
Abstract
Background
Kinematically aligned TKA restores function by aligning the femoral and tibial components to the normal or prearthritic joint lines of the knee. However, aligning the components to the joint lines of the normal knee also aligns the tibial component in varus, creating concern that varus alignment might result in poor function and early catastrophic failure.
Questions/Purposes
We therefore determined whether function and the incidence of catastrophic failure were different when the tibial component, knee, and limb alignment were in a specified normal range, varus outlier, or valgus outlier.
Methods
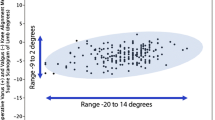
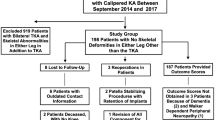
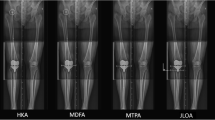
We prospectively followed all 198 patients (214 knees) who underwent TKAs between February and October 2008. We treated each knee in this cohort of patients with a kinematically aligned, cruciate-retaining prosthesis implanted using patient-specific guides. From a long-leg scanogram, we measured and categorized alignment of the tibial component as in range (≤ 0°) or a varus outlier (> 0°), alignment of the knee as in range (between −2.5° to −7.4° valgus) or a varus (> −2.5°) or valgus (< −7.4°) outlier, and alignment of the limb as in range (0° ± 3°) or a varus (> 3°) or valgus (< −3°) outlier. We assessed function using the Oxford Knee Score and WOMAC™ score, and reported catastrophic failure as the incidence of revision attributable to loosening, wear, and instability of the femoral or tibial components. The minimum followup was 31 months (mean, 38 months; range, 31–43 months).
Results
The mean Oxford Knee Score of 43 and WOMAC™ score of 92 were similar between the three alignment categories. The incidence of catastrophic failure in each alignment category was zero.
Conclusions
Kinematically aligned TKA restores function without catastrophic failure regardless of the alignment category. Because 75% of patients had their tibial component categorized as a varus outlier and also had high function and a zero incidence of catastrophic failure, the concern that kinematic alignment compromises function and places the components at a high risk for catastrophic failure is unfounded and should be of interest to surgeons committed to cutting the tibia perpendicular to the mechanical axis of the tibia.
Level of Evidence
Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.



Similar content being viewed by others
References
Baker PN, van der Meulen JH, Lewsey J, Gregg PJ. The role of pain and function in determining patient satisfaction after total knee replacement: data from the National Joint Registry for England and Wales. J Bone Joint Surg Br. 2007;89:893–900.
Bellemans J, Colyn W, Vandenneucker H, Victor J. The Chitranjan Ranawat Award: Is neutral mechanical alignment normal for all patients? The concept of constitutional varus. Clin Orthop Relat Res. 2012;470:45–53.
Bonner TJ, Eardley WG, Patterson P, Gregg PJ. The effect of post-operative mechanical axis alignment on the survival of primary total knee replacements after a follow-up of 15 years. J Bone Joint Surg Br. 2011;93:1217–1222.
Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010;468:57–63.
Dossett HG, Swartz GJ, Estrada NA, Lefevre GW, Kwasman BG. Kinematically versus mechanically aligned total knee arthroplasty. Orthopedics. 2012;35:e160–169.
Eckhoff D, Hogan C, DiMatteo L, Robinson M, Bach J. Difference between the epicondylar and cylindrical axis of the knee. Clin Orthop Relat Res. 2007;461:238–244.
Eckhoff DG, Bach JM, Spitzer VM, Reinig KD, Bagur MM, Baldini TH, Flannery NM. Three-dimensional mechanics, kinematics, and morphology of the knee viewed in virtual reality. J Bone Joint Surg Am. 2005;87(suppl 2):71–80.
Graves S. Australian Orthopaedic Association National Joint Replacement Registry Annual Report 2010. Australian Orthopaedic Association. Available at: http://www.dmac.adelaide.edu.au/aoanjrr/publications.jsp?section=reports2010. Accessed January 2, 2012.
Hollister AM, Jatana S, Singh AK, Sullivan WW, Lupichuk AG. The axes of rotation of the knee. Clin Orthop Relat Res. 1993;290:259–268.
Howell SM, Howell SJ, Hull ML. Assessment of the radii of the medial and lateral femoral condyles in varus and valgus knees with osteoarthritis. J Bone Joint Surg Am. 2010;92:98–104.
