
Abstract
Photoacoustic (PA) imaging requires channel data acquisition synchronized with a laser firing system. Unfortunately, the access to these channel data is only available on specialized research systems, and most clinical ultrasound scanners do not offer an interface to obtain this data. To broaden the impact of clinical PA imaging, we propose a vendor-independent PA imaging system utilizing ultrasound post-beamformed radio frequency (RF) data, which is readily accessible in some clinical scanners. In this paper, two PA beamforming algorithms that use the post-beamformed RF data as the input are introduced: inverse beamforming, and synthetic aperture (SA) based re-beamforming. Inverse beamforming recovers the channel data by taking into account the ultrasound beamforming delay function. The recovered channel data can then be used to reconstruct a PA image. SA based re-beamforming algorithm regards the defocused RF data as a set of pre-beamformed RF data received by virtual elements; an adaptive synthetic aperture beamforming algorithm is applied to refocus it. We demonstrated the concepts in simulation, and experimentally validated their applicability on a clinical ultrasound scanner using a pseudo-PA point source and in vivo data. Results indicate the full width at the half maximum (FWHM) of the point target using the proposed inverse beamforming and SA re-beamforming were 1.33 mm, and 1.08 mm, respectively. This is comparable to conventional delay-and-sum PA beamforming, for which the measured FWHM was 1.49 mm.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others

Keywords
- Photoacoustic (PA)
- Full Width At The Half Maximum (FWHM)
- Beamforming
- Clinical Ultrasound Scanner
- Delay Function
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Photoacoustic (PA) imaging is an emerging image modality that visualizes optical absorption property with acoustic penetration depth. PA imaging has a wide range of applications from small animals to human patients [1–3]. However, there are several factors that prevent PA imaging from being more widely used in clinical research and applications. The first limitation is the laser. Most of the laser systems used for PA imaging have high power and with low pulse repetition frequency (PRF). Those laser systems are expensive, bulky, and non-portable. Thus, a portable low cost laser system with sufficient power output such as a pulsed laser diode (PLD) is desired for easier access to PA data acquisition [4]. The second limitation is in PA signals receiving. PA signals contain broad-band spectral information, while conventional ultrasound (US) has a frequency window for reception [5]. Although a narrow-band probe cannot utilize the full potential of PA imaging, it still can receive signals, and is sometimes useful for collecting signals from deeper regions. The previous two limitations have been addressed or studied in the past research. The third limitation is the necessity of using channel data, which has not been well studied. PA reconstruction requires a delay function calculated based on the time-of-flight (TOF) from the PA source to the receiving probe element [6, 7], while US beamforming takes into account the round trip initiated from the transmitting and receiving probe element.
Thus, the reconstructed PA image with US beamformer would be defocused due to the incorrect delay function (Fig. 1a). Real-time channel data acquisition systems are only accessible from limited research platforms. Most of them are not FDA approved, which hinders the development of PA imaging in the clinical setting. Therefore, there is a strong demand to implement PA imaging on more widely used clinical machines. This third limitation motivated our research, whose goal is to investigate a vendor independent PA imaging system.

Conventional PA imaging system (a) and proposed PA imaging system using clinical US scanners (b). Channel data is necessary for PA beamforming because US beamformed PA data is defocused with the incorrect delay function. The proposed two approaches could overcome the problem.
To use clinical US systems for PA image formation, Harrison, and Zemp [8] proposed to change the speed of sound parameter. However, the access to the speed of sound parameter is uncommon, and the changeable range of this parameter is bounded. Zhang et al. [9] proposed to use US post-beamformed RF data with a fixed focal point. Our paper considers more general US beamformed data applied with delay-and-sum dynamic receive focusing. Two PA beamforming algorithms are introduced: inverse beamforming, and synthetic aperture (SA) based re-beamforming (Fig. 1). US beamforming is a sequential process scanning line by line. Using those sequentially beamformed data as input, inverse beamforming recovers channel data by taking into account the delay function used to construct US post-beamformed RF data. The recovered channel data can then be used to reconstruct a PA image. SA based re-beamforming algorithm regards the defocused RF data as a set of pre-beamformed RF data from virtual elements; an adaptive synthetic aperture beamforming algorithm is applied on the RF data to refocus it.
In this paper, we first introduce the theory behind the proposed PA reconstruction method. Afterwards, we present the evaluation of our method through simulation and experiments that validate its feasibility for practical implementation.
2 Methods
2.1 Approach I: Inverse Beamforming
The idea of inverse beamforming is based on three hypotheses; 1. Localizing an US point source does not require measuring its whole wavefront. 2. According to Huygens-Fresnel principle, a non-point source can be considered as a cloud of multiple point sub-sources. 3. Given the distribution, intensity and phase of the sub-sources, the pre-beamforming data can be derived using the previous two hypotheses.
According to Huygens-Fresnel principle, given any wavefront, each point on this wavefront is a sub-signal source. Thus, it is possible to reverse the beam propagation process, and reconstruct a map of the original signal source from beamformed RF data. In this specific case, each pixel on this image is considered as a sub-signal source. The value of the pixel represents the signal amplitude. Once the signal source map is derived, we can “fire” an US pulse from each pixel. By summing up all the time reversal wavefronts, and correcting the known distortion caused by the incorrect beamforming, the original channel data can be derived.
Figure 2 shows the three steps of the inverse beamforming method. The first step is to reconstruct the signal source map. Suppose at the beginning of the image frame t 0 , a laser pulse is sent to the field of view (FOV) and stimulates PA waves. The PA wave amplitude distribution at t 0 is I(x, y) under the continuous geometry (x, y). The US system receives the signal, performed the conventional pulse-echo beam forming, and output an incorrectly constructed image A(x m , y n ) under the discrete geometry (x m , y n ). If the FOV is quantized as an M by N grid, each cell can be viewed as a PA point sub-source, and the distribution I(x m , y n ) is the signal source map. The value of each cell I(x m , y n ) on the map indicates the sub-source intensity at that particular position. For each sub-source (x m , y n ), the intensity I(x m , y n ) is derived by integrating along the curve C 1 :

