
Abstract
A 23-year-old woman with no significant past medical history presented with fever every other day for 1 week. After graduating from college, she had spent a year as in Gabon, West Africa, before starting medical school. She was healthy until 1 week prior to presentation. At that time, she developed fever up to 102.5 °F, as well as chills and sweats, with symptoms occurring every other day. She also noted myalgia, headache, profuse sweats with defervescence of the fever, and intense fatigue.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


A 23-year-old female medical student presented with fever every other day for 1 week, which she believed was a cyclical fever highly suggestive of malaria . After graduating from college, she spent 1 year as a volunteer in Gabon, West Africa, before starting medical school. She had not traveled to a malaria-endemic area since leaving Gabon 13 months before.

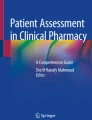
Plasmodium ovale on thin blood smear: large ring form with fimbriated red blood cell cytoplasm (a), amoeboid trophozoites (b), and schizont with brown pigment (c). Source: U.S. Centers for Disease Control and Prevention (CDC), DPDX Laboratory Identification of Parasites of Public Health Concern. https://www.cdc.gov/dpdx/resources/pdf/benchAids/malaria/Povale_benchaidV2.pdf (Accessed June 27, 2017)

Plasmodium vivax on thin blood smear: intracytoplasmic Schüffner’s dots; young ring forms are about one third of the diameter of an RBC; amoeboid trophozoites. Source: U.S. Centers for Disease Control and Prevention (CDC), http://phil.cdc.gov/phil_images/20021230/12/PHIL_2720_lores.jpg (Accessed June 27, 2017)
{kind=link}

Plasmodium falciparum on thin blood smear: (top) only delicate, young ring forms with small cytoplasm and 2 chromatin dots; very high parasitemia; multiply infected RBCs; accolé forms; no pigment; (bottom) banana-shaped gametocytes appear only about a week after the onset of illness, but may persist in asymptomatic persons (i.e., the human reservoir). Source: U.S. Centers for Disease Control and Prevention (CDC), DPDX Laboratory Identification of Parasites of Public Health Concern. https://www.cdc.gov/dpdx/resources/pdf/benchAids/malaria/Pfalciparum_benchaidV2.pdf (Accessed June 27, 2017)
She was healthy until 1 week prior to presentation, when she developed fever up to 102.5 °F, with chills and sweats. The symptoms only occurred every other day. Associated symptoms included myalgia, headache, profuse sweats with defervescence of the fever, and intense fatigue. She denied nasal or sinus congestion, sore throat, odynophagia, cough, chest pain, shortness of breath, abdominal pain, nausea, vomiting, diarrhea, dysuria, urinary frequency, or vaginal discharge. The patient’s past medical history was otherwise unremarkable.
During the year spent in Gabon, other than a few episodes of watery diarrhea, she did not develop any illness. She had not swum in freshwater (no risk of exposure to schistosomiasis), and she had taken weekly mefloquine malaria prophylaxis during her stay and until 4 weeks after returning to the United States (US). Since returning to the USA, she had remained in good health with no febrile illnesses. She was very active physically including running a few times a week. She had one sexual partner. She considered that they were in a monogamous relationship and were both at very low risk of HIV or other sexually transmitted infection (STI). She never had an STI herself and was followed regularly by a primary care physician who last did her cervical PAP smear about 3 months prior. She last had a negative HIV screening test 1 year prior to presentation.
She had never had a blood transfusion. She took no prescription drugs and was not taking a contraceptive pill. She had no drug allergies. The patient resided in Illinois and had traveled extensively within the USA including to the Upper Midwest and to New England. She reported never noting any tick bites. She had traveled abroad to the Caribbean, Israel, and Jordan, but she had not been in a malaria-endemic area since her stay in Gabon.
On physical examination, the patient was not in any acute distress. She was afebrile but stated that she had a fever to 102.5 °F the night before. Her blood pressure and pulse and respiratory rate were normal. Her conjunctivae appeared a bit pale but her sclerae were anicteric. She had no rash. The oral exam was normal, and she had no cervical or axillary lymphadenopathy. The heart rhythm was regular, without any murmur or abnormal sound. The lungs were clear to auscultation. The abdomen was soft and without hepatomegaly or splenomegaly. There was no suprapubic or costovertebral tenderness. A pelvic exam was unremarkable.
Laboratory tests were notable for hemoglobin 11.0 g/dL, white blood cell count 4000/μL (60% neutrophils, 30% lymphocytes, 8% monocytes, and 2% eosinophils), and platelet count 80,000/μL (normal range, 150,000–450,000/μL). Iron studies, liver enzymes, kidney function tests, and urinalysis were normal. Blood cultures were negative. A chest radiograph was normal.
