
Abstract
Airway management is central to the resuscitation of the neurologically ill. These patients often have evolving processes that threaten the airway and adequate ventilation. Therefore, airway, ventilation, and sedation were chosen as an Emergency Neurological Life Support (ENLS) protocol. Reviewed topics include airway management; the decision to intubate; when and how to intubate with attention to cardiovascular status; mechanical ventilation settings; and the use of sedation, including how to select sedative agents based on the patient’s neurological status.
Similar content being viewed by others

Introduction
Intubation of the acutely brain-injured patient is a matter of life or death. Failure to intubate a patient with rapidly progressive neurological decline may result in respiratory arrest, secondary brain injury from hypoxia or hypercarbia, and severe aspiration pneumonitis or acute respiratory distress syndrome.
The process of induction and intubation can itself provoke brain herniation when a mass lesion is present, complete a massive infarction when brain tissue is marginally perfused by collateral cerebrovascular circulation, or result in temporary obliteration of the neurological examination during the early—and often most critical—period of neurological and neurosurgical decision-making.
Rapid patient stabilization must occur concurrently with well-documented and detailed neurological assessment. The goals of airway management in neurological patients are therefore to maintain adequate (but not excessive) oxygenation and ventilation, and to prevent aspiration. Ideally, a neurological assessment prior to the administration of sedating and paralyzing medications is recommended in order to provide a functional baseline.
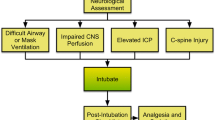
The Emergency Neurological Life Support (ENLS) suggested algorithm for the initial management of airway, ventilation, and sedation is shown in Fig. 1. Suggested items to complete within the first hour of evaluating a patient are shown in Table 1.

ENLS airway, ventilation, and sedation protocol
Need Intubation?
Patients with respiratory arrest or impending arrest should be intubated without delay. In addition, a patient who cannot “protect his airway” because of depressed mental status or vomiting with aspiration may need tracheal intubation. Intubation has the potential for morbidity, creates significant hemodynamic disturbances, and should not be undertaken without a risk-benefit assessment. However, it should not be delayed when emergent intubation is necessary. The decision to intubate involves factors specific to patient physiology and to the clinical environment and anticipated course of care.
In the prehospital or emergency department (ED) environment, an obtunded patient with unknown pathophysiology requiring interhospital/interdepartmental transfer or imaging/invasive procedures may be most safely managed by urgent intubation. The same patient with a known physiology, an anticipated stable or improving course, and no planned transportation may not require intubation, or may even be an appropriate candidate for extubation.
With these considerations in mind, there are four commonly accepted indications to intubate:
-
1.
Failure to oxygenate: May be driven by pulse oximetry (limitations include regional or systemic hypoperfusion, severe anemia, and opaque nail polish), arterial blood gas analysis, or the patient’s visual appearance (cyanosis).
-
2.
Failure to ventilate: May be driven by capnometry through nasal cannula monitoring (does not always correlate with pCO2, but provides a valuable tool for monitoring trends in ventilation) [1], by arterial blood gas analysis, or by gross visual appearance (excessive or inadequate work of breathing).
-
3.
Failure to protect the airway: Driven by the risk of aspiration and its complications. This is a balance between bulbar function, quantity and quality of secretions, strength of cough reflex, and ability to swallow after suctioning [2]. The gag reflex is an inaccurate method of assessing airway protection [3].
-
4.
Anticipated neurological or cardiopulmonary decline requiring transport or immediate treatment.
Airway Assessment
Assessment of the airway includes ease of bag-mask ventilation and the potential for a difficult intubation. This assessment enables strategic planning and efficient resource utilization. The “LEMON” mnemonic helps to predict the difficult airway [3]:
-
L = Look
-
E = Evaluate the mouth opening and airway position
-
M = Mallampati score
-
O = Obstruction
-
N = Neck mobility
The “MOANS” mnemonic predicts ease of bag-mask ventilation [3]:
-
M = Mask seal
-
O = Obesity/obstruction
-
A = Age >55
-
N = No teeth
-
S = Stiff lungs
Patients anticipated to be difficult in either regard should prompt the clinician to prepare with appropriate back-up in terms of skilled individuals (e.g., call for anesthesia assistance) and devices (e.g., fiberoptic and other adjunct intubating devices, and set-up for a cricothyrotomy). Assessment of the expected ease of bag-mask ventilation is critical; if deemed difficult, access to an extra-glottic ventilation device, such as a laryngeal mask airway (LMA), may be warranted.
Decision Made to Intubate: Perform Neurological Assessment
Whenever possible, urgent management of the airway should coincide with a rapid but detailed neurological assessment. The examination can typically be conducted in 1–2 min and is crucial to subsequent emergency decision making.
The pre-sedation/pre-intubation neurologic exam establishes a baseline that is used to assess therapeutic interventions (e.g., patients with stroke or non-convulsive status epilepticus) or may identify injuries that are at risk of progressing (e.g., unstable cervical spine fractures). The assessment identifies the type of testing and helps to avoid unnecessary, uncomfortable interventions, such as cervical spine immobilization with its potential for discomfort and skin care complications. In general, the pre-intubation neurological assessment is the responsibility of the team leader who is coordinating the resuscitation; findings should be documented and communicated directly to the team that assumes care of the patient.
As demonstrated in Table 5, pre-intubation neurological examination includes an assessment of:
-
Level of arousal, interaction, and orientation
-
Cranial nerves
-
Motor function of each individual extremity
-
Tone & reflexes
-
Subtle or gross seizure activity
-
Cervical spine stability
-
When spinal cord injury is suspected, assess sensory level
Intubating the Patient
Rapid sequence intubation is the preferred method of securing the airway in patients with suspected elevated intracranial pressure (ICP), since it provides protection against the reflex responses to laryngoscopy and rises in ICP [4–7]. The presence of coma should not be interpreted as an indication to proceed without pharmacological agents, or to administer only a neuromuscular blocking agent without appropriate pre-treatment and induction agents. Although the patient may seem unresponsive, laryngoscopy and intubation usually provoke reflexes that elevate ICP unless appropriate pre-treatment and induction agents are used [8].
Outcomes in patients with intracranial catastrophes are related to the maintenance of both brain perfusion and oxygenation; consequently, close assessment and management of these two parameters are critical. Cerebral perfusion pressure (CPP) is the physiologic correlate for blood flow to the brain and is measured by the difference between the mean arterial pressure (MAP) and the ICP:
It is generally recommended that the ICP be maintained below 20 mmHg, MAP between 80 and 110 mmHg, and CPP at a minimum of 60 mmHg.
Clinicians must recognize that many neurologically impaired patients have compromised cerebral blood flow (CBF) even with a normal ICP. For example, patients with ischemic stroke, vasospasm, and hypoxic-ischemic brain injury often have impaired auto regulation and are each critically sensitive to decreases in blood pressure and CBF. In these patients, the goal is to maintain MAP and CPP as for the patients with known or suspected elevation of ICP.
Problems associated with elevated ICP may be compounded by the techniques and drugs used in airway management, since they may further elevate ICP. In addition, victims of multiple trauma may present with hypotension, thus limiting the choice of agents and techniques available.
Intubating the Patient with Presumed Elevated Intracranial Pressure (ICP)
In the prehospital and ED environment, clinical evidence of increased ICP is inferred from clinical signs of brain herniation that include altered mental status plus a unilaterally dilated pupil, bilaterally dilated and fixed pupils, and decerebrate or extensor posturing (decorticate posturing is not predictive of elevated ICP) [9]. Since ICP measurement is usually not available in these situations, one should proceed with the assumption that ICP is elevated, assuming a value of at least 20 mmHg for ICP in these circumstances. When the airway is manipulated, two responses may result in even more increased ICP: the reflex sympathetic response (RSR), which results in increased heart rate, increased blood pressure, and, consequently, increased ICP; and the direct laryngeal reflex that stimulates an increase in ICP independent of the RSR [3].
