
Abstract
Excessive growth hormone secretion will result in acromegaly affect metabolic function. Patients with acromegaly is 2–4 times greater risk of death than the normal. Early diagnosis is the key follow-up treatment of acromegaly. The clinical diagnosis is based on typical acromegaly the face and body features, endocrine and radiological. However, acromegaly diagnosis is still quite deferred. Typical acromegaly, with the symptoms and appearance, the physician can diagnose. Obvious early symptoms, diagnosis is not easy. As imaging technology advances, one after another to explore the diagnosis of acromegaly, however, did not the size of the stereoscopic 3D image. The aim of this study is to compare the compare the Receiver operating characteristic (ROC) and discriminant analysis for acromegaly detection by three dimensional facial measurements. To explore the difference of detection rate between the two analysis methods. The result shows that the accuracies of three categories from the univariate discriminant analysis, the lateral angles displayed the highest accuracy between all three categories in the female but the lowest rate for the ROC analysis. However, the lateral angles displayed the lowest accuracy between all three categories in the male and the lowest rate for the ROC analysis. The lateral angles, calculated from the two prominent variables, made a larger difference than the other two categories. From the result, it shows that the accuracy difference analysis between the two analysis methods in both genders. The difference could come from the different operation of the analysis methods. It could use the different analysis method to analyze the different facial dimensions for the acromegaly detection in the future and increase the accuracy for disease detection.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Acromegaly is a rare disease, with an estimated incidence of three to four cases per million population per year, and a prevalence of between 40 and 70 cases per million [1,2,3,4,5,6]. Excess growth hormone (GH) and the resultant elevations of insulin-like growth factor (IGF-I), the biochemical hallmarks of this disease [7, 8], produce its characteristic multisystem, often disfiguring, physical manifestations as well as its clinically significant comorbidities including diabetes mellitus (DM), hypertension (HTN), arthritis, sleep apnoea and cardiovascular disease [9,10,11,12,13,14]. The mortality is two to four times higher than the general population, and is predominantly due to vascular, metabolic, and pulmonary comorbidities [15,16,17]. The effectiveness of treating acromegaly patients, like many other diseases, is heavily dependent upon how early it is detected [18]. Therefore, early recognition is considered key to achieve a high rate of treatment success [10, 19] and avoiding long-term comorbidities. Increased awareness by healthcare professionals, especially primary care physicians, of acromegaly presentations is needed. Educational programs should be targeted at early recognition of acromegaly, with the hope that these will lead to earlier diagnosis. However, acromegaly has long been known for its insidious nature and long delay from onset of symptoms to diagnosis [20,21,22].
Although the mean age of disease occurrence is 32 years old, the mean age at diagnosis is 39–42 years old, and most series report a delay in the diagnosis of 7–10 years from the onset of signs and symptoms [23]. The clinical characteristics at diagnosis of patients with acromegaly did not change from 1981 to 2006, suggesting that clinical recognition of acromegaly has not significantly improved over the last 25 years. The reasons why acromegaly has traditionally been under-recognized are unclear, but could include its slowly progressive course allowing its changes to go un-noticed by the patient, family members or physicians, as well as the overlap of many of its comorbidities with common disorders. As effective therapies, can now prevent disease progression and return lifespan to normal, early recognition of acromegaly is essential [16, 24]. Recent developments including highly sensitive biochemical markers, both GH and IGF-I [25, 26], and MRI scans to identify small tumors are available for diagnosing acromegaly.
The most common problem leading to the diagnosis was acral changes (24%) [27]. And, in this photograph appeared recently in the New England Journal of Medicine as one of the journal’s periodic “Medical Mysteries” with the caption, “Which twin is the patient?” [28]. The changes of the face could be a key factor for acromegaly diagnosis. Previous studies have shown that face classification software using regular two-dimensional (2D) photographs allow distinguishing between different genetic syndromes [29,30,31]. And an attempt has been made to recognize acromegaly by a computer program using a morphable model that establishes a three-dimensional model from a regular 2D photograph [32]. Acromegaly can be detected by computer software using photographs of the face. Classification accuracy by software is higher than by medical experts or general internists, particularly in patients with mild features of acromegaly. It is a promising tool to help detecting acromegaly [33]. If a patient’s appearance suggests that he or she may have the disease, additional laboratory blood tests may be performed to confirm its presence or absence. Because these tests are expensive and time consuming, it would clearly be valuable to have an inexpensive and automatic prescreening method. Early detection is important in treating the disease successfully, but it is often missed because the signs are subtle and the condition is rare. Since many of the symptoms of the disease, such as swelling of the nose and growth of the jaw, affect facial appearance, the disease can be detected by experts (endocrinologists, for example) in many cases from a normal frontal photograph of a person.
