
Abstract
Background
Fluoroquinolone antibiotics are commonly used to treat infections and are prescribed by general practitioners, medical specialists and surgeons. Tendon injury has been associated with the use of these medications but the risk associated with newer fluoroquinolones has not been established.
Objectives
The aim of this systematic review was to evaluate the evidence from observational studies to determine the strength of the association between fluoroquinolone use and tendinopathy, and to identify risk factors for this complication.
Methods
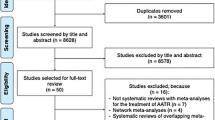
We searched MEDLINE, EMBASE and the Cochrane Collaboration from inception through May 2013 to identify observational studies focused on tendon injury and fluoroquinolones. Studies with original data were selected for inclusion following the PRISMA guidelines. Of the 560 abstracts screened, 16 relevant studies were independently rated by three authors (WW, AS, DC) using the Newcastle-Ottawa Quality Assessment Scale, and assigned a quality score out of 9. High-quality studies (i.e. scored 4.5 or higher) are summarized in detail in this article. Data were independently extracted by two authors (WW, AS).
Results
Overall, 16 studies were included in our study. Eight were deemed to be of high quality and five specifically evaluated Achilles tendon rupture. In addition, three studies examined Achilles tendinitis, and three included tendon disorders (including any tendon rupture) as an outcome. Results from these studies suggest that individuals exposed to fluoroquinolones are at increased risk for Achilles tendon rupture, particularly within the first month following exposure to the drug (odds ratios ranged from 1.1 to 7.1). One study showed an increased risk of tendon rupture in those over 60 years of age. Five studies stated that individuals taking fluoroquinolones and oral corticosteroids are at increased risk for tendon injury compared with those taking fluoroquinolones alone. Four studies examined the differential effect of a limited number of fluoroquinolones. Ofloxacin had the highest risk of tendon injury in three of the studies.
Limitations
Included studies are observational in nature and rely on self-report, which may lead to misclassification or underestimation of tendon injury.
Conclusions
Observational studies showed an increased risk of tendon injury, including tendon rupture and tendinitis, with exposure to fluoroquinolone antibiotic therapy. Although this complication appears to be rare, concomitant corticosteroids increase the risk for tendon injury, which varies depending on the fluoroquinolone used.

Similar content being viewed by others


References
Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother. 2007;41(11):1859–66.
Beyer J, Schellong S. Bilateral plantar tendinitis during levofloxacin therapy (Review, 8 refs). Br J. Clin Pharm. 2006;61(5):609.
Karistinos A, Paulos LE. “Ciprofloxacin-induced” bilateral rectus femoris tendon rupture. 17(5):406–7.
Braun D, Petitpain N, Cosserat F, Loeuille D, Bitar S, Gillet P, et al. Rupture of multiple tendons after levofloxacin therapy. Revue du Rhumatisme. 2004;71(6):586–7.
Burkhardt O, Kohnlein T, Pap T, Welte T. Recurrent tendinitis after treatment with two different fluoroquinolones. Scand J Infect Dis. 2004;36(4):315–6.
Mouzopoulos G, Stamatakos M, Vasiliadis G, Skandalakis P. Rupture of adductor longus tendon due to ciprofloxacin. Acta Ortho Belgica. 2005;71(6):743–5.
Khaliq Y, Zhanel GG. Musculoskeletal injury associated with fluoroquinolone antibiotics (Review, 43 refs). Clinics Plastic Surgery. 2005;32(4):495–502.
Ever-Silva WA, Netto Hde B, Pinto JF, Ferry FR, Neves-Motta R. Severe shoulder tendinopathy associated with levofloxacin. Braz J Infect Dis. 2012;16(4):393–5.
Tanne JH. FDA adds “black box” warning label to fluoroquinolone antibiotics. BMJ. 2008;337:a816.
Zhanel GG, Ennis K, Vercaigne L, Walkty A, Gin AS, Embil J, et al. A critical review of the fluoroquinolones: focus on respiratory infections. Drugs. 2002;62(1):13–59.
Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–72.
O’Donnell DE, Hernandez P, Kaplan A, Aaron S, Bourbeau J, Marciniuk D et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease—2008 update—highlights for primary care. Can Respir J 2008;15(Suppl A):1A–8A.
Khaliq Y, Zhanel GG. Fluoroquinolone-associated tendinopathy: a critical review of the literature. Clin Infect Dis. 2003;36(11):1404–10.
Linder JA, Huang ES, Steinman MA, Gonzales R, Stafford RS. Fluoroquinolone prescribing in the United States: 1995 to 2002. Am J Med. 2005;118:259–68.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M et al. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses.
Costa SM, Martins CC, Bonfim MC, Zina LG, Paiva SM, Pordeus IA, et al. A systematic review of socioeconomic indicators and dental caries in adults. Int J Environ Res Public Health. 2012;9:3540–74.
Wise BL, Peloquin C, Choi H, Lane NE, Zhang Y. Impact of age, sex, obesity, and steroid use on quinolone-associated tendon disorders. Amer J Med. 2012;125(12):1228.e23–8.
Lapi F, Tuccori M, Motola D, Pugi A, Vietri M, Montanaro N, et al. Safety profile of the fluoroquinolones: analysis of adverse drug reactions in relation to prescription data using four regional pharmacovigilance databases in Italy. Drug Saf. 2010;33(9):789–99.
Seeger JD, West WA, Fife D, Noel GJ, Johnson LN, Walker AM. Achilles tendon rupture and its association with fluoroquinolone antibiotics and other potential risk factors in a managed care population. Pharmacoepidemiol Drug Saf. 2006;15(11):784–92.
Corrao G, Zambon A, Bertu L, Mauri A, Paleari V, Rossi C, et al. Evidence of tendinitis provoked by fluoroquinolone treatment: a case-control study. Drug Saf. 2006;29(10):889–96.
van der Linden PD, Sturkenboom MC, Herings RM, Leufkens HM, Rowlands S, Stricker BH. Increased risk of Achilles tendon rupture with quinolone antibacterial use, especially in elderly patients taking oral corticosteroids. Arch Intern Med. 2003;163(15):1801–7.
Leone R, Venegoni M, Motola D, Moretti U, Piazzetta V, Cocci A, et al. Adverse drug reactions related to the use of fluoroquinolone antimicrobials: an analysis of spontaneous reports and fluoroquinolone consumption data from three Italian regions. Drug Saf. 2003;26(2):109–20.
Chhajed PN, Plit ML, Hopkins PM, Malouf MA, Glanville AR. Achilles tendon disease in lung transplant recipients: association with ciprofloxacin. Eur Respir J. 2002;19(3):469–71.
van der Linden PD, Sturkenboom MC, Herings RM, Leufkens HG, Stricker BH. Fluoroquinolones and risk of Achilles tendon disorders: case-control study. BMJ. 2002;324(7349):1306–7.
van der Linden PD, van Puijenbroek EP, Feenstra J, Veld BA, Sturkenboom MC, Herings RM, et al. Tendon disorders attributed to fluoroquinolones: a study on 42 spontaneous reports in the period 1988 to 1998. Arthritis Rheum. 2001;45(3):235–9.
van der Linden PD, Nab HW, Simonian S, Stricker BH, Leufkens HG, Herings RM. Fluoroquinolone use and the change in incidence of tendon ruptures in the Netherlands (Review, 23 refs). Pharm World Sci. 2001;23(3):89–92.
Pierfitte C, Royer RJ. Tendon disorders with fluoroquinolones. Therapie. 1996;51(4):419–20.
Hori K, Yamakawa K, Yoshida N, Ohnishi K, Kawakami J. Detection of fluoroquinolone-induced tendon disorders using a hospital database in Japan. Pharmacoepidemiol Drug Saf. 2012;21:886–9.