Although the RSR may be dangerous in a hypertensive patient, pre-treatment of the RSR is not indicated in a hypotensive patient with known or suspected increased ICP [10]. Elevations in ICP should be mitigated by minimizing airway manipulation (the most experienced person should perform the intubation) and administering medications.
The three common pre-medications used to prevent increased ICP during intubation are:
Lidocaine
Administered intravenously at a dose of 1.5 mg/kg 60–90 s before intubation, attenuates the direct laryngeal reflex; mixed evidence that it mitigates the RSR [3, 11].
Esmolol
Short-acting beta blocker at a dose of 1–2 mg/kg 3 min before intubation controls both heart rate and blood pressure responses to intubation, but is problematic in hypotensive patients and is rarely used in a critical care environment [12].
Fentanyl
At doses of 2–3 μg/kg, attenuates the RSR associated with intubation, and is administered as a single pre-treatment dose over 30–60 s in order to reduce chances of apnea or hypoventilation before induction and paralysis [13]. It is generally not used in patients with incipient or actual hypotension, or those who are dependent on sympathetic drive to maintain an adequate blood pressure for cerebral perfusion.
Induction is performed using an agent that will not adversely affect CPP (see also Table 4).
Etomidate
Short-acting imidazole derivative that provides sedation and muscle relaxation with minimal hemodynamic effect. Considered the most hemodynamically neutral of all commonly used induction agents and a good choice for patients with elevated ICP [14, 15].
Propofol
At a dose of 2 mg/kg intravenous (IV) push, is an alternative, but is also a potent vasodilator that routinely causes hypotension and often requires concurrent vasopressor administration to maintain CPP [16].
Thiopental
At a dose of 3 mg/kg IV push, confers cerebroprotective effect by decreasing the basal metabolic rate of oxygen utilization of the brain (CMRO2) and CBF, thus decreasing ICP. However, is a potent venodilator and negative inotrope with a strong tendency to cause hypotension and reduce CPP, even in relatively hemodynamically stable patients [8].
Ketamine
Hemodynamically neutral dissociative agent administered at 2 mg/kg IV push. In the past, was generally avoided as an agent believed to raise ICP. However, recent evidence suggests when sedation is provided concurrently, may be safe in patients with elevated ICP, and its hemodynamic profile argues for more widespread use [17–19].
Succinylcholine
Depolarizing agent that remains the neuromuscular blockade agent of choice for intubation of acutely ill neurological patients with elevated ICP, due to its rapid onset and short duration of action. Although it has been associated with transient increases in ICP, the effect is not considered clinically significant [20]. However, the neurologically ill are at higher risk for succinylcholine-induced hyperkalemia, and clinicians should consider that patients with disuse atrophy may have severe hyperkalemia following administration of a depolarizing agent. This includes patients with prior brain or spinal cord injury but also those with as little as 24–72 h of immobility, and patients with upper or lower motor neuron defects [21]. Risk may be averted by instead using a non-depolarizing agent, such as rocuronium (at 1.2–1.4 mg/kg IV push) or the longer acting agents pancuronium and vecuronium (at 0.2 mg/kg IV push).
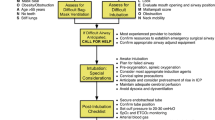
ICP during intubation also rises due to body positioning and to hypoventilation. Hypoventilation immediately causes increased pCO2, perhaps the most potent acute cerebral vasodilator. When ICP is known or suspected to be elevated, the following approach is suggested (Fig. 2):

Intubation with elevated ICP [22]
-
The head of the bed should be brought flat as briefly as possible, and immediately raised following endotracheal tube placement. Reverse Trendelenberg positioning during intubation should be considered.
-
MAP must be preserved throughout the procedure, with a goal of 80–100 mmHg, or should not drop below pre-intubation pressure. If ICP is monitored, keep CPP >60 mmHg.
-
If trauma is possible, protect the cervical-spine.
-
Pain, discomfort, agitation, and fear must be controlled with adequate analgesia and sedation.
-
Hypoventilation must be avoided, and end-tidal quantitative capnography monitoring is suggested since increased PaCO2 raises ICP.
-
Adequate pre-oxygenation with 100 % oxygen should be performed prior to induction, and the oxyhemoglobin saturation maintained >92 %. However, immediately following successful intubation and hemodynamic stabilization, the FiO2 should be reduced to 0.5, or to the lowest fraction that assures a PaO2 in the range of 110–300 mmHg. Conversely, hypoxia increases ICP and can exacerbate brain injury.
Intubating the Patient with Brain Ischemia
In suspected or proven ischemic stroke, one should proceed with intubation as with elevated ICP by avoiding hypotension during induction and post-intubation, and taking special precaution to avoid hypotension-inducing drugs, especially in hypotensive patients. When an ischemic stroke is suspected or known to be occurring, or a state of inadequate CBF exists for other reasons, brain ischemia should be presumed present.
The cerebrovascular circulation is ordinarily well collateralized, and many patients presenting with stroke symptoms can be seen to have an infarct core and an ischemic penumbra on perfusion computed tomography (CT) or magnetic resonance imaging (MRI). Under these circumstances, the ischemic penumbra may be conceptualized as a region of maximally vasodilated vessels, receiving maximal shunting of the cerebrovascular circulation, yet CBF is severely compromised and maximally compensated. Hypertension and tachycardia often reflect a physiologic, not pathophysiologic, response to this ischemia and may be necessary to maintain perfusion of the ischemic territory.
Further, certain vasoactive agents that may not drop the blood pressure or alter cerebral CPP may nonetheless reverse regional vasoconstriction in normal areas of the brain that is necessary to maintain physiologic shunting of blood to the region of ischemia. An episode of relative or actual hypotension, such as would be precipitated by the administration of vasodilator sedative medications to a relatively volume depleted patient, can worsen brain infarction by diverting blood flow from the maximally dilated watershed territories between vascular distributions.
Brain ischemia is not limited to ischemic stroke but can also be present in patients with vasospasm, traumatic brain injury (TBI), intracranial and extracranial cerebrovascular stenosis, intracerebral hemorrhage, and hypoxic-ischemic encephalopathy following resuscitation from cardiac arrest. Strong associations between episodic hypotension in the critical hours following resuscitation and poor neurological outcome have been noted in TBI and hypoxic-ischemic encephalopathy after cardiac arrest [23–26]. The intubating clinician should be aware of the risks of even a transient decrease in CBF and strive to maintain CBF and systemic vascular tone during airway management.
In addition, brain ischemia is worsened by hyperventilation—an association clearly demonstrated in TBI [27–29] and explained in the laboratory by a dramatic and immediate decrease in CBF and increase in the volume of ischemic brain tissue when hyperventilation is performed [30–32]. Clinicians should attempt to maintain normocapnea during this period, and early correlation of an arterial CO2 sample with ETCO2 is suggested, so that continuous capnography can be used to verify normocarbia [1, 33].
Intubating the Patient with Neuromuscular Weakness
Patients with neuromuscular weakness and acute or impending respiratory failure require a special approach to airway management. Respiratory failure in patients with neuromuscular disease is often associated with a weak cough and failure to clear secretions from the lower airways, leading to pneumonia, shunting, and an inability to meet ventilatory demands.
Although some patients with neuromuscular disease require immediate intubation, those with preserved bulbar function and reasonable functional ventilatory reserves should receive an aggressive trial of non-invasive ventilation combined with airway clearance by the frequent use of chest physiotherapy and cough-assist devices [34–36].
In any patient with neuromuscular weakness and a complaint of dyspnea, an assessment of respiratory function includes (see also the Acute Weakness protocol):
-
Arterial blood gas measurement
-
Interval pulmonary function testing to include negative inspiratory force (NIF) and vital capacity (FVC)
-
Assessment of bulbar function, neck strength, and cough
Candidates for intubation include patients with neuromuscular weakness and bulbar dysfunction; those who have a rapidly progressive course; and those who do not rapidly stabilize gas exchange and work of breathing with non-invasive ventilation [34]. Because of the potential for exacerbating weakness and prolonged effects of the medications, the administration of steroids, muscle relaxants, or neuromuscular blocking agents is discouraged.
