
Abstract
Background: There are many reports of disparities in health and medical care both between women and men and between various age groups. In most cases, men receive better treatment than women and young and middle-aged people are privileged compared with the old and the very old. Cardiovascular morbidity and diabetes mellitus are common, increase with age and are often treated extensively with drugs, many of which are known to have significant adverse effects.
Objective: The aim of the study was to analyse gender differences in the pharmacological treatment of cardiovascular disease and diabetes among very old people.
Methods: The study took the form of an epidemiological, cross-sectional survey. A structured interview was administered during one or more home visits, and data were further retrieved from medical charts and interviews with relatives, healthcare staff and other carers. Home-dwelling people as well as people living in institutional care in six municipalities in the county of Västerbotten, Sweden, in 2005–7 were included in the study. Half of all people aged 85 years, all of those aged 90 years and all of those aged ≥95 years living in the selected municipalities were selected for inclusion in the study. In total, 467 people were included in the present analysis. The main study outcome measures were medical diagnoses and drug use.
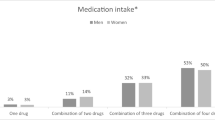
Results: In total, women were prescribed a larger number of drugs than men (mean 7.2 vs 5.4, p<0.001). Multiple logistic regression models adjusted for age and other background variables as well as relevant medical diagnoses (hypertension, heart failure) showed strong associations between female sex and prescriptions of thiazide diuretics (odds ratio [OR] 4.4; 95% CI 1.8, 10.8; p = 0.001), potassium-sparing diuretics (OR 3.5; 95% CI 1.4, 8.7; p = 0.006) and diuretics as a whole (OR 1.8; 95% CI 1.1, 2.9; p = 0.021). A similar model, adjusted for angina pectoris, showed that female sex was associated with prescription of short-acting nitroglycerin (OR 3.7; 95% CI 1.6, 8.9; p = 0.003). However, more men had been offered coronary artery surgery (p = 0.001). Of the participants diagnosed with diabetes, 55% of the women and 85% of the men used oral antihyperglycaemic drugs (p = 0.020), whereas no gender difference was seen in prescriptions of insulin.
Conclusions: Significant gender disparities in the prescription of several drugs, such as diuretics, nitroglycerin and oral antihyperglycaemic drugs, were observed in this study of very old people. In most cases, women were prescribed more drugs than men. Men more often had undergone coronary artery surgery. These disparities could only in part be explained by differences in diagnoses and symptoms.





Similar content being viewed by others


References
Swahn E. The care of patients with ischaemic heart disease from a gender perspective. Eur Heart J 1998; 19(12): 1758–65
Thorslund M, Lennartsson C, Parker MG, et al. Health status of the oldest old has changed for the worse: big differences between the sexes. Health of the women is worse than health of the men as illuminated by new data. Lakartidningen 2004; 101(17): 1494–9
Kosiak B, Sangl J, Correa-de-Araujo R. Quality of health care for older women: what do we know? Womens Health Issues 2006; 16(2): 89–99
Fremont AM, Correa-de-Araujo R, Hayes SN. Gender disparities in managed care: it’s time for action. Womens Health Issues 2007; 17(3): 116–9
Bramesfeld A, Grobe T, Schwartz FW. Who is treated, and how, for depression? An analysis of statutory health insurance data in Germany. Soc Psychiatry Psychiatr Epidemiol 2007; 42(9): 740–6
Bird CE, Rieker PP. Gender matters: an integrated model for understanding men’s and women’s health. Soc Sci Med 1999; 48(6): 745–55
Correa-De-Araujo R. Serious gaps: how the lack of sex/gender-based research impairs health. J Womens Health (Larchmt) 2006; 15(10): 1116–22
Le Couteur DG, Hilmer SN, Glasgow N, et al. Prescribing in older people. Aust Fam Physician 2004; 33(10): 777–81