Illustration of inverse beamforming processes.
where S(x, y) is an amplitude correction factor to correct the wave intensity change caused by the distance. The signal source map can be formed by repeating the integration for all pixels. The second step is to mimic the PA data acquisition, and find the signal value of each sampling point on a pre-beamformed image. As shown in Fig. 2, at t 0 , the signal source map in FOV is I(x m , y n ), the PA waves from each sub-source propagate through the media, and reach the US probe array at the top of the image. At a given time t 1 , a particular array element at x m receives signal from a circle with a radius y, where y = C * (t 1 −t 0 ). For each pixel of the recovered channel data geometry P(x m , y n ), we integrate along the circle C2:
where P(x m , y n ) is the pixel amplitude received by the x m sample at time t 1 . The last step is to repeat step two for all pre-beamforming image sampling points, so a pre-beamformed image is reconstructed.
2.2 Approach II: Synthetic Aperture Based Re-Beamforming
The difference between US beamforming and PA beamforming is the TOF and accompanied delay function. US beamforming takes into account the TOF of the round trip of acoustic signals transmitted and received by the US probe elements (that is sent to and reflected from targets), while PA beamforming only counts a one way trip from the PA source to the US probe. Therefore, the PA signals under US beamforming is defocused due to an incorrect delay function (Fig. 3).

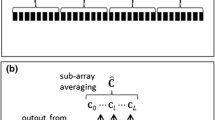
Illustration of synthetic aperture based re-beamforming processes.
The delay function in dynamically focused US beamforming takes into account the round trip between the transmitter and the reflecting point, thus the focus point at each depth becomes the half distance for that in PA beamforming. Thereby, it is possible to consider that there is a virtual point source, of which depth is dynamically varied in the axial dimension by a maximum value equal to half distance of the true focal point. The TOF from the virtual element to the receiving elements can be formulated as
where
2.3 Simulation and Experiment Setup
For the simulation, five point targets were placed at the depth of 10 mm to 50 mm with 10 mm intervals. A 0.3 mm pitch linear array transducer with 128 elements was designed to receive the PA signals. Delay-and-sum with dynamic receive focusing and an aperture size of 4.8 mm was used to beamform the simulated channel data assuming US delays.
The experiment was performed with a clinical US machine (Sonix Touch, Ultrasonix), which was used to display and save the received data. A 1 mm piezoelectric element was used to imitate a PA point source target. The element was attached to the tip of a needle and wired to an electric board controlling the voltage and transmission. The acoustic signal transmission is triggered by the line trigger sent from the clinical US machine. The US post-beamformed RF data with dynamic receive focusing was then saved. To validate the channel data recovery through inverse beamforming, the raw channel data was collected using a data acquisition device (DAQ). For in vivo mouse experiment, a tumor mimicking prostate cancer targeted by ICG was imaged using a 2 MHz center frequency convex probe.
3 Results
3.1 Simulation Analysis
The simulation results are shown in Fig. 4. The US beamformed RF data was defocused due to an incorrect delay function (Fig. 4b). The reconstructed PA images are shown in Figs. 4c–e. The proposed two approaches were compared to the ground truth conventional PA beamforming using channel data. The measured full width at the half maximum (FWHM) was shown in Table 1. The reconstructed point size was comparable to the point reconstructed using a 9.6 mm aperture on the conventional PA beamforming.

Simulation results. (a) Channel data. (b) US post-beamformed RF data. (c) Reconstructed PA image from channel data with an aperture size of 9.6 mm. (d) Reconstructed PA image through inverse beamforming. (e) Reconstructed PA image through SA re-beamforming.
3.2 Validation Using Pseudo-Photoacoustic Signal Source
US beamformed data was distorted due to incorrect delay (Fig. 5c), but both algorithms were applied on the RF data. Comparing the channel data recovered through inverse beamforming and the channel data from DAQ (Figs. 5a–b), identical wavefront was confirmed, while there were intensity differences due to different noise realization and recovery artifacts. However, this effect was negligible in the final PA image (Fig. 5e). The measured FWHM was also similar for both inverse beamforming and SA re-beamforming compared to the ground truth result using channel data (Table 2). This indicates the proposed methods could replace conventional PA beamforming using raw channel data.