In myasthenia gravis, succinylcholine is safe but requires approximately 2.5 times the dose to get the same effects [37]. Non-depolarizing agents such as rocuronium will have a prolonged duration [37]. In conditions such as Guillain–Barre, succinylcholine can precipitate life-threatening hyperkalemia, and only non-depolarizing agents should be used. Rocuronium is safe to use in neuromuscular weakness; therefore, if a neuromuscular blocking agent is used, the best choice may be rocuronium at a dose of 0.6–1.2 mg/kg.
Intubating the Patient with Cervical Spine Injury
A fundamental tenet of airway management is: when spinal column or ligamentous injury to the neck is suspected due to the mechanism of injury—such as any blunt head trauma resulting in loss of consciousness—all measures must be taken to protect the spinal cord during any movements or procedures. Pre-intubation airway maneuvers, including jaw tilt and the bag-mask ventilation, as well as direct laryngoscopy itself, can all injure the spinal cord when cervical instability is present.
Basic principles of cervical spine stabilization have been developed and refined over decades, by the American College of Surgeons’ Advanced Trauma Life Support (ATLS) course. [36]. In urgent circumstances in the field, endotracheal intubation is preferred to bag-mask ventilation or cricothyrotomy and must be performed with in-line spinal stabilization. Though cricoid pressure is no longer recommended during intubation, it definitely should not be used in patients with cervical spine injury, since it may cause posterior displacement of the cervical spine [38, 39].
Hypoxia and hypoventilation are larger risks to trauma patients than complications of endotracheal intubation; in-line spinal stabilization helps ensure safe intubating conditions when direct laryngoscopy is performed [40]. However, video and enhanced optical intubating devices are currently preferred when electively intubating patients at risk of cervical spine injury, since these devices are used with the patient’s cervical spine kept in a neutral position.
Post-intubation and Ventilation
Basic Ventilator Settings
Immediately following intubation, respiratory and hemodynamic homeostasis must be restored. Except in situations of acute brain herniation, the goals of mechanical ventilation are:
-
Normalization of oxygenation, at the lowest FiO2 that will maintain hemoglobin saturation >94 %
-
Normalization of ventilation, to correct the systemic pH to 7.35–7.45, and pCO2 to 35–45 mmHg, or the end-tidal CO2 to 30–40 mmHg
-
Normalization of the work of breathing
-
Prevention of ventilator induced lung injury
In most circumstances, clinicians should default to volume-cycled ventilation at 8 cc/kg of ideal body weight and a respiratory rate of 12–14 per minute. However, these settings must be influenced by the patient’s minute ventilation prior to induction and immediately titrated to maintain a normal pCO2. Normal pCO2 is the appropriate target unless there is chronic hypercarbia (i.e., CO2 retaining COPD or sleep-disordered breathing). In situations of chronic hypercarbia, the admission bicarbonate level should be used to estimate the “baseline” pCO2, and that level should subsequently be used as the target, or metabolic acidosis, in which case the correct target is unknown but should likely reflect a compromise between normal pCO2 and pH.
Herniation: Intentional Hyperventilation to Treat Brain Herniation and Increased ICP
When a patient develops brain herniation, hyperventilation is an appropriate part of a series of interventions designed to acutely decrease ICP and prevent widespread infarction of neuronal tissues and death [41, 42]. Maximal cerebral vasoconstriction is achieved at a pCO2 of 20 mmHg, so ventilation below this level will be ineffective and may further impede venous return to the heart, decrease blood pressure, and exacerbate cerebral hypoperfusion.
During hyperventilation, end-tidal CO2 monitoring (quantitative capnography) is suggested. As soon as other treatments to control ICP are in place (e.g., blood pressure support, osmotherapy, surgical decompression, hypothermia, metabolic therapy), hyperventilation must be rapidly weaned to restore brain perfusion [43].
Hyperventilation for increased ICP is not safe or effective when employed for a prolonged period. Hyperventilation severely reduces CBF, increases the volume of ischemic tissue, and when the patient is weaned off, may result in rebound elevation of ICP [30–32]. When prolonged hyperventilation must be employed, it is strongly recommended that cerebral metabolic monitoring (jugular oximetry, CBF, brain tissue oxygen, or cerebral microdialysis) be used together with ICP monitoring to verify the adequacy of tissue perfusion.
Titration of Ventilation
Induced Hyperventilation: Ventilation, Carbon Dioxide Tension, and Clinical Outcome
Hyperventilation causes cerebral vasoconstriction and decreased CBF, while hypoventilation causes cerebral vasodilation and increased ICP. Presumably due to this relationship, dysventilation (and especially hyperventilation) is associated with poor outcomes in TBI [27–29]. The Brain Trauma Foundation recommends targeting eucapnea in patients with brain trauma [44].
However, the relationship between arterial and central pH and pCO2 is complex and incompletely understood. When underlying metabolic acidosis is concurrent with acute brain injury, such as in diabetic ketoacidosis [45], it is likely that because of the blood–brain barrier and central nervous system (CNS) buffering capacity, CNS pH, and CBF may often be preserved despite a severely acidic systemic pH and very low pCO2.
Alternatively, in patients with chronic respiratory acidosis, the set-point of cerebral CO2 reactivity changes. It is, therefore, recommended that mechanical ventilation be adjusted to correct the pH and not the pCO2, or that the estimated “pre-morbid” pCO2 target be used (see Table 2 below). This is recommended on both a physiological and practical basis, since ventilating these patients to “normal” pCO2 targets may be extremely difficult or impossible when obstructive lung disease is present.
Since a great deal of physiologic uncertainty exists in these cases, CBF and/or metabolic monitoring are recommended whenever available to guide the titration of pH and pCO2 targets, with great attention paid to how changes in ventilation affect CBF and metabolism.
Under these circumstances, surrogates for CBF and metabolism may include jugular venous oximetry, direct intracranial monitoring of CBF or brain tissue oxygen tension, or measurement of lactate and pyruvate levels in the CNS by microdialysis techniques. It should be understood that these recommendations are based on physiologic knowledge as well as observational human and experimental animal data, and that little prospective experimental human research has been performed in this area.
Acidemic and Alkalemic Hypocarbia: Potential for Suppression of Spontaneous Hyperventilation
There are two circumstances that should be considered in patients with spontaneous hypocarbia: those whose response to systemic metabolic acidosis accounts for their high ventilatory demand, and those (alkalotic) patients in whom ventilation exceeds systemic metabolic needs.
In patients whose ventilation is driven by metabolic acidosis, suppression of the respiratory drive with sedation or neuromuscular blockade is not recommended, unless direct measurement of brain chemistry suggests that hyperventilation is linked directly to cerebral metabolic crisis. Under these circumstances, clinicians must find another means to buffer systemic pH.
It has been observed in TBI that while intubated and mechanically ventilated patients presenting with hypocarbia have worse outcomes than their normocarbic peers, non-intubated patients presenting with hypocarbia do not—suggesting that such hypercarbia may be a physiologic response and should not be suppressed [28].
Despite decades of observation and consideration, little is known about alkalemic hypocarbia in patients with an acute brain injury. Alkalemic hypocarbia following brain injury may be theoretically explained by a variety of physiologic and pathophysiologic mechanisms, more than one of which may be present in an individual patient:
-
Brain tissue acidosis requiring acute hyperventilation as a buffer until CNS bicarbonate-generating compensatory mechanisms can catch up
-
Inadequately treated pain, anxiety, fear, or agitation
-
Fever
-
Auto-regulation of elevated ICP
-
Heme breakdown products or a lactic acid load in the ventricular system
-
Direct pressure on chemoreceptors present in the floor of the 4th ventricle
-
Physiologic dysregulation of the medullary respiratory rhythm generator, which has afferent inputs from the pons, mesencephalon, and higher cortical centers
Since it is rarely known whether alkalemic hypocapnia is a physiologic or pathophysiologic process, suppression of this respiratory activity is recommended only in response to evidence that hyperventilation is causing direct harm, either directly by inducing cerebral ischemia or indirectly by increased systemic metabolic demands and work of breathing.
