
Abstract
Background
Tyrosine kinase inhibitors have been shown to have marked clinical efficacy in patients with unresectable or metastatic gastrointestinal stromal tumors (GIST). We performed a comparative and prognostic analysis of our experience with surgically managed GIST to determine factors associated with adverse oncologic outcomes.
Methods
Oncologic outcomes of 191 patients with primary GIST surgically managed between 1978 and 2004 at a single institution were reviewed. Prognostic factors were analyzed by Cox analysis (hazard ratio [HR] and 95% confidence interval [95% CI]) and included age, sex, disease presentation (asymptomatic vs. symptomatic), tumor site (stomach, small bowel, colorectal), disease extent (localized vs. metastatic) and risk levels (high, intermediate, low, very-low) assigned on the basis of size and number of mitoses according to current National Institutes of Health recommendations. Primary end points were disease-free survival (DFS) and disease-specific survival (DSS).
Results
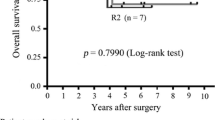
A total of 186 patients (97%) had c-kit–positive GIST. There were 54% high, 22% intermediate, 18% low, and 8% very low risk GIST originating from the stomach (54%), small bowel (36%), and colon and rectum (10%). Median patient age was 65 (range, 13–91) years, and 108 subjects (57%) were male. Seventy-two percent of patients had symptomatic local disease, and 21% patients had synchronous metastases. Most (95%) underwent R0 resections of their primary tumor. Among 146 patients (76%) with localized disease at presentation undergoing R0 resection, the 5-year DFS was 65%. High-risk GIST (HR 12, 95% CI, 5–32, P < .0001), symptomatic presentation (HR 2.5, 95% CI, 1.1–6, P = .04), and GIST in the small bowel (HR 2.8, 95% CI, 1–5, P = .003) were independently associated with decreased DFS. After a median follow-up of 63 months among survivors, the 5-year DSS was 68%. High-risk disease (HR 14.3, 95% CI, 5–41, P < .0001), symptomatic presentation (HR 3.1, 95% CI, 1.2–7.9, P = .02), and GIST in the small bowel (2.6,3 95% CI, 1–5, P = .006) were independently associated with decreased DSS.
Conclusions
High-risk GIST are associated with increased disease recurrence and decreased survival despite complete surgical resection. These patients should receive adjuvant therapy in the form of tyrosine kinase inhibitors.


Similar content being viewed by others

References
Gold JS, Dematteo RP. Combined surgical and molecular therapy: the gastrointestinal stromal tumor model. Ann Surg 2006;244:176–84
Verweij J, Casali PG, Zalcberg J, et al. Progression-free survival in gastrointestinal stromal tumours with high-dose imatinib: randomised trial. Lancet 2004;364(9440):1127–34
van Oosterom AT, Judson IR, Verweij J, et al. Update of phase I study of imatinib (STI571) in advanced soft tissue sarcomas and gastrointestinal stromal tumors: a report of the EORTC Soft Tissue and Bone Sarcoma Group. Eur J Cancer 2002;38(Suppl 5):S83–7
Joensuu H. Sunitinib for imatinib-resistant GIST. Lancet 2006;368(9544):1303–4
Demetri GD, van Oosterom AT, Garrett CR, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet 2006;368(9544):1329–38
Dematteo RP, Antonescu CR, Chadaram Y, et al. Adjuvant imatinib mesylate in patients with primary high risk gastrointestinal stromal tumor (GIST) following complete resection: safety results from the US Intergroup Phase II Trial ACOSOG Z9000 (abstract). Proc Am Soc Clin Oncol 2005:9009
DeMatteo RP, Lewis JJ, Leung D, et al. Two hundred gastrointestinal stromal tumors: recurrence patterns and prognostic factors for survival. Ann Surg 2000;231:51–8