Barge-Caballero E, Crespo-Leiro MG, Paniagua-Martin MJ, Muniz J, Naya C, Bouzas-Mosquera A, et al. Quinolone-related Achilles tendinopathy in heart transplant patients: incidence and risk factors. J Heart Lung Transpl. 2008;27(1):46–51.
Sode J, Obel N, Hallas J, Lassen A. Use of fluroquinolone and risk of Achilles tendon rupture: a population-based cohort study. Eur J Clin Pharmacol. 2007;63(5):499–503.
van der Linden PD, van de Lei J, Nab HW, Knol A, Stricker BH. Achilles tendinitis associated with fluoroquinolones. Br J Clin Pharmacol. 1999;48(3):433–7.
Wilton LV, Pearce GL, Mann RD. A comparison of ciprofloxacin, norfloxacin, ofloxacin, azithromycin and cefixime examined by observational cohort studies. Br J Clin Pharmacol. 1996;41(4):277–84.
Le Huec JC, Schaeverbeke T, Chauveaux, Rivel J, Dehais J, Le Rebeller A. Epicondylitis after treatment with fluoroquinolone antibiotics. J Bone Joint Surg Br. 1995;77(293):295.
Schwald N, Debray-Meignan S. Suspected role of ofloxacin in a case of arthralgia, myalgia, and multiple tendinopathy. Revue du Rhumatisme. 1999;66:419–21.
Williams RJ III, Attia E, Wickiewicz TL, Hannafin JA. The effect of ciprofloxacin on tendon, paratenon, and capsular fibroblast metabolism. Am J Sports Med. 2000;28(3):364–9.
Hynes RO. Integrins: bidirectional, allosteric signaling machines. Cell. 2002;110:673–87.
Pouzaud F, Bernard-Beaubois K, Thevenin M, Warnet JM, Hayem G, Rat P. In vitro discrimination of fluoroquinolones toxicity on tendon cells: involvement of oxidative stress. J Pharmacol Exp Ther. 2004;308(1):394–402.
Maffulli N, Sharma P, Luscombe KL. Achilles tendinopathy: aetiology and management. J R Soc Med. 2004;97(10):472–6.
McLauchlan GJ, Handoll HH. Interventions for treating acute and chronic Achilles tendinitis. Cochrane Database Syst Rev 2001;(2):CD000232.
Marie I, Delafenetre H, Massy N, Thuillez C, Noblet C, et al. Tendinous disorders attributed to statins: a study on ninety-six spontaneous reports in the period 1990–2005 and review of the literature. Arthritis Rheum. 2008;59(3):367–72.
Acknowledgments
This study was funded by Team Grant OTG-88591 from the Canadian Institutes of Health Research (CIHR). The authors are grateful for the work of Corinne Holubowich and Pamela Richards, Information Specialists at the Health Sciences Library, Li Ka Shing Knowledge Institute, St. Michael’s Hospital and who conducted the literature searches for this review.
Author Contributions
Dr. Stephenson had full access to all of the data in the study and takes responsibility for the integrity of the data, the accuracy of the data analysis, and had final responsibility for the decision to submit for publication. Study concept and design, analysis and interpretation of data, drafting of the manuscript, and critical revision of the manuscript for important intellectual content was carried out by Drs Stephenson and Rochon, Mr. Wu and Mr. Cortes; acquisition of data was undertaken by Drs Stephenson, Wu and Cortes; statistical analysis was carried out by Drs Stephenson and Wu; funding was obtained by Dr Rochon; and study supervision was carried out by Dr Rochon.
Role of the funding source
The study sponsor did not participate in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the paper for publication.
Conflicts of interest
Drs Stephenson and Rochon, Mr. Wu and Mr. Cortes do not have any conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Stephenson, A.L., Wu, W., Cortes, D. et al. Tendon Injury and Fluoroquinolone Use: A Systematic Review. Drug Saf 36, 709–721 (2013). https://doi.org/10.1007/s40264-013-0089-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40264-013-0089-8