The differential diagnosis was broad as it included infections acquired in the USA and abroad as well as a few noninfectious etiologies (see Table 1). However, because of the cyclical nature of her febrile illness, malaria was considered much more likely than other etiologies, although a cyclical fever is not pathognomonic of malaria. Thin and thick blood smears were obtained and reviewed carefully.
Thin blood smears showed intraerythrocytic plasmodia-like protozoa including ring forms, older trophozoites, and schizonts, with a parasitemia of about 2%. Older parasites had brown pigment. Infected red blood cells had intracytoplasmic dots and were enlarged, often with an oval shape. No gametocytes were identified but they may be difficult to recognize.
Babesiosis was ruled out due to the lack of tetrads, polymorphism, or vacuoles and the presence of brown pigment in older protozoa. Plasmodium falciparum malaria was also ruled out because in this infection only tiny, young ring forms with two dots of chromatin and a scant cytoplasm are identified on blood smear, with at times a few banana-shaped gametocytes [1]. Maturing P. falciparum induces the formation of knobs rich in P. falciparum erythrocyte membrane protein 1 (PfEMP-1) on the surface of red blood cells (RBC), with binding of PfEMP-1 to endothelial receptors on post-capillary venules, so that older parasites are trapped in the microcirculation [2,3,4].
Non-falciparum malaria was therefore diagnosed as all Plasmodium stages were identified, including young ring forms, older trophozoites, and schizonts. There are three non-falciparum plasmodia to consider. P. malariae can cause minimally symptomatic chronic malaria but is not common. In P. malariae infection, the parasitemia is very low, infected RBCs are of normal size, and typical trophozoites called band forms are recognized. P. vivax and P. ovale are quite similar on blood smears. In both of these, infected RBCs are enlarged, with the presence of intracytoplasmic Schüffner’s dots; young ring forms are large, about one third of the diameter of an RBC; and ameboid trophozoites are recognized. It is difficult to differentiate between the two species, but P. ovale tends to cause infected, enlarged RBCs to have an oval shape (see Table 46.2) [1,2,3,4].
Both P. vivax and P. ovale cause late relapses of malaria due to activation of dormant liver forms, called hypnozoites in the US literature. P. ovale is not as prevalent as P. vivax, except in Western Africa because local populations lack the Duffy blood type that is the major receptor for P. vivax entry into RBCs [2,3,4]. Our patient had therefore acquired P. ovale malaria in West Africa despite being on malaria prophylaxis there. She remained asymptomatic for more than a year when a hypnozoite activated and caused a relapse of malaria. The patient was treated for P. vivax malaria with chloroquine phosphate 1000 mg once, followed by 500 mg 6 h, 24 h, and 48 h later. Her glucose-6-phosphate dehydrogenase (G6PD) level was normal, allowing her physicians to prescribe safely primaquine 30 mg a day for 14 days to eradicate hypnozoites and to prevent further relapses of malaria [5].
46.1 Malaria
Female Anopheles mosquitoes transmit malaria at night, injecting sporozoa when they take a blood meal. Plasmodia are Apicomplexa, protozoa that use an apical complex of organelles and microtubules to penetrate into cells. Plasmodia infect hepatocytes (exoerythrocytic schizogony) first, then reach the blood, and infect RBCs (erythrocytic schizogony). There are four species of human plasmodia.
P. falciparum is highly lethal, causing about 95% of malaria-related mortality. Because the parasite infects all RBCs regardless of their age, it can cause very high parasitemia. Because it induces RBCs to grow PfEMP-1 knobs on their surface with resulting entrapment of the mature protozoa in the microcirculation, tissue injury is much more severe in falciparum malaria, with manifestations including cerebral malaria, placenta infection with adverse effects on pregnancy, and pulmonary edema or the acute respiratory distress syndrome (ARDS) [2,3,4]. Uncomplicated falciparum malaria manifestations include fever (every day initially, especially in travelers without prior semi-immunity; with prior semi-immunity, a fever every other day is often seen) and many associated symptoms (e.g., headache, nausea, vomiting, abdominal pain, and profuse sweats). The complete blood count usually shows anemia, thrombocytopenia, and a normal white blood cell count. Even uncomplicated falciparum malaria can progress rapidly to severe illness. P. falciparum can result in a large number of complications (see Table 46.3), and treatment is considered an emergency. Because P. falciparum has acquired drug resistance to multiple antimalarial agents, including chloroquine, sulfadoxine/pyrimethamine, mefloquine, quinine, and recently artemisinin derivatives, treatment always includes two different agents, and choice of therapy depends on the severity of illness. Acutely ill patients are best treated in the intensive care unit with rapidly acting intravenous agents, such as quinidine, quinine, or artesunate, plus a second active drug (doxycycline or clindamycin). Patients who are stable and can take oral therapy usually receive one of three combinations: atovaquone/proguanil, artemether/lumefantrine, or a combination of quinine plus either doxycycline or clindamycin [2,3,4,5].