Oxygenation and Outcomes
Despite the traditional view that oxygen is good, it is now apparent that the supra-physiologic levels of oxygen frequently provided to acutely ill patients have the potential to worsen reperfusion injury [46, 47]. The mechanism is likely by potentiating the formation of reactive oxygen species in post-ischemic tissue beds and further impairing mitochondrial function [48]. Conversely, hypoxia is a major source of secondary brain injury [49], and the injured and ischemic brain is particularly vulnerable to low oxygen levels.
Long hypothesized based on laboratory and animal data, hyperoxia at a level of PaO2 > 300 mmHg on the first arterial blood gas following resuscitation is independently associated with poor outcomes in humans following TBI [48] and cardiac arrest [47, 50], though not all data are in accordance [51]. Hyperoxia drives the formation of reactive oxygen species, overwhelming antioxidants at sites of tissue injury; directly injures respiratory epithelium and alveoli inducing inflammation; drives hypercarbia; and leads to absorption atelectasis in the lung.
It is recommended that 100 % oxygen be provided for pre-oxygenation immediately prior to intubation, but that oxygen be immediately weaned following intubation to 50 %, or the lowest FiO2 that will support an oxyhemoglobin saturation of 95–100 %. This normoxic resuscitation strategy is recommended in 2010 American Heart Association Guidelines for post-resuscitation care after cardiac arrest [51].
Oxygenation and Ventilation Monitoring
Oxygenation should be monitored by pulse oximetry or by arterial blood gas analysis when oximetry is suspected to be inaccurate. Conditions of poor perfusion to the extremities, acidosis, vasopressor use, anemia, carboxyhemoglobinemia and methemoglobinemia, and hypoxia all have the potential to compromise the accuracy of pulse oximetry measurements [52].
Ventilation is traditionally monitored by serial arterial blood gas analysis, though venous blood gas analysis may provide an adequate surrogate during titration of mechanical ventilation, or when arterial samples cannot be obtained. End-tidal quantitative capnography of exhaled gases provides an appealing continuous measurement and is extremely useful to monitor trends in ventilation.
One study showed that severely hyperventilated head trauma patients (pCO2 < 25 mmHg) in the prehospital environment had higher mortality, and that use of quantitative capnography by paramedics significantly decreased the incidence of hyperventilation [53]. A similar study in patients with major trauma showed a much higher incidence of “normocapnea” on hospital arrival when ETCO2 was monitored by medics.
Since ETCO2 measurements reflect not only ventilation but also systemic perfusion, the correlation between ETCO2 and pCO2 in the blood is variable. In an inpatient environment, ETCO2 measurements should always be correlated with an arterial pCO2 sample. ETCO2 and pCO2 may also vary significantly when lung disease and ventilation-perfusion mismatch are present [54].
Lung Injury
Patients with acute lung injury (ALI) or the acute respiratory distress syndrome (ARDS) are vulnerable to lung injury known variably as ventilator induced lung injury (VILI) or ventilator associated lung injury (VALI). ALI and ARDS represent a spectrum of disease, in which there exist bilateral parenchymal pulmonary infiltrates, significant hypoxia, absence of left ventricular dysfunction, and an acute onset of symptoms [55]. These patients often require high levels of oxygen and ventilator pressures to achieve adequate gas exchange.
Patients with ALI and ARDS have high circulating levels of inflammatory mediators, which are associated with injury to other vital organs, and are exacerbated by injurious techniques of ventilation. VALI is thought to be caused by:
-
Barotauma, induced by high ventilator pressures, and particularly a high plateau pressure
-
Volutrauma, induced by higher tidal volumes and often despite low ventilator pressures
-
Atelectrauma, or the shearing injury caused by recurrent opening and closing of alveolar sacs that may lack adequate surfactant
-
High inspired fraction of oxygen
-
High levels of circulating inflammatory cytokines
Many modes and techniques of ventilation have been proposed to manage the severe gas exchange abnormalities associated with ARDS, though only a few important issues are covered here.
Patients with ALI or ARDS should be ventilated using a strategy of low tidal volumes (6 cc/kg); low plateau pressures (<30 mmHg); positive end expiratory pressure (PEEP) adequate to prevent cyclic collapse of alveolar units; and inhaled oxygen fraction rapidly weaned to 0.6 or less, using PEEP and body positioning to best advantage.
Although the landmark study of low tidal volume mechanical ventilation [56] emphasizes permissive hypercarbia, fluctuations of carbon dioxide levels are potent mediators of CBF, and ICP and must be carefully considered in patients with elevated ICP or compromised CBF.
Several very small investigations suggest that lung protective ventilation strategies causing mild hypercarbia in patients with elevated ICP may be tolerated [57, 58], but more data are needed before this may be considered safe in routine practice. Prone positioning seems to increase ICP [59].
When lung compliance is high, PEEP has the potential to be transmitted to the intrathoracic vessels and indirectly increase ICP. Although this physiology was once used to justify low-PEEP ventilation in patients with head injury, subsequent research has shown PEEP in brain-injured patients to be well tolerated, especially when lung compliance is poor and adequate blood pressure is maintained [60, 61]. Ventilation without PEEP is discouraged, due to the likelihood of inducing lung injury [62]. However, the relationship of PEEP to ICP is of concern and should be individually reviewed based on each patient’s physiology.
Sedation
Sedation use in the neurocritically ill is paradoxically necessary yet fundamentally undesirable. Sedation may be needed to alleviate fear and anxiety, reduce ICP and cerebral oxygen consumption, facilitate intubation and tolerance of mechanical ventilation, or to reduce sympathetic nervous activity. Conversely, sedation makes accurate neurological examination—the cornerstone of clinical assessment—difficult or impossible. Acute changes in brain physiology become difficult to detect, and the accuracy of neuroprognostication is decreased [63].
Sedation often causes vasodilation, threatening cerebral perfusion by hypotension but also by reversing physiologically advantageous shunting of blood into areas of ischemia. It is possible that prolonged deep sedation may worsen cognitive outcomes and contribute to muscle weakness. Even short-acting sedatives are known to build up in fatty tissues, causing effects well beyond their intended duration, and no commonly employed sedative has been well studied in a brain-injured population, as regards the duration of effect or adverse consequences.
Decisions regarding the need for craniotomy, endovascular therapies, ventricular drainage, ICP monitoring, therapeutic temperature management, and many other potentially morbid but also lifesaving therapies require an accurate neurological assessment. Especially in the first hours of care, the sedation of patients with unstable intracranial pathophysiology should be minimized when it can safely and humanely be limited.
This does not mean that patients should be agitated, uncomfortable, severely hypertensive, or unsafe. It means simply that the need for sedation must be weighed against the need for accurate neurological assessment and tailored to the individual patient and situation. Even more than with other critically ill patients, medication-induced coma for neurologically compromised patients is usually not desirable.
Necessity of Sedation
Complications associated with undersedation include ventilator dysynchrony, patient injury, agitation, anxiety, device removal [64–66], and elevated ICP [67]. Adequate sedation is paramount in all therapeutic algorithms for the treatment of increased ICP [68, 69], since psychomotor restlessness, pain, and autonomic stress all adversely affect ICP, CBF, CPP, and the cerebral metabolic rate for oxygen metabolism (CMRO2). In this respect, adequate analgesia and sedation make an essential contribution to preventing or limiting secondary brain damage. Nevertheless, there are insufficient data to confirm that sedation and analgesia per se reduce ICP and improve neurological outcome [68]. Conversely, in a general intensive care unit (ICU) population, the use of excessive sedation and analgesia contributes to increased duration of mechanical ventilation and longer length of stay in the ICU and hospital [70–72], as well as increased rates of depression, post-traumatic stress disorder, infections, and long-term neurocognitive impairments [73–75].
Randomized controlled trials demonstrate that protocols requiring decreases in sedative doses or daily interruption of sedative and analgesic drugs can reduce lengths of mechanical ventilation and ICU stay and reduce drug doses administered [70–72]. Unless deep sedation or general anesthesia is desired, analgesia should precede sedation. Analgesia-based “sedation” is an evolving trend in general critical care, and a recent randomized trial suggests improved outcomes among mechanically ventilated patients receiving primarily opioid analgesia with no sedation [76].