Howell SM, Hull ML. Kinematic alignment in TKA: definition, surgical technique, and challenging cases. Orthopedic Knowledge Online. 2012;10, Number 7.
Howell SM, Hull ML. Kinematically aligned TKA with MRI-based cutting guides. In: Thienpont E, ed. Improving Accuracy in Knee Arthroplasty. New Delhi, India: Jaypee Brothers Medical Publishers (P) Ltd; 2012:207–232.
Howell SM, Hull ML. Kinematic alignment in total knee arthroplasty. In: Scott WN, ed. Insall and Scott Surgery of the Knee. Philadelphia, PA: Elsevier; 2012:1255–1268.
Howell SM, Kuznik K, Hull ML, Siston RA. Results of an initial experience with custom-fit positioning total knee arthroplasty in a series of 48 patients. Orthopedics. 2008;31:857–863.
Howell SM, Kuznik K, Hull ML, Siston RA. Longitudinal shapes of the tibia and femur are unrelated and variable. Clin Orthop Relat Res. 2010;468:1142–1148.
Howell SM, Rogers SL. Method for quantifying patient expectations and early recovery after total knee arthroplasty. Orthopedics. 2009;32:884–890.
Kamat YD, Aurakzai KM, Adhikari AR, Matthews D, Kalairajah Y, Field RE. Does computer navigation in total knee arthroplasty improve patient outcome at midterm follow-up? Int Orthop. 2009;33:1567–1570.
Klatt BA, Goyal N, Austin MS, Hozack WJ. Custom-Fit total knee arthroplasty (OtisKnee) results in malalignment. J Arthroplasty. 2008;23:26–29.
Labek G, Neumann D, Agreiter M, Schuh R, Böhler N. Impact of implant developers on published outcome and reproducibility of cohort-based clinical studies in arthroplasty. J Bone Joint Surg Am. 2011;93(suppl 3):55–61.
Malkani AL, Rand JA, Bryan RS, Wallrichs SL. Total knee arthroplasty with the kinematic condylar prosthesis: a ten-year follow-up study. J Bone Joint Surg Am. 1995;77:423–431.
Noble PC, Conditt MA, Cook KF, Mathis KB. The John Insall Award: Patient expectations affect satisfaction with total knee arthroplasty. Clin Orthop Relat Res. 2006;452:35–43.
Nunley RM, Ellison BS, Zhu J, Ruh EL, Howell SM, Barrack RL. Do patient-specific guides improve coronal alignment in total knee arthroplasty? Clin Orthop Relat Res. 2012;470:895–902.
Pandit H, Jenkins C, Gill HS, Barker K, Dodd CA, Murray DW. Minimally invasive Oxford phase 3 unicompartmental knee replacement: results of 1000 cases. J Bone Joint Surg Br. 2011;93:198–204.
Parratte S, Pagnano MW, Trousdale RT, Berry DJ. Effect of postoperative mechanical axis alignment on the fifteen-year survival of modern, cemented total knee replacements. J Bone Joint Surg Am. 2010;92:2143–2149.
Ritter MA, Davis KE, Meding JB, Pierson JL, Berend ME, Malinzak RA. The effect of alignment and BMI on failure of total knee replacement. J Bone Joint Surg Am. 2011;93:1588–1596.
Rothwell AG, Hooper GJ, Hobbs A, Frampton CM. An analysis of the Oxford hip and knee scores and their relationship to early joint revision in the New Zealand Joint Registry. J Bone Joint Surg Br. 2010;92:413–418.
Acknowledgments
We thank the imaging department and technicians at Methodist Hospital for performing the CT scanograms.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors certifies that he (KTK) is an employee of Stryker Orthopedics (Mahwah, NJ, USA). One author (SMH) is a consultant for Stryker Orthopedics (Mahwah, NJ, USA). All other authors certify that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA-approval status, of any drug or device prior to clinical use.
Each author certifies that his or her institution has approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
This work was performed at Methodist Hospital, Sacramento, CA, USA, and at the Department of Mechanical Engineering, University of California at Davis, Davis, CA, USA.
About this article
Cite this article
Howell, S.M., Howell, S.J., Kuznik, K.T. et al. Does A Kinematically Aligned Total Knee Arthroplasty Restore Function Without Failure Regardless of Alignment Category?. Clin Orthop Relat Res 471, 1000–1007 (2013). https://doi.org/10.1007/s11999-012-2613-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2613-z