Experiment results with Pseudo-PA data. (a–b) Comparison of channel data. (a) Reference channel data collected using DAQ. (b) Recovered channel data through inverse beamforming from US post-beamformed RF data. (c) US post-beamformed RF data collected from clinical US scanner. Reconstructed PA image using DAQ channel data (d), inverse beamforming (e), and SA re-beamforming (f).
3.3 In Vivo Prostate Cancer Visualization
The tumor mimicking prostate cancer could be visualized in both approaches (Fig. 6). The main contrast features were well captured in both methods, while the surrounding contrast varies due to different noise realization.

In vivo evaluation results. (a) Experiment setup. Contrast agents (ICG) targeting tumor are visualized. (b) PA image using channel data. (c) PA image through SA re-beamforming.
4 Discussion and Conclusion
Although demonstration of PA image formation was done based on point targets, the proposed algorithms would work for any structures that have high optical absorption such as a blood vessel that shows strong contrast for near-infrared wavelength light excitation. The algorithms could be also integrated into a real-time imaging system using clinical US machines [10].
A high PRF laser system can be considered as a system requirement, as it is necessary to synchronize the laser transmission to the US line transmission trigger. To keep the frame rate similar to that of conventional US B-mode imaging, the PRF of the laser transmission should be the same as the transmission rate, in the range of at least several kHz. Therefore, a high PRF laser system such as a laser diode is desirable. US transmission should be off or use low energy to eliminate the artifacts from US signals.
In this paper, we proposed a new paradigm on PA imaging using US post-beamformed RF data from clinical US systems. Two algorithms, inverse beamforming and SA based re-beamforming, were introduced and their performance was demonstrated in the simulation. In addition, experimental study using the pseudo-PA signal source and in vivo targets reveals the validity and clinical significance of these methods, in that a similar resolution was achieved compared to conventional PA imaging using channel data. Future work includes implementing the algorithm in a real-time environment.
References
Xu, M., Wang, L.V.: Photoacoustic imaging in biomedicine. Rev. Sci. Instrum. 77, 041101 (2006)
Wang, L.V., Hu, S.: Photoacoustic tomography. in vivo imaging from organelles to organs. Science 335, 1458–1462 (2012)
Kolkman, R.G.M., et al.: Real-time in vivo photoacoustic and ultrasound imaging. J. Biomed. Opt. 13(5), 050510 (2008)
Kolkman, R.G.M., et al.: In vivo photoacoustic imaging of blood vessels with a pulsed laser diode. Lasers Med. Sci. 21(3), 134–139 (2006)
Park, S., Aglyamov, S.R., Emelianov, S.: Beamforming for photoacoustic imaging using linear array transducer. In: Proceedings in IEEE International Ultrasonics Symposium, pp. 856–859 (2007)
Yin, B., et al.: Fast photoacoustic imaging system based on 320-element linear transducer array. Phys. Med. Biol. 49(7), 1339–1346 (2004)
Liao, C.K., et al.: Optoacoustic imaging with synthetic aperture focusing and coherence weighting. Opt. Lett. 29, 2506–2508 (2004)
Harrison, T., Zemp, R.J.: The applicability of ultrasound dynamic receive beamformers to photoacoustic imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 58(10), 2259–2263 (2011)
Zhang, H.K., et al.: Photoacoustic reconstruction using beamformed RF data: a synthetic aperture imaging approach. Proc. SPIE 9419, 94190L (2015)
Taruttis, A., Ntziachristos, V.: Advances in real-time multispectral optoacoustic imaging and its applications. Nat. Photonics 9(4), 219–227 (2015)
Acknowledgement
Authors acknowledge Howard Huang for proofreading, and Dr. Ying Chen for assisting in vivo experiment.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing AG
About this paper
Cite this paper
Zhang, H.K., Guo, X., Tavakoli, B., Boctor, E.M. (2016). Photoacoustic Imaging Paradigm Shift: Towards Using Vendor-Independent Ultrasound Scanners. In: Ourselin, S., Joskowicz, L., Sabuncu, M., Unal, G., Wells, W. (eds) Medical Image Computing and Computer-Assisted Intervention – MICCAI 2016. MICCAI 2016. Lecture Notes in Computer Science(), vol 9900. Springer, Cham. https://doi.org/10.1007/978-3-319-46720-7_68
Download citation
DOI: https://doi.org/10.1007/978-3-319-46720-7_68
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-46719-1
Online ISBN: 978-3-319-46720-7
eBook Packages: Computer ScienceComputer Science (R0)