Hamberg K. Gender bias in medicine. Womens Health (Lond Engl) 2008; 4(3): 237–43
Norris CM, Ghali WA, Galbraith PD, et al. Women with coronary artery disease report worse health-related quality of life outcomes compared to men. Health Qual Life Outcomes 2004; 2: 21
Anderson GD. Sex and racial differences in pharmacological response: where is the evidence? Pharmacogenetics, pharmacokinetics, and pharmacodynamics. J Womens Health (Larchmt) 2005; 14(1): 19–29
Franconi F, Brunelleschi S, Steardo L, et al. Gender differences in drug responses. Pharmacol Res 2007; 55(2): 81–95
Courtenay WH. Constructions of masculinity and their influence on men’s well-being: a theory of gender and health. Soc Sci Med 2000; 50(10): 1385–401
Klarin I, Fastbom J, Wimo A. A population-based study of drug use in the very old living in a rural district of Sweden, with focus on cardiovascular drug consumption: comparison with an urban cohort. Pharmacoepidemiol Drug Saf 2003; 12(8): 669–78
Noble RE. Drug therapy in the elderly. Metabolism 2003; 52 (10 Suppl. 2): 27–30
Hunter KF, Cyr D. Pharmacotherapeutics in older adults. J Wound Ostomy Continence Nurs 2006; 33(6): 630–6; quiz 37–8
McLachlan A, Hilmer S, Le Couteur D. Variability in response to medicines in older people: phenotypic and genotypic factors. Clin Pharmacol Ther 2009; 85(4): 431–3
Klarin I, Wimo A, Fastbom J. The association of inappropriate drug use with hospitalisation and mortality: a population-based study of the very old. Drugs Aging 2005; 22(1): 69–82
Fryckstedt J, Asker-Hagelberg C. Drug-related problems common in the emergency department of internal medicine: the cause of admission in almost every third patient according to quality follow-up. Lakartidningen 2008; 105(12-13): 894–8
Odar-Cederlof I, Oskarsson P, Ohlen G, et al. Adverse drug effect as cause of hospital admission. Common drugs are the major part according to the cross-sectional study. Lakartidningen 2008; 105(12-13): 890–3
Cumming RG, Le Couteur DG. Benzodiazepines and risk of hip fractures in older people: a review of the evidence. CNS Drugs 2003; 17(11): 825–37
Passarelli MC, Jacob-Filho W, Figueras A. Adverse drug reactions in an elderly hospitalised population: inappropriate prescription is a leading cause. Drugs Aging 2005; 22(9): 767–77
Wills P, Claesson CB, Fratiglioni L, et al. Drug use by demented and non-demented elderly people. Age Ageing 1997; 26(5): 383–91
Anthony M, Berg MJ. Biologic and molecular mechanisms for sex differences in pharmacokinetics, pharmacodynamics, and pharmacogenetics: part I. J Womens Health Gend Based Med 2002; 11(7): 601–15
Rademaker M. Do women have more adverse drug reactions? Am J Clin Dermatol 2001; 2(6): 349–51
Correa-de-Araujo R, Miller GE, Banthin JS, et al. Gender differences in drug use and expenditures in a privately insured population of older adults. J Womens Health (Larchmt) 2005; 14(1): 73–81
Pinquart M, Sorensen S. Gender differences in self-concept and psychological well-being in old age: a meta-analysis. J Gerontol B Psychol Sci Soc Sci 2001; 56(4): P195–213
Liang J, Bennett JM, Sugisawa H, et al. Gender differences in old age mortality: roles of health behavior and baseline health status. J Clin Epidemiol 2003; 56(6): 572–82
Rieker PP, Bird CE. Rethinking gender differences in health: why we need to integrate social and biological perspectives. J Gerontol B Psychol Sci Soc Sci 2005; 60 Spec. No. 2: 40–7
Hall-Lipsy EA, Chisholm-Burns MA. Pharmacotherapeutic disparities: racial, ethnic, and sex variations in medication treatment. Am J Health Syst Pharm 2010; 67(6): 462–8
SCB. Regional statistics. Stockholm: Statistiska centralbyrån (Statistics Sweden), 2006 [online]. Available from URL: http://www.ssd.scb.se/databaser/makro/start.asp?lang=2 [Accessed 2011 Jul 6]
Guigoz Y, Vellas B. The Mini Nutritional Assessment (MNA) for grading the nutritional state of elderly patients: presentation of the MNA, history and validation. Nestle Nutr Workshop Ser Clin Perform Programme 1999; 1: 3–11; discussion 11–2
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12(3): 189–98
