
Abstract
The mainstay of treatment for acute decompensated heart failure (ADHF) is intravenous (IV) diuretic therapy either as a bolus or via continuous infusion. Despite being available for decades, few randomized trials exist to guide dosing and administration of these drugs. In 2011, the Diuretic Optimization Strategies Evaluation (DOSE) trial used a prospective, randomized design to compare bolus versus continuous infusion of IV furosemide, as well as high-dose versus low-dose therapy. The study found no difference in the primary end point for continuous versus bolus infusion. High-dose diuretics were more effective than low dose without clinically important negative effects on renal function. Although limited by patient selection criteria and protocol design, the study challenges long-held beliefs that continuous infusion is more effective than bolus dosing. The study also challenges the notion that high-dose diuretics carry clinically important renal toxicity risks for patients.
Similar content being viewed by others

References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Jessup M, Abraham WT, Casey DE, et al. 2009 Focused Update Incorporated Into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: Developed in Collaboration With the International Society for Heart and Lung Transplantation. Circulation. 2009;119:e391–479.
Brest AN, Seller R, Onesti G, et al. Clinical selection of diuretic drugs in management of cardiac edema. Am J Card. 2004;22:168–76.
Lindenfeld J, Albert NM, Boehmer JP, et al. Executive summary: HFSA 2010 comprehensive heart failure practice guideline. J Card Fail. 2010;6:475–528.
Emerman CL, Marco TD, Constanzo MR, et al. Impact of intravenous diuretics on the outcomes of patients hospitalized with acute decompensated heart failure: insights from the ADHERE(R) Registry. J Card Fail. 2004;10:S116–7.
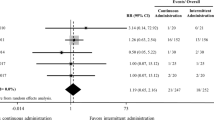
Felker GM, Lee KL, Bull DA, et al. Diuretic strategies in patients with acute decompensated heart failure. N Engl J Med. 2011;364(9):797–805.
Sica DA. Edema mechanisms in the patient with heart failure and treatment options. Heart Failure Clinics. 2008;4:511–8.
Schrier RW, Abraham WT. Hormones and hemodynamics in heart failure. N Engl J Med. 1999;341:577–85.
• Kemp CD, Conte JV. The pathophysiology of heart failure. Cardiovasc Pathol. 2012 Jan 5. This is a comprehensive review of the pathophysiology of heart failure with focus on the neuroendocrine system, pressure-volume relationships, and ventricular remodeling.
Franics GS, Siegel RM, Goldsmith SR, et al. Acute vasoconstrictor response to intravenous furosemide in patients with chronic congestive heart failure. Ann Int Med. 1985;103:1–6.
Francis GS, Benedict C, Johnstone DE, Kirlin PC, et al. Comparison of neuroendocrine activation in patients with left-ventricular dysfunction with and without congestive heart failure—a substudy of the studies of left-ventricular dysfunction (SOLVD). Circulation. 1990;82:1724–9.
Bayliss J, Norell M, Canepaanson R, Sutton G, et al. Untreated heart failure—clinical and neuroendocrine effects of introducing diuretics. Br Heart J. 1987;57:17–22.
McCurley JM, Hanlon SU, Wei SK, et al. Furosemide and the progression of left ventricular dysfunction in experimental heart failure. J Am Coll Cardiol. 2004;44:1301–7.
Packer M, Cohn JN. Consensus recommendations for the management of chronic heart failure. On behalf of the membership advisory council to improve outcomes nationwide in heart failure. Am J Cardiol. 1999;83:1A–38A.
The SOLVD Investigators. Effects of enalapril on survival in patients with reduced left ventricular ejection fraction and congestive heart failure. N Engl J Med. 1991;325:293–302.
The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med. 1987;316:1429–35.
Godwin TF, Gunton RW. Clinical trial of a new diuretic, furosemide: comparison with hydrochlorothiazide and mercaptomerin. Canadian Medical Association Journal. 1965;93(25):1296–300.
Dube P, Weber KT. Congestive heart failure: pathophysiologic consequences of neurohormonal activation and the potential for recovery: part 1. Am J Med Sci. 2011;342(5):348–51.
Leary WP, Reyes AJ. Diuretic-induced magnesium losses. Drugs. 1984;29 suppl 1:182–7.
• Jentzer JC, DeWald TA, Hernandez AF. Combination of loop diuretics with Thiazide-type diuretics in Heart Failure. J Am Coll Cardiol. 2010;56:1527–34. This state-of-the-art paper reviews the current data regarding combination diuretic therapy in refractory or diuretic-resistant heart failure, highlighting the need for large-scale clinical trials to develop safe and effective treatment strategies for advanced heart failure. The paper reviews the physiology and pathophysiology of diuretics in heart failure.
Rosenberg J, Gustafsson F, Galatius S, et al. Combination therapy with metolazone and loop diuretics in outpatients with refractory heart failure: an observational study and review of the literature. Cardiovasc Drugs Ther. 2005;19:301–6.
Klein L, O’Conner CM, Leimberger JD, et al. Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the outcomes of a prospective trial of intravenous milrinone for exacerbations of chronic heart failure (OPTIMIZE-HF) study. Circulation. 2005;111:2454–60.
Cooper HA, Dries DL, Davis CE, Shen YL, Domanski MJ. Diuretics and risk of arrhythmic death in patients with left ventricular dysfunction. Circulation. 1999;100:1311–5.