Many patients with adequate pain control do not require sedation, and, conversely, most sedative medications provide no analgesia. Sedation without pain control may be an important cause of delirium. Infusion of short acting analgesics allows for interruption and neurological assessment and intervals. In particular, a mechanistic review suggests that remifentanil—a potent narcotic analgesic with some sedating properties and an extremely rapid pharmacokinetic profile—may be cost effective when ICU length of stay is considered [77], though superiority over fentanyl has not been demonstrated [78].
Environmental stimuli are important triggers of anxiety and agitation. Providing a calm and reassuring environment, with attention to day–night cycles, restriction of noise, use of appropriate music, and/or the reassuring presence of friends and family may decrease agitation and anxiety, making sedation unnecessary [79]. These environmental measures are especially important when a dominant-hemisphere lesion causes aphasia and attempts at verbal communication generate agitated behaviors. The use of “sitters” to re-direct and re-orient confused or agitated patients is preferred to the use of sedating medications.
Patients with acute brain injury often have deficits in short-term memory, concentration, and emotional control, and their confusion may cause agitation. Confused patients require gentle and repeated re-orientation to situation and circumstances, which may obviate the need for sedation.
Given the potential of many sedatives (especially the benzodiazepines) to cause delirium, agitated delirium occasionally may be more effectively treated with antipsychotic medications than sedatives, though antipsychotic medications may affect neurological recovery [80–82]. Examples of antipsychotic medication (each with its own adverse-events profile) that may obviate the need for sedatives include haloperidol, quetiapine, olanzipine, and risperidol.
Common Sedatives in Neurological Intensive Care
Prior to the release of dexmedetomidine in Canada, one review of Canadian pharmacy databases and interviews with caregivers in three Canadian neuro-intensive care units (NICUs) [83] found that fentanyl was the most commonly used analgesic. The same review showed that propofol was the most common sedative agent in non-trauma NICUs and some trauma NICUs, with midazolam also used in some trauma NICUs.
Propofol
Propofol is perhaps better studied than other agents in neurological critical care. Pharmacologically, its lipid formulation allows for rapid penetration of the blood–brain barrier, with rapid onset and cessation of action. It has potent and immediate depressant effects on cerebral electrical and metabolic activity, and it does not require renal or hepatic metabolism for elimination. Disadvantages include robust vasodilating and hypotensive effects, a considerable intravenous lipid load, and the potential for the rare, but frequently fatal, propofol infusion syndrome, especially in children and in adults at higher doses.
Propofol has been used to sedate neurosurgical patients to reduce elevated ICP [84, 85]. Propofol and morphine are associated with improved control of ICP compared with morphine alone in the treatment of severe TBI [85], and propofol reduced elevated ICP more effectively than fentanyl following severe TBI [86]. Propofol infusions to reduce elevated ICP may need to be continued longer than usually recommended for routine sedation [87], and high doses for refractory status epilepticus or brain trauma has been associated with propofol infusion syndrome [88].
Benzodiazepines
Midazolam is an appealing sedative option given the rapid onset of action and short duration of effect with bolus administration—making it an ideal agent for procedural sedation. In addition, due to its potent gamma-aminobutyric acid (GABA) activity and relatively benign hemodynamic profile, midazolam is an important drug in refractory status epilepticus. Yet as a long-term sedative for general ICU use, midazolam accumulates in adipose tissues, significantly prolonging duration of action unless interruptions or down-titration of dose are routinely utilized.
Bolus-dose midazolam is a good choice for intermittent agitation in a NICU population, while midazolam infusion is associated with prolonged mechanical ventilation [89, 90]. Though most studies suggest the impact of midazolam on hemodynamics is similar compared to dexmedetomidine or propofol, a recent report suggests less instability compared to dexmedetomidine [90].
Lorazepam is a longer acting benzodiazepine when used in the short-term, but its duration of action is shorter than midazolam when infused for more than 1 to 2 days. The strong GABA activity of lorazepam suppresses electrical and metabolic brain activity. Unlike midazolam, lorazepam is formulated in propylene glycol, which can accumulate to toxic levels causing metabolic acidosis and kidney injury. At lorazepam infusion rates above 3 mg/h or daily doses approaching 1 mg/kg, the osmolar gap should be followed, and alternative agents should be used if the osmolar gap rises above 10–12 mOsm/L [91, 92].
Dexmedetomidine
Dexmedetomidine, a centrally acting alpha agonist similar to clonidine, but more specific for the alpha-2 receptor than clonidine, is increasingly utilized for ICU sedation. Desirable properties include rapid onset and termination of activity, mild to moderate sedation without significant respiratory depressant action, analgesic effects, and less delirium than the benzodiazepines [93]. Undesirable properties include a high incidence of bradycardia and hypotension [90]. In addition, dexmedetomidine may produce less hemodynamic intolerance than clonidine, which is available intravenously in many countries but not in the United States.
In a prospective, randomized, double-blind study of 18 awake and intubated brain-injured patients using a crossover design [94], each patient received fentanyl–propofol and fentanyl–dexmedetomidine. Both drugs were titrated to the validated 100-point Hopkins Adapted Cognitive Exam (ACE) cognitive battery. The difference in the change of ACE scores between dexmedetomidine and propofol was 19.2 (95 % CI 12.3–26.1 p < 0.001) favoring improved ACE scores with dexmedetomidine, suggesting better cognitive function.
Several case reports and case series have evaluated the potential role of dexmedetomidine for sedation in the NICU. One reported successful sedation with dexmedetomidine in a challenging TBI patient with alcohol withdrawal syndrome when benzodiazepines clouded the patient’s neurological examination and depressed ventilatory drive [95].
Another described six patients with TBI or intraventricular hemorrhage treated with dexmedetomidine sedation for 66 h at a mean dose of 0.67 mcg/kg/h in an effort to wean off midazolam or propofol and fentanyl, which was successful in all cases [96]. Though not clinically significant, two patients experienced decreases in heart rate with dexmedetomidine (from 101 to 69 beats per minute and from 76 to 68 beats per minute), and two other patients experienced different changes in systolic blood pressure with dexmedetomidine (from 150 to 138 mmHg, and 126 to 139 mmHg).
Barbiturates
Although out of favor due to prolonged duration of action as well as cardiodepressant and possibly immunosuppressant properties, barbiturates remain second-line therapy for the control of ICP after propofol. They remain in widespread use to control refractory status epilepticus, and their potent effects on cerebral metabolic and electrical activity make them an appealing class of agents for sedation in the NICU. Pentobarbital serves as a potent agent for deep sedation in patients with refractory status epilepticus or elevated ICP [97–99].
Analgesia-First Sedation
Investigators at a single center randomized intubated general ICU patients receiving bolus-dose morphine as needed to either “no sedation” or “sedation with propofol and midazolam.” “No sedation” patients required more morphine than “sedation” patients but also had more ventilator-free days and a shorter ICU length of stay, without more adverse events related to undersedation but a higher incidence of delirium [76].
Another randomized, open-label, multicenter study compared two strategies: an analgesia-first approach with remifentanil supplemented as needed with propofol (in the first 3 days) and midazolam for day 4 and beyond; and a hypnotic-based regimen using propofol (for the first 3 days) or midazolam (after day 4) with supplemental analgesia with fentanyl or morphine [100]. Both regimens were titrated to a Sedation Agitation Scale (SAS) score of 1–3 and a pain intensity score of 1–2. Variability of neurological assessment and assessment times were less when using remifentanil compared to fentanyl or morphine. Patients receiving the analgesia-first approach with remifentanil were extubated more quickly than those treated with morphine but were not different than those receiving fentanyl. Remifentanil was well tolerated and provided comparable hemodynamic stability to the hypnotic-based regimen. Over three times as many users rated analgesia-based sedation with remifentanil “very good” or “excellent” compared with the hypnotic-based regimen.
Sedation Targets and Monitoring
Sedation should be titrated to a validated sedation scale or use an electrophysiologic endpoint when neuromuscular blockade is employed or burst-suppression is desired. A recent review of sedation assessment tools in the neurocritical care setting concluded that the SAS and Richmond Agitation Sedation Scale (RASS) are valid and useful for NICU patients, and the bispectral index (BIS) may have a role in monitoring deeply sedated patients in the NICU [84, 101–103].