Aparicio T, Boige V, Sabourin JC, et al. Prognostic factors after surgery of primary resectable gastrointestinal stromal tumours. Eur J Surg Oncol 2004;30:1098–103
Besana-Ciani I, Boni L, Dionigi G, et al. Outcome and long term results of surgical resection for gastrointestinal stromal tumors (GIST). Scand J Surg 2003;92:195–9
Bumming P, Ahlman H, Andersson J, et al. Population-based study of the diagnosis and treatment of gastrointestinal stromal tumours. Br J Surg 2006;93:836–43
Miettinen M, El-Rifai W, HL Sobin L, et al. Evaluation of malignancy and prognosis of gastrointestinal stromal tumors: a review. Hum Pathol 2002;33:478–83
Pierie JP, Choudry U, Muzikansky A, et al. The effect of surgery and grade on outcome of gastrointestinal stromal tumors. Arch Surg 2001;136:383–9
Fletcher CD, Berman JJ, Corless C, et al. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol 2002;33:459–65
Nilsson B, Bumming P, Meis-Kindblom JM, et al. Gastrointestinal stromal tumors: the incidence, prevalence, clinical course, and prognostication in the preimatinib mesylate era—a population-based study in western Sweden. Cancer 2005;103:821–9
Langer C, Gunawan B, Schuler P, et al. Prognostic factors influencing surgical management and outcome of gastrointestinal stromal tumours. Br J Surg 2003;90:332–9
Tran T, Davila JA, El-Serag HB. The epidemiology of malignant gastrointestinal stromal tumors: an analysis of 1,458 cases from 1992 to 2000. Am J Gastroenterol 2005;100:162–8
Pierie JP, Choudry U, Muzikansky A, et al. The effect of surgery and grade on outcome of gastrointestinal stromal tumors. Arch Surg 2001;136:383–9
Wu PC, Langerman A, Ryan CW, et al. Surgical treatment of gastrointestinal stromal tumors in the imatinib (STI-571) era. Surgery 2003;134:656–65
Miettinen M, Makhlouf H, Sobin LH, et al. Gastrointestinal stromal tumors of the jejunum and ileum: a clinicopathologic, immunohistochemical, and molecular genetic study of 906 cases before imatinib with long-term follow-up. Am J Surg Pathol 2006;30:477–89
Ruka W, Rutkowski P, Nowecki Z, et al. Other malignant neoplasms in patients with gastrointestinal stromal tumors (GIST). Med Sci Monitor 2004;10:LE13–4
Chacon M, Roca E, Barugel M, et al. Report of solid cancer in patients (pts) with gastrointestinal stromal tumours (GIST). J Clin Oncol 2004;22(14 Suppl):9065
Tryggvason G, Gislason HG, Magnusson MK, et al. Gastrointestinal stromal tumors in Iceland 1990–2003: the Icelandic GIST Study, a population-based incidence and pathologic risk stratification study. Int J Cancer 2005;117:289–93
Emory TS, Sobin LH, Lukes L, et al. Prognosis of gastrointestinal smooth-muscle (stromal) tumors: dependence on anatomic site. Am J Surg Pathol 1999;23:82–7
Miettinen M, Sobin LH, Sarlomo-Rikala M. Immunohistochemical spectrum of GISTs at different sites and their differential diagnosis with a reference to CD117 (KIT). Mod Pathol 2000;13:1134–42
Antonescu CR, Viale A, Sarran L, et al. Gene expression in gastrointestinal stromal tumors is distinguished by KIT genotype and anatomic site. Clin Cancer Res 2004;10:3282–90
Raut CP, Posner M, Desai J, et al. Surgical management of advanced gastrointestinal stromal tumors after treatment with targeted systemic therapy using kinase inhibitors. J Clin Oncol 2006;24:2325–31
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hassan, I., You, Y.N., Shyyan, R. et al. Surgically Managed Gastrointestinal Stromal Tumors: A Comparative and Prognostic Analysis. Ann Surg Oncol 15, 52–59 (2008). https://doi.org/10.1245/s10434-007-9633-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-007-9633-z