
Abstract
Background
Radical cholecystectomy is recommended for T2 gallbladder cancer. However, it is unclear whether hepatic resection is essential for peritoneal-side gallbladder cancer.
Methods
From January 2000 to December 2011, we identified T2 gallbladder cancer patients who had undergone curative intent surgery. A peritoneal-side tumor was defined when the epicenter of the tumor was located within the free peritoneal-side gallbladder mucosa. Hepatic-side gallbladder cancer was defined when the epicenter of the tumor was located within the gallbladder bed or neck.
Results
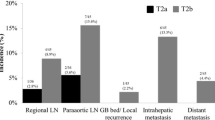
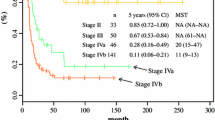
A total of 157 patients with T2 gallbladder cancer were included; 33 peritoneal-side and 124 hepatic-side tumors. In total, 122 patients underwent hepatic resection, whereas the remaining 35 patients did not. After a median follow-up period of 40 (range 5–170) months, the survival of the peritoneal-side group was better than that of the hepatic-side group (p = 0.002). In a multivariate analysis, tumor location, lymph node metastasis, hepatic resection, lymphatic invasion, and perineural invasion were significant prognostic factors (p = 0.045, p < 0.001, p = 0.003, p = 0.046, and p = 0.027, respectively). For the peritoneal-side group, there was no recurrence or death after cholecystectomy without hepatic resection. However, hepatic resection was an important factor associated with overall survival in patients with hepatic-side gallbladder cancer (p = 0.007).
Conclusions
In T2 gallbladder cancer patients, hepatic resection is recommended when there is tumor invasion of the gallbladder bed or neck. However, it is not always necessary in selected patients with peritoneal-side gallbladder cancer.


Similar content being viewed by others

References
You DD, Lee HG, Paik KY, Heo JS, Choi SH, Choi DW. What is an adequate extent of resection for T1 gallbladder cancers? Ann Surg. 2008;247:835-8.
Choi SB, Han HJ, Kim CY, et al. Surgical outcomes and prognostic factors for T2 gallbladder cancer following surgical resection. J Gastrointest Surg. 2010;14:668-78.
Dai M, Fong Y, Lowy A. Treatment of T3 gallbladder cancer. J Gastrointest Surg. 2009;13:2040-2.
Kohya N, Miyazaki K. Hepatectomy of segment 4a and 5 combined with extra-hepatic bile duct resection for T2 and T3 gallbladder carcinoma. J Surg Oncol. 2008;97:498-502.
Wise PE, Shi YY, Washington MK, et al. Radical resection improves survival for patients with pT2 gallbladder carcinoma. Am Surg. 2001;67:1041-7.
Schnelldorfer T, Sarr MG, Adams DB. What is the duct of Luschka? A systematic review. J Gastrointest Surg. 2012;16:656-62.
Shindoh J, de Aretxabala X, Aloia TA, et al. Tumor location is a strong predictor of tumor progression and survival in T2 gallbladder cancer: an international multicenter study. Ann Surg. 2014. doi:10.1097/SLA.0000000000000728.
Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC cancer staging manual, 7th edn. Springer, New York, 2010.
Foster JM, Hoshi H, Gibbs JF, et al. Gallbladder cancer: defining the indications for primary radical resection and radical re-resection. Ann Surg Oncol. 2007;14:833-40.
Angelsen JH, Horn A, Eide GE, Viste A. Surgery for colorectal liver metastases: the impact of resection margins on recurrence and overall survival. World J Surg Oncol. 2014;12:127.
Liu GJ, Li XH, Chen YX, Sun HD, Zhao GM, Hu SY. Radical lymph node dissection and assessment: Impact on gallbladder cancer prognosis. World J Gastroenterol. 2013;19:5150-8.
Harada K, Ochiai T, Inoue K, et al. Optimal surgical treatment for patients with pT2 gallbladder cancer. Hepatogastroenterology. 2011;58:14-9.
Gadzijev EM. Surgical anatomy of hepatoduodenal ligament and hepatic hilus. J Hepatobiliary Pancreat Surg. 2002;9:531-3.
Miyakawa S, Ishihara S, Horiguchi A, Takada T, Miyazaki M, Nagakawa T. Biliary tract cancer treatment: 5,584 results from the Biliary Tract Cancer Statistics Registry from 1998 to 2004 in Japan. J Hepatobiliary Pancreat Surg. 2009;16:1-7.
Kiran RP, Pokala N, Dudrick SJ. Incidence pattern and survival for gallbladder cancer over three decades–an analysis of 10301 patients. Ann Surg Oncol. 2007;14:827-32.
Ito H, Ito K, D’Angelica M, et al. Accurate staging for gallbladder cancer: implications for surgical therapy and pathological assessment. Ann Surg. 2011;254:320-5.
Shirai Y, Sakata J, Wakai T, Ohashi T, Ajioka Y, Hatakeyama K. Assessment of lymph node status in gallbladder cancer: location, number, or ratio of positive nodes. World J Surg Oncol. 2012;10:87.
Suzuki S, Yokoi Y, Kurachi K, et al. Appraisal of surgical treatment for pT2 gallbladder carcinomas. World J Surg. 2004;28:160-5.
Choi SB, Han HJ, Kim WB, Song TJ, Suh SO, Choi SY. Surgical strategy for T2 and T3 gallbladder cancer: is extrahepatic bile duct resection always necessary? Langenbecks Arch Surg. 2013;398:1137-44.
Wiggers JK, Koerkamp BG, Ovadia Z, Busch OR, Gouma DJ, van Gulik TM. Patterns of recurrence after resection of gallbladder cancer without routine extrahepatic bile duct resection. HPB (Oxford). 2014;16:635-40.
Hueman MT, Vollmer CM Jr, Pawlik TM. Evolving treatment strategies for gallbladder cancer. Ann Surg Oncol. 2009;16:2101-15.
Acknowledgment
There has been no grant support.
Disclosure
Huisong Lee, Dong Wook Choi, Jin Young Park, Sangmin Youn, Wooil Kwon, Jin Seok Heo, Seong Ho Choi, and Kee-Taek Jang have none to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lee, H., Choi, D.W., Park, J.Y. et al. Surgical Strategy for T2 Gallbladder Cancer According to Tumor Location. Ann Surg Oncol 22, 2779–2786 (2015). https://doi.org/10.1245/s10434-014-4300-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-014-4300-7