual deductible was less than these values. Cost-related medication non-adherence (CRN) was assessed using responses to four survey questions. Participants were asked if, in the last 12 months, they (1) could not afford prescription medications; (2) skipped medication doses to save money; (3) took less medicine to save money; or (4) delayed filling a prescription for a medication to save money. In addition, we constructed a composite measure for which experiencing any CRN was defined as answering “yes” to at least one of these individual items. CRN has been linked to adverse outcomes in patients with diabetes31 but not in a nationally representative sample. Thus to assess the importance of CRN as an outcome in this population, we also examined two potential adverse consequences of CRN: (1) having 1 or more emergency department visits in the last 12 months (this includes emergency room visits that resulted in a hospital admission); and (2) having 1 or more hospitalizations. We considered respondents to be insulin users if they answered affirmatively to the question “Insulin can be taken by shot or pump. Are you now taking insulin?”
We obtained information on self-reported health status (those with excellent, very good, or good health were categorized as “good” while those with fair or poor health were categorized as “poor”) and the presence of health limitations (physical, mental, or emotional problem requiring the help of other persons with personal care needs). NHIS also assesses the presence of the following set of common chronic medical conditions: diabetes, hypertension, cardiovascular disease (with questions about coronary heart disease, angina, myocardial infarction, and other heart disease), chronic obstructive pulmonary disease (with questions about chronic bronchitis, emphysema, and, from 2012 onward, COPD), stroke, and kidney disease. We also obtained information on the following demographic variables and treated them analytically as indicated in parentheses: age (continuous), race (Hispanic, white, black, Asian, or other), family size (1, 2, 3, 4, or more), marital status (currently married vs not married), health status (good or poor), education status (less than high-school, high-school degree, college degree, postgraduate degree), employment status (employed or not), and annual family income: lowest-income ($0–$34,999), low-income ($35,000–$74,999), middle-income ($75,000–$99,999), and high-income ($100,000 or more).
Analyses
We compared baseline characteristics of the study population between respondents enrolled in a HDHP and those enrolled in a TCP. We then examined the relationship between HDHP enrollment (vs TCP enrollment) and CRN among the entire cohort (“all diabetics”) and the subset of those taking insulin (“insulin users”). For all diabetics and for insulin users, we calculated the proportion of individuals in both HDHPs and TCPs that reported experiencing each of the four individual CRN measures and the composite, “any CRN” measure. We then examined the association of HDHP status with CRN by estimating the adjusted percentage point difference between HDHP enrollees and TCP enrollees for each CRN outcome measure using multiple linear probability regression models that included terms for the presence of each chronic medical condition, age, sex, family size, race/ethnicity, marital status, health status, presence of a functional limitation, education level, income group, and employment status.
In order to assess the effect of income on the relationship between HDHP enrollment and CRN, we stratified the study sample by income group and replicated the above analysis for any CRN outcome, except that for these models, we excluded the term for income.
We also examined the relationship between experiencing any CRN and having an emergency room visit (1 or more) or hospitalization (1 or more) in the last year by estimating the adjusted percentage point difference for each outcome between those with and without CRN using the same modelling approach as described above. In addition, because the association between CRN and these outcomes could be influenced by enrollment in a HDHP (vs a TCP), in a sensitivity analysis, we additionally controlled for enrollment in a HDHP. This did not alter any of our findings and thus we do not report these analyses further.
Although our study population was comprised entirely of people with diabetes, the CRN questions were not specific to diabetes medications. To assess the extent to which CRN to non-diabetic medications influenced our results, we conducted 2 additional sensitivity analyses in which we excluded those respondents who reported having any chronic condition other than diabetes. We replicated the analyses of the association between HDHP and CRN and the association between CRN and emergency department visits and hospitalizations described above, including only people with diabetes but no other chronic condition.
For all analyses, we applied survey weights provided by NHIS in order to produce nationally representative estimates. Statistical significance was assigned at the p<0.05 level. Categorical variables were analyzed using chi-square tests of independence. We used STATA (version 15.1) for all analyses. The Cambridge Health Alliance Internal Review Board deemed this study exempt from human subjects review.
RESULTS
Sample
The Supplement Figure illustrates how our study population was formed. The final study population included 7469 adults, 2691 with a HDHP, and 4778 with a TCP.