However, identification methods and tracking facial changes in the early stages of acromegaly, by patients or family members, could be an important issue for promoting early disease diagnosis and treatment. The aim of this study is to compare the compare the Receiver operating characteristic (ROC) and discriminant analysis for acromegaly detection by three-dimensional facial measurements. To explore the difference of detection rate between the two analysis methods.
2 Methods
2.1 Samples
A group of patients with acromegaly was compared with a healthy control group. Eleven facial soft tissues measurements were collected. The study group consisted of 70 patients with acromegaly (35 females with ages ranging between 34–64 years with a mean age of 44.7 years; and 35 men aged between 28–67 years with a mean age of 43.5 years) who were admitted to the Chang Gung Memorial Hospital, Linkou, Taiwan between 2012 and 2014. All subjects participating in this cross-sectional study were Taiwanese and reside in the Taiwan. All patients with acromegaly were diagnosed on the basis of relevant clinical features including a mean GH level > 5 ng/mL, plasma IGF-I level greater than the average age/sex-matched levels, or a nadir GH > 1 ng/mL after a 75-gm oral glucose tolerance test (OGTT). And the control group comprised of 140 healthy adults (70 women with ages ranging between 28–41 years with a mean age of 30.5 years and 70 men with aged between 29–43 years with a mean age of 30.9 years). Controls were matched by gender to the acromegaly patient group at twice the sample size of those with the disease. Control subjects were volunteers from Chang Gung Memorial Hospitals.
2.2 3D Facial Measurements
All examinations were conducted using standardized protocols and trained staff gathered the data. Three-dimensional (3D) facial data was collected via a 3D camera system (LT3D FaceCam EXII) (Fig. 1).

3D face camera system and experiment space set-up
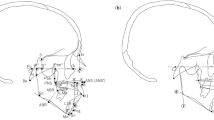
Participating subjects sat in front of a white background and 3D facial stereo photographs were taken with the subject’s head positioned in a cephalostand oriented on the Frankfort horizontal plane. Thirteen landmarks (Fig. 2) were digitalized. Eleven variables from the three categories were selected and applied, including five frontal widths, three lateral depths and three lateral angular measurements. All linear dimensions were measured from point-to-point (i.e., facial width -zy-zy). The angles measured were given in triple abbreviations (i.e., nasofrontal angle -g-n-prn). All measurements were collected and calculated by the one well-trained researcher.

Definition of thirteen landmarks and eleven dimensions
2.3 Statistical Analysis
The discriminant function equations were constructed in two ways by using each variable using univariate methods. All accuracies of discriminant equations were obtained by cross-validated classification. Receiver operating characteristic (ROC) curves were used to select the most sensitive and specific facial measurements (cutoff values) for detecting acromegaly. The statistical software packages used for this study were SPSS version 20 (SPSS Inc., Chicago, IL, USA).
3 Results and Discussion
Compare the average accuracy between both genders, higher accuracy for the discriminant analysis than the ROC analysis, besides the lateral view width. It shows that the difference accuracy between the two analysis methods. And the lateral view angle shows the lowest accuracy from the ROC in both genders.
The result in the Table 1 shows that the accuracies of three categories from the univariate discriminant analysis, the lateral angles displayed the highest accuracy between all three categories in the female but the lowest rate for the ROC analysis. However, the lateral angles displayed the lowest accuracy between all three categories in the male and the lowest rate for the ROC analysis. The lateral angles, calculated from the two prominent variables, made a larger difference than the other two categories. Furthermore, the angles could be calculated by the relative point-to-point from the 2D lateral image without the real dimensional measurements [34].
ROC graphs are a very useful tool for visualizing and evaluating classifiers. They are able to provide a richer measure of classification performance than scalar measures such as accuracy, error rate or error cost. [35]. An ROC curve is a two-dimensional depiction of classifier performance. To compare classifiers, we may want to reduce ROC performance to a single scalar value representing expected performance. A common method is to calculate the area under the ROC curve, abbreviated AUC. Since the AUC is a portion of the area of the unit square, its value will always be between 0 and 1.0. However, because random guessing produces the diagonal line between (0, 0) and (1, 1), which has an area of 0.5, no realistic classifier should have an AUC less than 0.5 [36].
When using normalized units, the area under the curve (often referred to as simply the AUC) is equal to the probability that a classifier will rank a randomly chosen positive instance higher than a randomly chosen negative one (assuming ‘positive’ ranks higher than ‘negative’). This can be seen as follows: the area under the curve is given by (the integral boundaries are reversed as large T has a lower value on the x-axis).

It can further be shown that the AUC is closely related to the Mann–Whitney U, which tests whether positives are ranked higher than negatives. It is also equivalent to the Wilcoxon test of ranks.