Regarding assessment of delirium, no assessment tools have been validated in neurocritical care patients, though several studies that used the Intensive Care Delirium Screening Checklist enrolled NICU patients [102, 104, 105]. A recent, highly insightful review of the topic is also available [106].
Sedation for neurocritical care patients remains highly variable, as shown by the inconsistent clinical approaches to sedation during endovascular intervention for ischemic stroke. One survey of 49 members of the Society of Vascular and Interventional Neurology found that general anesthesia was the most common approach, closely followed by conscious sedation either by an anesthesia team or with local anesthetic [107].
A retrospective study of 980 patients treated with endovascular therapy for anterior circulation stroke showed that the 44 % treated with general anesthesia had no delay in time to therapy compared to conscious sedation (306 vs. 296 min), but had the same rate of hemorrhage and an independent association with poor outcome and mortality [108]. A similar study of 126 patients suggested that non-intubated patients had lower mortality, smaller infarct size, and better clinical outcomes [109]. These retrospective studies await prospective confirmation but suggest that conscious sedation may be safe and associated with improved outcomes.
Several studies have addressed the sedation monitoring approaches and medication choices for NICU patients. One prospective, randomized trial of 67 mechanically ventilated adult patients sedated with propofol showed that the BIS monitor added to routine sedation scale monitoring significantly reduced the propofol dose and the time to awakening when compared to subjective scale monitoring alone [110].
Daily Interruption of Sedation
Sedation protocols requiring a daily interruption of sedation [71] are not yet sufficiently evaluated in patients with underlying cerebral disease. In addition to adequate analgesia, which is essential in severe cerebral trauma, additional analgesia and sedation must be provided for nursing interventions and any surgical interventions. In the acute phase of intensive treatment, deep sedation (RASS score of −5 or SAS score of 1) should generally be targeted, especially if intracranial hypertension >15–20 mmHg) is present [111, 112].
Communication
When communicating to an accepting or referring physician about this patient, consider including the key elements listed in Table 3.
References
Davis DP, Dunford JV, Ochs M, Park K, Hoyt DB. The use of quantitative end-tidal capnometry to avoid inadvertent severe hyperventilation in patients with head injury after paramedic rapid sequence intubation. J Trauma. 2004;56:808–14.
Coplin WM, Pierson DJ, Cooley KD, Newell DW, Rubenfeld GD. Implications of extubation delay in brain-injured patients meeting standard weaning criteria. Am J Respir Crit Care Med. 2000;161:1530–6.
Walls RM, Murphy MF. Manual of emergency airway management. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2008.
Sagarin MJ, Barton ED, Chng YM, Walls RM. National Emergency Airway Registry I. Airway management by US and Canadian emergency medicine residents: a multicenter analysis of more than 6,000 endotracheal intubation attempts. Ann Emerg Med. 2005;46:328–36.
Li J, Murphy-Lavoie H, Bugas C, Martinez J, Preston C. Complications of emergency intubation with and without paralysis. Am J Emerg Med. 1999;17:141–3.
Sakles JC, Laurin EG, Rantapaa AA, Panacek EA. Airway management in the emergency department: a one-year study of 610 tracheal intubations. Ann Emerg Med. 1998;31:325–32.
Walls RM. Rapid-sequence intubation in head trauma. Ann Emerg Med. 1993;22:1008–13.
Bedford RF, Persing JA, Pobereskin L, Butler A. Lidocaine or thiopental for rapid control of intracranial hypertension? Anesth Analg. 1980;59:435–7.
Gabriel EJ, Ghajar J, Jagoda A, et al. Guidelines for prehospital management of traumatic brain injury. J Neurotrauma. 2002;19:111–74.
Weingart S. Additional thoughts on the controversy of lidocaine administration before rapid sequence intubation in patients with traumatic brain injuries. Ann Emerg Med. 2007;50:353.
Salhi B, Stettner E. In defense of the use of lidocaine in rapid sequence intubation. Ann Emerg Med. 2007;49:84–6.
Feng CK, Chan KH, Liu KN, Or CH, Lee TY. A comparison of lidocaine, fentanyl, and esmolol for attenuation of cardiovascular response to laryngoscopy and tracheal intubation. Acta Anaesthesiol Sin. 1996;34:61–7.
Reynolds SF, Heffner J. Airway management of the critically ill patient: rapid-sequence intubation. Chest. 2005;127:1397–412.
Bergen JM, Smith DC. A review of etomidate for rapid sequence intubation in the emergency department. J Emerg Med. 1997;15:221–30.
Moss E, Powell D, Gibson RM, McDowall DG. Effect of etomidate on intracranial pressure and cerebral perfusion pressure. Br J Anaesth. 1979;51:347–52.
Hug CC Jr, McLeskey CH, Nahrwold ML, et al. Hemodynamic effects of propofol: data from over 25,000 patients. Anesth Analg. 1993;77:S21–9.
Bar-Joseph G, Guilburd Y, Tamir A, Guilburd JN. Effectiveness of ketamine in decreasing intracranial pressure in children with intracranial hypertension. J Neurosurg Pediatr. 2009;4:40–6.
Langsjo JW, Maksimow A, Salmi E, et al. S-ketamine anesthesia increases cerebral blood flow in excess of the metabolic needs in humans. Anesthesiology. 2005;103:258–68.
Bourgoin A, Albanese J, Wereszczynski N, Charbit M, Vialet R, Martin C. Safety of sedation with ketamine in severe head injury patients: comparison with sufentanil. Crit Care Med. 2003;31:711–7.
Kovarik WD, Mayberg TS, Lam AM, Mathisen TL, Winn HR. Succinylcholine does not change intracranial pressure, cerebral blood flow velocity, or the electroencephalogram in patients with neurologic injury. Anesth Analg. 1994;78:469–73.
Martyn JA, Richtsfeld M. Succinylcholine-induced hyperkalemia in acquired pathologic states: etiologic factors and molecular mechanisms. Anesthesiology. 2006;104:158–69.
Seder DB, Mayer SA. Critical care management of subarachnoid hemorrhage and ischemic stroke. Clin Chest Med. 2009;30:103–22, viii–ix.
Chesnut RM, Marshall SB, Piek J, Blunt BA, Klauber MR, Marshall LF. Early and late systemic hypotension as a frequent and fundamental source of cerebral ischemia following severe brain injury in the Traumatic Coma Data Bank. Acta Neurochir Suppl. 1993;59:121–5.
Prough DS, Lang J. Therapy of patients with head injuries: key parameters for management. J Trauma. 1997;42:S10–8.
Trzeciak S, Jones AE, Kilgannon JH, et al. Significance of arterial hypotension after resuscitation from cardiac arrest. Crit Care Med. 2009;37:2895–903. quiz 904.
Kilgannon JH, Roberts BW, Reihl LR, et al. Early arterial hypotension is common in the post-cardiac arrest syndrome and associated with increased in-hospital mortality. Resuscitation. 2008;79:410–6.
Dumont TM, Visioni AJ, Rughani AI, Tranmer BI, Crookes B. Inappropriate prehospital ventilation in severe traumatic brain injury increases in-hospital mortality. J Neurotrauma. 2010;27:1233–41.
Davis DP, Idris AH, Sise MJ, et al. Early ventilation and outcome in patients with moderate to severe traumatic brain injury. Crit Care Med. 2006;34:1202–8.
Davis DP, Stern J, Sise MJ, Hoyt DB. A follow-up analysis of factors associated with head-injury mortality after paramedic rapid sequence intubation. J Trauma. 2005;59:486–90.
Coles JP, Fryer TD, Coleman MR, et al. Hyperventilation following head injury: effect on ischemic burden and cerebral oxidative metabolism. Crit Care Med. 2007;35:568–78.
Coles JP, Minhas PS, Fryer TD, et al. Effect of hyperventilation on cerebral blood flow in traumatic head injury: clinical relevance and monitoring correlates. Crit Care Med. 2002;30:1950–9.