Demographics
We found that HDHP enrollees and TCP enrollees did not differ with respect to age, sex, family size, marital status, health status, and family income (Table 1). However, HDHP enrollees were more likely than TCP enrollees to identify as white (69.7% vs 62.9%, p<0.01), be employed (83.0% vs 79.3%, p<0.01), have a college education (21.3% vs 18.2%, p<0.01), and report a functional limitation (53.5% vs 49.9%, p<0.05).
Association Between HDHP Enrollment and Cost-Related Medication Non-adherence
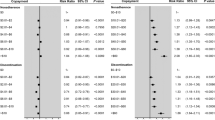
HDHP enrollees were more likely than TCP enrollees to be unable to afford a prescription medication (13.4% vs 9.9%; AD 3.4 [95% CI 1.5 to 5.4]); to skip a medication to save money (11.4% vs 8.5%; AD 2.8 [CI 1.0 to 4.7]); take less medication (11.1% vs 8.8%; AD 2.3 [CI 0.5 to 4.0]); and delay filling a prescription (14.4% vs 10.8%; AD 3.0 [CI 1.1 to 4.9]) (Table 2). HDHP enrollees were also more likely to have any CRN (20.4% vs 15.5%; AD 4.4 [CI 2.2 to 6.7], a 28% relative increase). Among insulin users, HDHP enrollees were more likely than TCP enrollees to have any CRN (25.1% vs 18.9%; AD 5.9% [CI 1.1 to 10.8], a 31% relative increase). While the point estimates for proportions of enrollees experiencing each of the remaining individual CRN measures were higher for HDHP enrollees, they did not achieve statistical significance.
In analyses stratified by income level, we found that the proportion of respondents having any CRN was substantially greater among lower income compared with higher income respondents, with approximately one-third of those in HDHPs and TCPs in the lowest-income group reporting any CRN, for the overall and insulin user sub-population (Table 3). The magnitude of the point estimates for differences between HDHP enrollees and TCP enrollees was small and non-significant for the lowest income group and larger for the remaining 3 income groups among all people with diabetes and the insulin user groups. Among all diabetics, HDHP enrollees were more likely than TCP enrollees to have any CRN in the low-income group (26.1% vs 19.7%; AD 5.4 [CI 1.5 to 9.3]) and high-income group (10.7% vs 6.1%; AD 4.5 [CI 1.1 to 8.0]). No statistically significant difference was observed for the remaining income categories. Among insulin users, we observed a similar pattern.
Association of Cost-Related Medication Non-adherence with Emergency Department Visits and Hospitalizations
Among all diabetics, those reporting any CRN were more likely to have 1 or more emergency department visits (34.1% vs 20.6%; AD 5.5 [CI 2.1 to 8.9]) but not hospitalizations (Table 4). Among insulin users, those reporting any CRN were also more likely to have 1 or more emergency department visits (43.7% vs 24.6%; AD 11.2 [CI 4.4 to 18.1]) but not hospitalizations.
Sensitivity Analyses
When we replicated our analysis of the association between HDHP status and any CRN excluding those with chronic diseases other than diabetes, the point estimates for adjusted differences were comparable to the main analyses, although the difference for insulin users was no longer statistically significant (Supplement Table 1). When we replicated our analysis on the association of any CRN with emergency department visits and hospitalizations, the adjusted differences were again comparable and maintained the same pattern of statistical significance (Supplement Table 2).
DISCUSSION
In this nationally representative observational study of commercially insured non-elderly adults with diabetes, we found that enrollment in a HDHP was associated with greater CRN, with larger effects among insulin users. We also observed that among the lowest income group, approximately one-third of all diabetic patients and the insulin using subgroup experienced CRN. Differences in CRN were not observed in the lowest income group but were seen among the low-, middle-, and high-income groups, although for several comparisons, statistical significance was not reached. Finally, we found that CRN was associated with greater emergency department utilization, but not hospital utilization.
Prior literature has documented that HDHP enrollment is associated with decreased5,16,23 or delayed27 utilization of several forms of care in people with diabetes, but that being switched to a HDHP (with a health savings account) which covers medications such as insulin before deductibles are met, decreases out-of-pocket costs.32 However, little has been known about the association of HDHP enrollment and CRN to medications among patients with diabetes.1,2,4,7,17,33 Two prior studies have demonstrated that a switch to a HDHP was associated with a modest decline in hypoglycemic medication use,34,35 but both were conducted in a single health plan or employer over a decade ago, prior to the recent rapid rises in cost of hypoglycemic medications. Our study is the only one we are aware of that examines the association of HDHP enrollment with CRN among diabetic patients in a contemporary, nationally representative sample. It also documents that the increased rate of CRN among HDHP compared with TCP enrollees is sizeable — 28% greater among all diabetic patients and 31% greater among insulin users.