P. vivax is highly prevalent, including previously in North America and Europe. It only infects young RBCs, resulting in lower parasitemia (1–2%). It requires the Duffy receptor on the surface of RBCs and therefore is rare in most of sub-Saharan Africa, although common in the horn of Africa and in Madagascar. Liver hypnozoites allow the parasite to survive cold winters. Chloroquine resistance has been described in Papua New Guinea and Indonesia. Patients present initially with daily fever and then get febrile paroxysms every 48 h (benign tertian fever). Splenic rupture is a rare complication.
P. ovale causes malaria that is clinically indistinguishable from P. vivax malaria and is also associated with late relapses due to the activation of hypnozoites. It is most prevalent in western Africa.
P. malariae is a minor species causing chronic malaria of low severity, as it only infects old cells with very low parasitemia. It may cause nephrotic syndrome due to chronic immune complexes [2,3,4].
P. knowlesi causes malaria in long-tailed and pig-tailed, crab-eating macaques found over a wide range of Southeast Asia from Myanmar to Timor. It causes zoonotic human malaria in Malaysia (especially Borneo), with cases reported elsewhere (Thailand, Myanmar, Singapore, and Philippines). Blood smears show tiny ring forms (like P. falciparum) and band forms (like P. malariae, with which it is confused). It results in a higher mortality than non-falciparum malaria, and chloroquine is an effective therapy [1,2,3,4,5].
Key Points/Pearls
-
P. falciparum smears only show young ring forms, but no mature trophozoites or schizonts because these are entrapped in the microcirculation.
-
Banana-shaped gametocytes are pathognomonic of P. falciparum, but are not seen in recently infected travelers; gametocytes appear late and are seen alone in non-ill persons in endemic areas.
-
Relapsing malaria only occurs with P. vivax and P. ovale; the term “relapse” in malaria has a specific meaning: the appearance of blood-stage parasites originating from a dormant liver stage of the parasite, called a hypnozoite .
-
Malaria relapses occur in 50% of persons infected with P. vivax or P. ovale, for up to 1–3 years after infection.
-
Only primaquine (30 mg base a day for 14 days) kills hypnozoites, but there is a risk of severe intravascular hemolysis in patients with G6PD deficiency.
-
Proper malaria prophylaxis in most areas is mefloquine taken weekly or either atovaquone/proguanil or doxycycline taken daily; malaria prophylaxis is continued after returning to a non-endemic area for 1 week with atovaquone/proguanil and for 4 weeks with either doxycycline or mefloquine.
References
U.S. Centers for Disease Control and Prevention (CDC), DPDX Laboratory Identification of Parasites of Public Health Concern. http://www.dpd.cdc.gov/dpdx/HTML/Babesiosis.htm. Accessed 27 June 2017.
Bennett JE, Dolin R, Blaser MJ. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. 8th ed. New York: Elsevier/Saunders; 2015.
Farrar J, Hotez PJ, Junghanss T, et al. Manson’s tropical infectious diseases. 23rd ed. New York: Elsevier/Saunders; 2013.
Guerrant RL, Walker DH, Weller PF. Tropical infectious diseases principles, pathogens & practice. 3rd ed. New York: Elsevier/Saunders; 2011.
CDC Guidelines for Treatment of Malaria in the United States. https://www.cdc.gov/malaria/resources/pdf/treatmenttable.pdf. Accessed 27 June 2017.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter
Cite this chapter
Benoit, JL. (2018). A Woman with a History of a 2-Year Stay in Gabon and Onset of a Cyclical Fever More Than 1 Year Later. In: David, M., Benoit, JL. (eds) The Infectious Disease Diagnosis. Springer, Cham. https://doi.org/10.1007/978-3-319-64906-1_46
Download citation
DOI: https://doi.org/10.1007/978-3-319-64906-1_46
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-64905-4
Online ISBN: 978-3-319-64906-1
eBook Packages: MedicineMedicine (R0)