Collin C, Wade DT, Davies S, et al. The Barthel ADL Index: a reliability study. Int Disabil Stud 1988; 10(2): 61–3
Almeida OP, Almeida SA. Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry 1999; 14(10): 858–65
Lawton MP. The Philadelphia Geriatric Center Morale Scale: a revision. J Gerontol 1975; 30(1): 85–9
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: American Psychiatric Association, 1994
Johnell K, Fastbom J, Rosen M, et al. Inappropriate drug use in the elderly: a nationwide register-based study. Ann Pharmacother 2007; 41(7): 1243–8
Mancia G, Laurent S, Agabiti-Rosei E, et al. Reappraisal of European guidelines on hypertension management: a European Society of Hypertension Task Force document. Blood Press 2009; 18(6): 308–47
Stromberg A, Martensson J. Gender differences in patients with heart failure. Eur J Cardiovasc Nurs 2003; 2(1): 7–18
Läkemedelsboken. Stockholm: Apoteket, 2009
Franklin SS, Gustin 4th W, Wong ND, et al. Hemodynamic patterns of age-related changes in blood pressure: the Framingham Heart Study. Circulation 1997; 96(1): 308–15
Basu R, Franzini L, Krueger PM, et al. Gender disparities in medical expenditures attributable to hypertension in the United States. Womens Health Issues 2010; 20(2): 114–25
Lloyd-Jones DM, Evans JC, Levy D. Hypertension in adults across the age spectrum: current outcomes and control in the community. JAMA 2005; 294(4): 466–72
Viigimaa M, Doumas M, Vlachopoulos C, et al. Hypertension and sexual dysfunction: time to act. J Hypertens 2011; 29(2): 403–7
Passare G, Viitanen M, Torring O, et al. Sodium and potassium disturbances in the elderly: prevalence and association with drug use. Clin Drug Investig 2004; 24(9): 535–44
Skoog I, Lernfelt B, Landahl S, et al. 15-year longitudinal study of blood pressure and dementia. Lancet 1996; 347(9009): 1141–5
Molander L, Gustafson Y, Lövheim H. Low blood pressure is associated with cognitive impairment in very old people. Dement Geriatr Cogn Disord 2010; 29(4): 335–41
Verghese J, Lipton RB, Hall CB, et al. Low blood pressure and the risk of dementia in very old individuals. Neurology 2003; 61(12): 1667–72
Molander L, Lövheim H, Norman T, et al. Lower systolic blood pressure is associated with greater mortality in people aged 85 and older. J Am Geriatr Soc 2008; 56(10): 1853–9
Banegas JR, Segura J, de la Sierra A, et al. Gender differences in office and ambulatory control of hypertension. Am J Med 2008; 121(12): 1078–84
Klarin I, Fastbom J, Wimo A. The use of angiotensin-converting enzyme inhibitors and other drugs with cardiovascular effects by non-demented and demented elderly with a clinical diagnosis of heart failure: a population-based study of the very old. Eur J Clin Pharmacol 2006; 62(7): 555–62
Williams D, Bennett K, Feely J. Evidence for an age and gender bias in the secondary prevention of ischaemic heart disease in primary care. Br J Clin Pharmacol 2003; 55(6): 604–8
Cross SE, Madson L. Models of the self: self-construals and gender. Psychol Bull 1997; 122(1): 5–37
Cannon PJ, Connell PA, Stockley IH, et al. Prevalence of angina as assessed by a survey of prescriptions for nitrates. Lancet 1988; 1(8592): 979–81
Acknowledgements
This study was supported by grants from the European Union Bothnia-Atlantica Program, the Vårdal Research Foundation, the King Gustav V’s and Queen Viktoria’s Foundation of Freemasons, the Umeå University Foundations for Medical Research, the Erik and Anne-Marie Detlof’s Foundation at Umeå University, the Swedish Dementia Association and Interreg IIIA Mitt-Skandia.
None of the funding sources had any financial interest in the study, and none of them were involved in the data collection or the analyses. The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brännström, J., Hamberg, K., Molander, L. et al. Gender Disparities in the Pharmacological Treatment of Cardiovascular Disease and Diabetes Mellitus in the Very Old. Drugs Aging 28, 993–1005 (2011). https://doi.org/10.2165/11594730-000000000-00000
Published:
Issue Date:
DOI: https://doi.org/10.2165/11594730-000000000-00000