High-deductible health plans, by design, expose patients to high out-of-pocket costs for care.9,13,24,25 Until the insurance plan deductible is reached in any given year, some may be unable to afford these out-of-pocket costs and may instead skip medication doses, take less medication than prescribed, or delay filling a prescription.14 We were not able to directly study the impact of medication prices; however, it seems likely that cost increases of newer oral hypoglycemic agents and insulin,18 as well as the concurrent general rise in out-of-pocket expenditures for these medications,21,36 particularly in HDHPs tied to health savings accounts,37 also play a role in the CRN we observed. Our finding that HDHP-related CRN was generally greater among insulin users is consistent with these patients’ higher costs for medications and other care. This is particularly concerning given the potential clinical consequences of non-adherence to insulin compared with oral agents, such as diabetic ketoacidosis.
Our finding that income level dramatically affects CRN rates among both HDHP enrollees and TCP enrollees, and that a full third of patients in the lowest-income group report CRN, underscores the substantial financial barriers currently faced by commercially insured patients with diabetes. Differences in CRN between HDHP enrollees and TCP enrollees were observed in income groups above the lowest income category. These findings show that exposure to high out-of-pocket costs of medical care may adversely affect those with middle or even relatively high incomes.
Among patients with diabetes, medication non-adherence (from any cause) has been associated with a range of adverse outcomes, including an increase in hospitalizations,5,6,7 and CRN has been associated with worse glycemic control and physical functioning in studies conducted within single health insurers or managed care organizations. In our national sample of patients with diabetes, we found that experiencing any CRN was associated with an elevated risk of having an emergency department visit; this adds additional support for the use of CRN as a clinically relevant outcome among people with diabetes. In contrast to prior studies, we found no increase in rates of hospitalization associated with HDHP enrollment in adjusted analyses, although the reasons for this are not clear.
Our study has several limitations. First, the NHIS deductible variable is binary — high vs low or no deductible — and the actual numerical values were unknown. Consequently, we were unable to assess how actual differences in deductible levels in the two plan types are related to CRN. Second, we do not know the duration of insurance coverage of respondents at the time of the survey interview; therefore, some respondents with newly acquired insurance could have answered CRN questions referring to a time when they did not have their current coverage. Third, we did not have information about the time course or severity of the diabetes diagnosis, both of which could affect perceptions about the urgency of adherence to diabetes medications and, if this differed by HDHP status, may have affected our results. Fourth, our outcomes were self-reported and are therefore subject to potential recall error, although it seems unlikely that there would be a differential effect by HDHP status. Fifth, our CRN questions were not specific to diabetes medications. However, in our sensitivity analysis, we obtained very similar results when patients with other chronic conditions were excluded, suggesting that the CRN we observed related to medications for diabetes. Sixth, this was an observational study; thus, we cannot definitively establish that the associations we observed were causal. We were able to control for a wide range of potential demographic and clinical confounders but residual confounding by unobserved factors remains a possibility.
Our findings have several implications. First, clinicians should be cognizant that inadequacies in insurance coverage could lead to CRN among their patients with diabetes, particularly among insulin users and those with low incomes. Second, to improve CRN, policy makers should enact reforms to control rapidly escalating prices of diabetes medications, particularly insulin. Potential tools include patent reform, ensuring timely generic drug availability, expanding opportunities for government entities to negotiate prices with pharmaceutical companies,38 and expanding a recent IRS rule allowing HDHPs with a health savings account to cover medications such as insulin before deductibles are met39 to other types of HDHPs. Finally, the public should be aware that policies that expand the use of HDHPs could harm patients with diabetes, while policies that reduce financial barriers to care could improve access and adherence to needed medications for patients with this condition.
References
Pladevall M, Williams LK, Potts LA, Divine G, Xi H, Lafata JE. Clinical outcomes and adherence to medications measured by claims data in patients with diabetes. Diabetes Care. 2004;27(12):2800-5.
Egede LE, Gebregziabher M, Echols C, Lynch CP. Longitudinal effects of medication nonadherence on glycemic control. Ann Pharmacother. 2014;48(5):562-70.