Sica DA, Gehr TW. Diuretic combinations in refractory edema states: pharmacokinetics/pharmacodynamic relationships. Clin Pharmacokinet. 1996;30:229–49.
Shankar SS, Brater DC. Loop diuretics: from the Na-K-2Cl transporter to clinical use. Am J Physiol Renal Physio. 2003;284:F11–21.
Gottlieb SS, Brater DC, Thomas I, Havranek E, Bourge R, et al. BG9719 (CVT-124), an A(1) adenosine receptor antagonist, protects against decline in renal function observed with diuretic therapy. Circulation. 2002;105:1348–53.
Liguori A, Casini A, Di Loreto M, et al. Loop diuretics enhance the secretion of prostacyclin in vitro, in healthy persons and in patients with chronic heart failure. Eur J Clin Pharmacol. 1999;55:117–24.
Sjostrom PA, Kron BG, Odlind BG. Changes in renal clearance of furosemide due to changes in renal blood flow and plasma albumin concentration. Eur J Clin Pharmacol. 1993;45:135–9.
Butler J, Forman DE, Abraham WT, et al. Relationship between heart failure treatment and developing worsening renal function among hospitalized patients. Am Heart J. 2004;147:331–8.
Hasselblad V, Stough WG, Shah MR, et al. Relation between dose of loop diuretics and outcomes in a heart failure population: results of the ESCAPR trial. Eur J Heart Fail. 2007;9:1064–9.
Eshaghian S, Horwich TB, Fonarow GC. Relation of loop diuretic dose to mortality in advanced heart failure. Am J Cardiol. 2006;97:1759–64.
Philbin EF, Cotto M, Rocco Jr TA, Jenkins PL. Association between diuretic use, clinical response and death in acute heart failure. Am J Cardiol. 1997;80:519–22.
Mielniczuk LM, Tsang SW, Desai AS, et al. The association between high-dose diuretics and clinical stability in ambulatory chronic heart failure patients. J Card Fail. 2008;14:388–93.
Wilcox CS, Mitch WE, Kelly RA, et al. Response of the kidney to furosemide. I. Effects of salt intake and renal compensation. J Lab Clin Med. 1983;102:450–8.
Kaissling B, Bachman S, Kriz W. Structural adaptation of the distal convoluted tubule to prolonged furosemide treatment. Am J Physiol. 1985;248:F374–381.
Dormans TPJ, van Meyel JJM, Gerlag PGG, et al. Diuretic efficacy of high dose furosemide in severe heart failure: bolus injection versus continuous infusion. Journal of the American College of Cardiology. 1996;28:376–82.
Licata G, Di Pasquale P, Parrinello G, et al. Effects of high doses of furosemide and small volume hypertonic saline solution infusion in comparison with high dose of furosemide as a bolus in refractory congestive heart failure. American heart Journal. 2003;145:459–66.
Salvador DR, Rey NR, Ramos GC, Punzalan FE. Continuous Infusion versus bolus injection of loop diuretics in congestive heart failure. Cochrane Database Syst Rev. 2005 Jul 20;(3): CD003178.
Aaser E, Gullestad L, Tollofsrud S, Lundberg J, et al. Effect of bolus injection versus continuous infusion of furosemide on diuresis and neruohormonal activation in patients with severe congestive heart failure. Scandinavian Journal of Clinical and Laboratory Investigation. 1997;57:361–8.
Krammer WG, Smith WB, Ferguson J, et al. Pharmacodynamics of torsemide administered as an intravenous injection and as a continuous infusion to patients with congestive heart failure. Journal of Clinical Pharmacology. 1996;36:265–70.
• Allen LA, Turer AT, DeWald T et al. Continuous versus Bolus Dosing of Furosemide for Patients Hospitalized for Heart Failure. Am J Cardiol 2010;105:1794-1797. This paper presents the data from a prospective, open-label, single-center, randomized trial evaluating bolus injection versus continuous infusion of furosemide in acute decompensated heart failure. The study enrolled 41 patients with a mean EF of 35 %. The authors found no difference in regards to change in serum creatinine, urine output, electrolyte abnormalities, or length of stay between the two treatment strategies. The authors concluded that continuous infusion and bolus dosing of furosemide were of equal effectiveness and safety in acute decompensated heart failure.
• Thompson MR, Nappi JM, Dunn SP et al. Continuous versus Intermittent Infusion of Furosemide in Acute Decompensated Heart Failure. J Cardiac Fail. 2010;16:188-193. This small (56 patient), prospective, randomized parallel study evaluated the effectiveness of continuous and intermittent infusion of intravenous diuretics. Patients receiving continuous infusion furosemide experienced significantly greater diuresis compared to intermittent infusion (3726 ± 1121 mL/24 h vs 2955 ± 1267 mL/24 h, respectively [P = 0.019]). The authors concluded that continuous infusion was safe and more effective than intermittent infusion.
Disclosures
PT Campbell: none. Dr. Jason Ryan has served as a consultant for iCare nursing homes.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Campbell, P.T., Ryan, J. Diuretic Dosing in Acute Decompensated Heart Failure: Lessons from DOSE. Curr Heart Fail Rep 9, 260–265 (2012). https://doi.org/10.1007/s11897-012-0094-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11897-012-0094-8