Linear discriminant analysis [37] is a well-known scheme for feature extraction and dimension reduction. For many applications, such as face recognition, all scatter matrices in question can be singular since the data is from a very high-dimensional space, and in general, the dimension exceeds the number of data points. This is known as the undersampled or singularity problem [38].
Compare the two analysis methods, discriminant analysis shows the more consistent accuracy than the ROC analysis in three measurement categories. For the gender comparison, shows the higher accuracy for the males than the females.
About the limitation of this study, facial appearance may vary from one ethnic population to another one. Therefore, the data obtained from a special population (Taiwanese) couldn’t be generalized. It could be the limitation that the standard cut-off measurements wouldn’t be possible for all ethnic populations. It will be an important issue to compare the acromegaly facial measurements for different ethnic populations in the future study (Fig. 3).

ROC curve for the lateral view angle (AUC: Females = 0.14; Males = 0.2)
4 Conclusion
From the result, it shows that the accuracy difference analysis between the two analysis methods in both genders. The difference could come from the different operation of the analysis methods. Linear discriminant analysis shows the consistent AUC from 67–78% for females, and 70–88% for males. ROC analysis shows the AUC from 14–70% for females, and 20–90% for males. It could use the different analysis method to analyze the different facial dimensions for the acromegaly detection in the future and increase the accuracy for disease detection.
References
Alexander, L., Appleton, D., Hall, R., Ross, W.M.: Epidemiology of acromegaly in the newcastle region. Clin. Endocrinol. (Oxf) 12(1), 71–79 (1980)
Bengtsson, B.A., Eden, S., Ernest, I., Oden, A.: Epidemiology and long term survival in acromegaly. Acta. Med. Scand. 223, 327–335 (1988)
Ritchie, C.M., Atkinson, A.B., Kennedy, A.L., et al.: Ascertainment and natural history of treated acromegaly in Northern Ireland. Ulster. Med. J. 59, 55–62 (1990)
Extabe, J., Gaztambide, S., Latorre, P., Vazquez, J.A.: Acromegaly: an epidemiological study. J. Endocrinol. Invest. 16(3), 181–187 (1993)
Holdaway, I.M., Rajasoorya, C.: Epidemiology of acromegaly. Pituitary 2(1), 29–41 (1999)
Daly, A.F., Petrossians, P., Beckers, A.: An overview of the epidemiology and genetics of acromegaly. J. Endocrinol. Invest. 28, 67–69 (2005)
Melmed, S.: Medical progress: acromegaly. N. Engl. J. Med. 355, 2558–2573 (2006)
Freda, P.U.: Current concepts in the biochemical assessment of the patient with acromegaly. Growth Horm. IGF Res. 13, 171–184 (2003)
Beauregard, C., Truong, U., Hardy, J., et al.: Long-term outcome and mortality after transsphenoidal adenomectomy for acromegaly. Clin. Endocrinol. (Oxf) 58, 86–91 (2003)
Mestron, A., Webb, S.M., Astorga, R., et al.: Epidemiology, clinical characteristics, outcome, morbidity and mortality in acromegaly based on the Spanish acromegaly registry. Eur. J. Endocrinol. 151, 439–446 (2004)
Swearingen, B., Barker, F.G., Katznelson, L., et al.: Longterm mortality after transsphenoidal surgery and adjunctive therapy for acromegaly. J. Clin. Endocrinol. Metab. 83, 3419–3426 (1998)
Ezzat, S., Strom, C., Melmed, S., et al.: Colon polyps in acromegaly. Ann. Internal Med. 114, 754–755 (1991)
Ron, E., Gridley, G., Hrubec, Z., et al.: Acromegaly and gastrointestinal cancer. Cancer 68, 1673–1677 (1991)
Colao, A., Vitale, G., Pivonello, R., et al.: The heart: an endorgan of GH action. Eur. J. Endocrinol. 151, 93–101 (2004)
Rajasoorya, C., Holdaway, I.M., Wrightson, P., et al.: Determinants of clinical outcome and survival in acromegaly. Clin. Endocrinol. 41, 95–102 (1994)
Bates, A.S., Van’t Hoff, W., Jones, J.M., et al.: An audit of outcome in acromegaly. Q. J. Med. 86, 293–299 (1993)
Colao, A., Cuocolo, A., Marzullo, P., et al.: Is the acromegalic cardiomyopathy reversible? Effect of 5-year normalization of growth hormone and insulinlike growth factor I levels on cardiac performance. J. Clin. Endocrinol. Metab. 86, 1551–1557 (2001)