Garcia-Perez LE, Alvarez M, Dilla T, Gil-Guillen V, Orozco-Beltran D. Adherence to therapies in patients with type 2 diabetes. Diabetes Ther. 2013;4(2):175-94.
Aikens JE, Piette JD. Longitudinal association between medication adherence and glycaemic control in type 2 diabetes. Diabet Med. 2013;30(3):338-44.
Ho PM, Rumsfeld JS, Masoudi FA, McClure DL, Plomondon ME, Steiner JF, et al. Effect of medication nonadherence on hospitalization and mortality among patients with diabetes mellitus. Arch Intern Med. 2006;166(17):1836-41.
Sokol MC, McGuigan KA, Verbrugge RR, Epstein RS. Impact of medication adherence on hospitalization risk and healthcare cost. Med Care. 2005;43(6):521-30.
Lau DT, Nau DP. Oral antihyperglycemic medication nonadherence and subsequent hospitalization among individuals with type 2 diabetes. Diabetes Care. 2004;27(9):2149-53.
American Diabetes A. Standards of medical care in diabetes--2013. Diabetes Care. 2013;36 Suppl 1:S11-66.
Goldman DP, Joyce GF, Zheng Y. Prescription drug cost sharing: associations with medication and medical utilization and spending and health. JAMA. 2007;298(1):61-9.
Briesacher BA, Gurwitz JH, Soumerai SB. Patients at-risk for cost-related medication nonadherence: a review of the literature. J Gen Intern Med. 2007;22(6):864-71.
Kesselheim AS, Huybrechts KF, Choudhry NK, Fulchino LA, Isaman DL, Kowal MK, et al. Prescription drug insurance coverage and patient health outcomes: a systematic review. Am J Public Health. 2015;105(2):e17-30.
Zhang JX, Meltzer DO. The high cost-related medication non-adherence rate among medicare-medicaid dual-eligible diabetes patients. J Health Med Econ. 2016;2(2).
Karter AJ, Parker MM, Solomon MD, Lyles CR, Adams AS, Moffet HH, et al. Effect of out-of-pocket cost on medication initiation, adherence, and persistence among patients with type 2 diabetes: the Diabetes Study of Northern California (DISTANCE). Health Serv Res. 2018;53(2):1227-47.
Herkert D, Vijayakumar P, Luo J, Schwartz JI, Rabin TL, DeFilippo E, et al. Cost-related insulin underuse among patients with diabetes. JAMA Intern Med. 2018.
Kang H, Lobo JM, Kim S, Sohn MW. Cost-related medication non-adherence among U.S. adults with diabetes. Diabetes Res Clin Pract. 2018;143:24-33.
Rabin DL, Jetty A, Petterson S, Saqr Z, Froehlich A. Among low-income respondents with diabetes, high-deductible versus no-deductible insurance sharply reduces medical service use. Diabetes Care. 2017;40(2):239-45.
Schectman JM, Nadkarni MM, Voss JD. The association between diabetes metabolic control and drug adherence in an indigent population. Diabetes Care. 2002;25(6):1015-21.
Hua X, Carvalho N, Tew M, Huang ES, Herman WH, Clarke P. Expenditures and prices of antihyperglycemic medications in the United States: 2002-2013. JAMA. 2016;315(13):1400-2.
Tribble SJ. Flurry of federal and state probes target insulin drugmakers and pharma middlemen. https://khn.org/news/flurry-of-federal-and-state-probes-target-insulin-drugmakers-and-pharma-middlemen/. Accessed June 25, 2020.
Luo J, Avorn J, Kesselheim AS. Trends in Medicaid reimbursements for insulin from 1991 through 2014. JAMA Intern Med. 2015;175(10):1681-6.
Lipska KJ, Ross JS, Van Houten HK, Beran D, Yudkin JS, Shah ND. Use and out-of-pocket costs of insulin for type 2 diabetes mellitus from 2000 through 2010. JAMA. 2014;311(22):2331-3.
Claxton G, Rae M, Long M, Damico A, Whitmore H. The Kaiser Family Foundation Employer Health Benefits 2018 Annual Survey. October 3, 2018. Accessed at: https://www.kff.org/report-section/2018-employer-health-benefits-survey-section-1-cost-of-health-insurance/.