Diringer MN, Videen TO, Yundt K, et al. Regional cerebrovascular and metabolic effects of hyperventilation after severe traumatic brain injury. J Neurosurg. 2002;96:103–8.
Walsh BK, Crotwell DN, Restrepo RD. Capnography/Capnometry during mechanical ventilation: 2011. Respir Care. 2011;56:503–9.
Seneviratne J, Mandrekar J, Wijdicks EF, Rabinstein AA. Noninvasive ventilation in myasthenic crisis. Arch Neurol. 2008;65:54–8.
Flandreau G, Bourdin G, Leray V, et al. Management and long-term outcome of patients with chronic neuromuscular disease admitted to the intensive care unit for acute respiratory failure: a single-center retrospective study. Respir Care. 2011;56:953–60.
Piastra M, Antonelli M, Caresta E, Chiaretti A, Polidori G, Conti G. Noninvasive ventilation in childhood acute neuromuscular respiratory failure: a pilot study. Respiration. 2006;73:791–8.
Abel M, Eisenkraft JB. Anesthetic implications of myasthenia gravis. Mt Sinai J Med. 2002;69:31–7.
Rice MJ, Mancuso AA, Gibbs C, Morey TE, Gravenstein N, Deitte LA. Cricoid pressure results in compression of the postcricoid hypopharynx: the esophageal position is irrelevant. Anesth Analg. 2009;109:1546–52.
Ellis DY, Harris T, Zideman D. Cricoid pressure in emergency department rapid sequence tracheal intubations: a risk-benefit analysis. Ann Emerg Med. 2007;50:653–65.
Grande CM, Barton CR, Stene JK. Appropriate techniques for airway management of emergency patients with suspected spinal cord injury. Anesth Analg. 1988;67:714–5.
Koenig MA, Bryan M, Lewin JL 3rd, Mirski MA, Geocadin RG, Stevens RD. Reversal of transtentorial herniation with hypertonic saline. Neurology. 2008;70:1023–9.
Qureshi AI, Geocadin RG, Suarez JI, Ulatowski JA. Long-term outcome after medical reversal of transtentorial herniation in patients with supratentorial mass lesions. Crit Care Med. 2000;28:1556–64.
Oertel M, Kelly DF, Lee JH, et al. Efficacy of hyperventilation, blood pressure elevation, and metabolic suppression therapy in controlling intracranial pressure after head injury. J Neurosurg. 2002;97:1045–53.
Badjatia N, Strongilis E, Prescutti M, et al. Metabolic benefits of surface counter warming during therapeutic temperature modulation. Crit Care Med. 2009;37:1893–7.
Wood EG, Go-Wingkun J, Luisiri A, Aceto T Jr. Symptomatic cerebral swelling complicating diabetic ketoacidosis documented by intraventricular pressure monitoring: survival without neurologic sequela. Pediatr Emerg Care. 1990;6:285–8.
Balan IS, Fiskum G, Hazelton J, Cotto-Cumba C, Rosenthal RE. Oximetry-guided reoxygenation improves neurological outcome after experimental cardiac arrest. Stroke. 2006;37:3008–13.
Brucken A, Kaab AB, Kottmann K, et al. Reducing the duration of 100 % oxygen ventilation in the early reperfusion period after cardiopulmonary resuscitation decreases striatal brain damage. Resuscitation. 2010;81:1698–703.
Davis DP, Meade W, Sise MJ, et al. Both hypoxemia and extreme hyperoxemia may be detrimental in patients with severe traumatic brain injury. J Neurotrauma. 2009;26:2217–23.
Kilgannon JH, Jones AE, Shapiro NI, et al. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA. 2010;303:2165–71.
Kilgannon JH, Jones AE, Parrillo JE, et al. Relationship between supranormal oxygen tension and outcome after resuscitation from cardiac arrest. Circulation. 2011;123:2717–22.
Bellomo R, Bailey M, Eastwood GM, et al. Arterial hyperoxia and in-hospital mortality after resuscitation from cardiac arrest. Crit Care. 2011;15:R90.
Peberdy MA, Callaway CW, Neumar RW, et al. Part 9: post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S768–86.
Menchem CC. Pulse Oximetry. In: Basow DS, editor. UpToDate. Waltham, MA: UpToDate Publishing; 2012.
Helm M, Schuster R, Hauke J, Lampl L. Tight control of prehospital ventilation by capnography in major trauma victims. Br J Anaesth. 2003;90:327–32.
Hardman JG, Aitkenhead AR. Estimating alveolar dead space from the arterial to end-tidal CO(2) gradient: a modeling analysis. Anesth Analg. 2003;97:1846–51.
Artigas A, Bernard GR, Carlet J, et al. The American-European Consensus Conference on ARDS, part 2: ventilatory, pharmacologic, supportive therapy, study design strategies, and issues related to recovery and remodeling. Acute respiratory distress syndrome. Am J Respir Crit Care Med. 1998;157:1332–47.
Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;342:1301–8.
Petridis AK, Doukas A, Kienke S, et al. The effect of lung-protective permissive hypercapnia in intracerebral pressure in patients with subarachnoid haemorrhage and ARDS. A retrospective study. Acta Neurochir. 2010;152:2143–5.
Bennett SS, Graffagnino C, Borel CO, James ML. Use of high frequency oscillatory ventilation (HFOV) in neurocritical care patients. Neurocrit Care. 2007;7:221–6.
Reinprecht A, Greher M, Wolfsberger S, Dietrich W, Illievich UM, Gruber A. Prone position in subarachnoid hemorrhage patients with acute respiratory distress syndrome: effects on cerebral tissue oxygenation and intracranial pressure. Crit Care Med. 2003;31:1831–8.
Caricato A, Conti G, Della Corte F, et al. Effects of PEEP on the intracranial system of patients with head injury and subarachnoid hemorrhage: the role of respiratory system compliance. J Trauma. 2005;58:571–6.
Muench E, Bauhuf C, Roth H, et al. Effects of positive end-expiratory pressure on regional cerebral blood flow, intracranial pressure, and brain tissue oxygenation. Crit Care Med. 2005;33:2367–72.
Koutsoukou A, Perraki H, Raftopoulou A, et al. Respiratory mechanics in brain-damaged patients. Intensive Care Med. 2006;32:1947–54.
Samaniego EA, Mlynash M, Caulfield AF, Eyngorn I, Wijman CA. Sedation confounds outcome prediction in cardiac arrest survivors treated with hypothermia. Neurocrit Care. 2011;15:113–9.
Riker RR, Fraser GL. Altering intensive care sedation paradigms to improve patient outcomes. Anesthesiol Clin. 2011;29:663–74.
Jacobi J, Fraser GL, Coursin DB, et al. Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med. 2002;30:119–41.
Fraser GL, Riker RR, Prato BS, Wilkins ML. The frequency and cost of patient-initiated device removal in the ICU. Pharmacotherapy. 2001;21:1–6.
Skoglund K, Enblad P, Marklund N. Effects of the neurological wake-up test on intracranial pressure and cerebral perfusion pressure in brain-injured patients. Neurocrit Care. 2009;11:135–42.
Brain Trauma F, American Association of Neurological S, Congress of Neurological S, et al. Guidelines for the management of severe traumatic brain injury. VI. Indications for intracranial pressure monitoring. J Neurotrauma. 2007;24(Suppl 1):S37–44.
Citerio G, Cormio M. Sedation in neurointensive care: advances in understanding and practice. Curr Opin Crit Care. 2003;9:120–6.
Brook AD, Ahrens TS, Schaiff R, et al. Effect of a nursing-implemented sedation protocol on the duration of mechanical ventilation. Crit Care Med. 1999;27:2609–15.
Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471–7.
Mehta S, Burry L, Martinez-Motta JC, et al. A randomized trial of daily awakening in critically ill patients managed with a sedation protocol: a pilot trial. Crit Care Med. 2008;36:2092–9.
Treggiari MM, Romand JA, Yanez ND, et al. Randomized trial of light versus deep sedation on mental health after critical illness. Crit Care Med. 2009;37:2527–34.