Freda, P.U.: Advances in the diagnosis of acromegaly. Endocrinologist 10, 237–244 (2000)
Clemmons, D.R., Chihara, K., Freda, P.U., et al.: Optimizing control of acromegaly: integrating a growth hormone receptor antagonist into the treatment algorithm. J. Clin. Endocrinol. Metab. 88, 4759–4767 (2003)
Pearce, J.M.: Pituitary tumours and acromegaly (Pierre Marie’s disease). J. Neurol. Neurosurg. Psychiatry 73, 394 (2004)
Nabarro, J.D.: Acromegaly. Clin. Endocrinol. 26, 481–512 (1987)
Molitch, M.E.: Clinical manifestations of acromegaly. Endocrinol. Metab. Clin. North Am. 21, 597–614 (1994)
Nabarro, J.D.: Management of acromegaly. J. Clin. Pathol. 1, 62–67 (1976)
Kauppinen-Makelin, R., Sane, T., Reunanen, A., et al.: A nationwide survey of mortality in acromegaly. J. Clin. Endocrinol. Metab. 90, 4081–4086 (2005)
Freda, P.U., Post, K.D., Powell, J.S., et al.: Evaluation of disease status with sensitive measures of growth hormone secretion in 60 postoperative patients with acromegaly. J. Clin. Endocrinal. Metab. 83, 3808–3816 (1998)
Freda, P.U., Reyes, C.M., Nuruzzaman, A.T.: Basal and glucose-suppressed GH levels less than 1 μg/L in newly diagnosed acromegaly. Pituitary 6, 175–180 (2003)
Nachtigall, L., Delgado, A., Swearingen, B., et al.: Changing patterns in diagnosis and therapy of acromegaly over two decades. J. Clin. Endocrinol. Metab. 93, 2035–2041 (2008)
Nieuwlaat, W.A., Pieters, G.: A medical mystery– which twin is the patient? N. Engl. J. Med. 351, 68 (2004)
Loos, H.S., Wieczorek, D., Würtz, R.P., et al.: Computer-based recognition of dysmorphic faces. Eur. J. Hum. Genet. 11, 555–560 (2003)
Boehringer, S., Vollmar, T., Tasse, C., et al.: Syndrome identification based on 2D analysis software. Eur. J. Hum. Genet. 14, 1082–1089 (2006)
Vollmar, T., Maus, B., Wurtz, R.P., et al.: Impact of geometry and viewing angle on classification accuracy of 2D based analysis of dysmorphicfaces. Eur. J. Med. Genet. 51, 44–53 (2008)
Learned-Miller, E., Lu, Q., Paisley, A., Trainer, P., Blanz, V., Dedden, K., Miller, R.: Detecting acromegaly: screening for disease with a morphable model. In: Larsen, R., Nielsen, M., Sporring, J. (eds.) MICCAI 2006. LNCS, vol. 4191, pp. 495–503. Springer, Heidelberg (2006). doi:10.1007/11866763_61
Schneider, H.J., Kosilek, R.P., Günther, M., et al.: A novel approach to the detection of acromegaly: accuracy of diagnosis by automatic face classification. J. Clin. Endocrinol. Metab. 96, 2074–2080 (2006)
Bishara, S.E., Cummins, D.M., Jorgensen, G.J., Jakobsen, J.R., et al.: A computer assisted photogrammetric analysis of soft tissue changes after orthodontic treatment Part I: methodology and reliability. Am. J. Orthod. Dentofacial. Orthop. 107, 633–639 (1995)
Fawcett, T.: An introduction to ROC analysis. Pattern Recogn. Lett. 27(8), 861–874 (2006)
Hanley, J.A., McNeil, B.J.: The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 143, 29–36 (1982)
Fukunaga, K.: Introduction to Statistical Pattern Classification. Academic Press, San Diego (1990)
Krzanowski, W.J., Jonathan, P., McCarthy, W.V., Thomas, M.R.: Discriminant analysis with singular covariance matrices: methods and applications to spectroscopic data. Appl. Stat. 44, 101–115 (1995)
Acknowledgement
This project was funded by the Ministry of Science and Technology of the Republic of China, Taiwan, under grant no. (MOST 103-2221-E-182-050-MY3). The authors, therefore, acknowledge with thanks the Ministry of Science and Technology of the Republic of China for financial support.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this paper
Cite this paper
Wang, MH., Chen, BH., Chiou, WK. (2017). Compare the Receiver Operating Characteristic (ROC) and Linear Discriminant Analysis (LDA) for Acromegaly Detection by Three-Dimensional Facial Measurements. In: Duffy, V. (eds) Digital Human Modeling. Applications in Health, Safety, Ergonomics, and Risk Management: Health and Safety. DHM 2017. Lecture Notes in Computer Science(), vol 10287. Springer, Cham. https://doi.org/10.1007/978-3-319-58466-9_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-58466-9_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-58465-2
Online ISBN: 978-3-319-58466-9
eBook Packages: Computer ScienceComputer Science (R0)