Wharam JF, Zhang F, Eggleston EM, Lu CY, Soumerai S, Ross-Degnan D. Diabetes outpatient care and acute complications before and after high-deductible insurance enrollment: a Natural Experiment for Translation in Diabetes (NEXT-D) Study. JAMA Intern Med. 2017;177(3):358-68.
Abdus S, Keenan PS. Financial burden of employer-sponsored high-deductible health plans for low-income adults with chronic health conditions. JAMA Intern Med. 2018;178(12):1706-8.
Segel JE, Kullgren JT. Health insurance deductibles and their associations with out-of-pocket spending and affordability barriers among US adults with chronic conditions. JAMA Intern Med. 2017;177(3):433-6.
Chua KP, Lee JM, Conti RM. Out-of-pocket spending for insulin, diabetes-related supplies, and other health care services among privately insured US patients with type 1 diabetes. JAMA Intern Med. 2020.
Wharam JF, Lu CY, Zhang F, Callahan M, Xu X, Wallace J, et al. High-deductible insurance and delay in care for the macrovascular complications of diabetes. Ann Intern Med. 2018;169(12):845-54.
Gaffney A, White A, Hawks L, Himmelstein D, Woolhandler S, Christiani DC, et al. High-deductible health plans and healthcare access, use, and financial strain in those with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2020;17(1):49-56.
Lewey J, Gagne JJ, Franklin J, Lauffenburger JC, Brill G, Choudhry NK. Impact of high deductible health plans on cardiovascular medication adherence and health disparities. Circ Cardiovasc Qual Outcomes. 2018;11(11):e004632.
Center for Disease Control and Prevention. National Center for Health Statistics National Health Interview Survey. About the National Health Interview Survey. Accessed at: https://www.cdc.gov/nchs/nhis/about_nhis.htm.
Piette JD, Wagner TH, Potter MB, Schillinger D. Health insurance status, cost-related medication underuse, and outcomes among diabetes patients in three systems of care. Med Care. 2004;42(2):102-9.
Ross-Degnan D, Wallace J, Zhang F, Soumerai SB, Garabedian L, Wharam JF. Reduced cost-sharing for preventive drugs preferentially benefits low-income patients with diabetes in high deductible health plans with health savings accounts. Med Care. 2020;58 Suppl 6 Suppl 1:S4-S13.
Rogers MAM, Lee JM, Tipirneni R, Banerjee T, Kim C. Interruptions In private health insurance and outcomes in adults with type 1 diabetes: a longitudinal study. Health Aff (Millwood). 2018;37(7):1024-32.
Reiss SK, Ross-Degnan D, Zhang F, Soumerai SB, Zaslavsky AM, Wharam JF. Effect of switching to a high-deductible health plan on use of chronic medications. Health Serv Res. 2011;46(5):1382-401.
Nair K, Park J, Wolfe P, Saseen J, Read Allen R, Ganguly R.. Consumer- driven health plans: impact on utilization and expenditures for chronic disease sufferers. J Occup Environ Med. 2009;51: 594–602.
Li R, Barker LE, Shrestha S, Zhang P, Duru OK, Pearson-Clarke T, et al. Changes over time in high out-of-pocket health care burden in U.S. adults with diabetes, 2001-2011. Diabetes Care. 2014;37(6):1629-35.
Meiri A, Zhang F, Ross-Degnan D, Wharam JF. Trends in insulin out-of-pocket costs and reimbursement price among us patients with private health insurance, 2006-2017. JAMA Intern Med. 2020.
Kesselheim AS, Avorn J, Sarpatwari A. The high cost of prescription drugs in the United States: origins and prospects for reform. JAMA. 2016;316(8):858-71.
Internal Revenue Service IRS expands list of preventive care for HSA participants to include certain care for chronic conditions. Published July 17, 2019. https://www.irs.gov/newsroom/irs-expands-list-of-preventive-care-for-hsa-participants-to-include-certain-care-for-chronic-conditions. Accessed January 7, 2020.
Author information
Authors and Affiliations
Contributions
There were no contributors that did not meet authorship criteria.
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 43.5 kb)
Rights and permissions
About this article

Cite this article
Rastas, C., Bunker, D., Gampa, V. et al. Association Between High Deductible Health Plans and Cost-Related Non-adherence to Medications Among Americans with Diabetes: an Observational Study. J GEN INTERN MED 37, 1910–1916 (2022). https://doi.org/10.1007/s11606-021-06937-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-021-06937-9