Jones C, Backman C, Capuzzo M, Flaatten H, Rylander C, Griffiths RD. Precipitants of post-traumatic stress disorder following intensive care: a hypothesis generating study of diversity in care. Intensive Care Med. 2007;33:978–85.
Hopkins RO, Jackson JC. Long-term neurocognitive function after critical illness. Chest. 2006;130:869–78.
Strom T, Martinussen T, Toft P. A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomised trial. Lancet. 2010;375:475–80.
Spies C, Macguill M, Heymann A, et al. A prospective, randomized, double-blind, multicenter study comparing remifentanil with fentanyl in mechanically ventilated patients. Intensive Care Med. 2011;37:469–76.
Al MJ, Hakkaart L, Tan SS, Bakker J. Cost-consequence analysis of remifentanil-based analgo-sedation vs. conventional analgesia and sedation for patients on mechanical ventilation in the Netherlands. Crit Care. 2010;14:R195.
Khalifezadeh A, Safazadeh S, Mehrabi T, Mansour BA. Reviewing the effect of nursing interventions on delirious patients admitted to intensive care unit of neurosurgery ward in Al-Zahra Hospital, Isfahan University of Medical Sciences. Iran J Nurs Midwifery Res. 2011;16:106–12.
Kline AE, Hoffman AN, Cheng JP, Zafonte RD, Massucci JL. Chronic administration of antipsychotics impede behavioral recovery after experimental traumatic brain injury. Neurosci Lett. 2008;448:263–7.
Hoffman AN, Cheng JP, Zafonte RD, Kline AE. Administration of haloperidol and risperidone after neurobehavioral testing hinders the recovery of traumatic brain injury-induced deficits. Life Sci. 2008;83:602–7.
Kline AE, Massucci JL, Zafonte RD, Dixon CE, DeFeo JR, Rogers EH. Differential effects of single versus multiple administrations of haloperidol and risperidone on functional outcome after experimental brain trauma. Crit Care Med. 2007;35:919–24.
Teitelbaum JS, Ayoub O, Skrobik Y. A critical appraisal of sedation, analgesia and delirium in neurocritical care. Can J Neurol Sci. 2011;38:815–25.
Herregods L, Verbeke J, Rolly G, Colardyn F. Effect of propofol on elevated intracranial pressure. Preliminary results. Anaesthesia. 1988;43:107–9.
Kelly DF, Goodale DB, Williams J, et al. Propofol in the treatment of moderate and severe head injury: a randomized, prospective double-blinded pilot trial. J Neurosurg. 1999;90:1042–52.
Herregods L, Mergaert C, Rolly G, Collardyn F. Comparison of the effects of 24-hour propofol or fentanyl infusions on intracranial pressure. J Drug Dev. 1989;2:99–100.
Cremer OL, Moons KG, Bouman EA, Kruijswijk JE, de Smet AM, Kalkman CJ. Long-term propofol infusion and cardiac failure in adult head-injured patients. Lancet. 2001;357:117–8.
Iyer VN, Hoel R, Rabinstein AA. Propofol infusion syndrome in patients with refractory status epilepticus: an 11-year clinical experience. Crit Care Med. 2009;37:3024–30.
Barrientos-Vega R, Mar Sanchez-Soria M, Morales-Garcia C, Robas-Gomez A, Cuena-Boy R, Ayensa-Rincon A. Prolonged sedation of critically ill patients with midazolam or propofol: impact on weaning and costs. Crit Care Med. 1997;25:33–40.
Jakob SM, Ruokonen E, Grounds RM, et al. Dexmedetomidine vs. midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA. 2012;307:1151–60.
Yahwak JA, Riker RR, Fraser GL, Subak-Sharpe S. Determination of a lorazepam dose threshold for using the osmol gap to monitor for propylene glycol toxicity. Pharmacotherapy. 2008;28:984–91.
Horinek EL, Kiser TH, Fish DN, MacLaren R. Propylene glycol accumulation in critically ill patients receiving continuous intravenous lorazepam infusions. Ann Pharmacother. 2009;43:1964–71.
Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA. 2009;301:489–99.
Mirski MA, Lewin JJ 3rd, Ledroux S, et al. Cognitive improvement during continuous sedation in critically ill, awake and responsive patients: the Acute Neurological ICU Sedation Trial (ANIST). Intensive Care Med. 2010;36:1505–13.
Tang JF, Chen PL, Tang EJ, May TA, Stiver SI. Dexmedetomidine controls agitation and facilitates reliable, serial neurological examinations in a non-intubated patient with traumatic brain injury. Neurocrit Care. 2011;15:175–81.
Grof TM, Bledsoe KA. Evaluating the use of dexmedetomidine in neurocritical care patients. Neurocrit Care. 2010;12:356–61.
Chen HI, Malhotra NR, Oddo M, Heuer GG, Levine JM, LeRoux PD. Barbiturate infusion for intractable intracranial hypertension and its effect on brain oxygenation. Neurosurgery. 2008;63:880–6. discussion 6–7.
Marshall GT, James RF, Landman MP, et al. Pentobarbital coma for refractory intra-cranial hypertension after severe traumatic brain injury: mortality predictions and one-year outcomes in 55 patients. J Trauma. 2010;69:275–83.
Claassen J, Hirsch LJ, Mayer SA. Treatment of status epilepticus: a survey of neurologists. J Neurol Sci. 2003;211:37–41.
Karabinis A, Mandragos K, Stergiopoulos S, et al. Safety and efficacy of analgesia-based sedation with remifentanil versus standard hypnotic-based regimens in intensive care unit patients with brain injuries: a randomised, controlled trial [ISRCTN50308308]. Crit Care. 2004;8:R268–80.
Riker RR, Picard JT, Fraser GL. Prospective evaluation of the Sedation-Agitation Scale for adult critically ill patients. Crit Care Med. 1999;27:1325–9.
Sessler CN, Gosnell MS, Grap MJ, et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166:1338–44.
Deogaonkar A, Gupta R, DeGeorgia M, et al. Bispectral Index monitoring correlates with sedation scales in brain-injured patients. Crit Care Med. 2004;32:2403–6.
Bergeron N, Dubois MJ, Dumont M, Dial S, Skrobik Y. Intensive Care Delirium Screening Checklist: evaluation of a new screening tool. Intensive Care Med. 2001;27:859–64.
Van Rompaey B, Elseviers MM, Schuurmans MJ, Shortridge-Baggett LM, Truijen S, Bossaert L. Risk factors for delirium in intensive care patients: a prospective cohort study. Crit Care. 2009;13:R77.
Frontera JA. Delirium and sedation in the ICU. Neurocrit Care. 2011;14:463–74.
McDonagh DL, Olson DM, Kalia JS, Gupta R, Abou-Chebl A, Zaidat OO. Anesthesia and sedation practices among neurointerventionalists during acute ischemic stroke endovascular therapy. Front Neurol. 2010;1:118.
Abou-Chebl A, Lin R, Hussain MS, et al. Conscious sedation versus general anesthesia during endovascular therapy for acute anterior circulation stroke: preliminary results from a retrospective, multicenter study. Stroke. 2010;41:1175–9.
Jumaa MA, Zhang F, Ruiz-Ares G, et al. Comparison of safety and clinical and radiographic outcomes in endovascular acute stroke therapy for proximal middle cerebral artery occlusion with intubation and general anesthesia versus the nonintubated state. Stroke. 2010;41:1180–4.
Olson DM, Thoyre SM, Peterson ED, Graffagnino C. A randomized evaluation of bispectral index-augmented sedation assessment in neurological patients. Neurocrit Care. 2009;11:20–7.
Enblad P, Nilsson P, Chambers I, et al. R3-survey of traumatic brain injury management in European Brain IT centres year 2001. Intensive Care Med. 2004;30:1058–65.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Seder, D.B., Riker, R.R., Jagoda, A. et al. Emergency Neurological Life Support: Airway, Ventilation, and Sedation. Neurocrit Care 17 (Suppl 1), 4–20 (2012). https://doi.org/10.1007/s12028-012-9753-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-012-9753-6