
Abstract
We discuss a set of ongoing participatory design projects where participants are working to adapt a physiological monitoring prototype for use within the fire service. These projects include members of the fire service community, the director of a comprehensive firefighter medical and fitness program called the Firefighter Testing Program (FTP) located in the Human Performance Clinical Research Laboratory (HPCRL) at Colorado State University (CSU), a user-experience researcher, and a team of developers. The original AvidCor prototype (AC-1) is an affordable physiological monitor that pairs with a smartphone, allowing a user to independently record data about their electrocardiogram (EKG), pulse oximetry, and body temperature. The purpose of one of these participatory design projects is to identify barriers and envision opportunities where the AC-1 prototype and smart-phone app could be used to increase firefighters’ access to information and care that can be used to manage cardiovascular risk. Similarly, the purpose of the second project is to develop and test a second prototype, the AvidCor Fire-ground (AC-FG), capable of streaming real-time information about firefighters’ physiological performance which can enrich the types of decisions making processes that EMS professionals, firefighters, fire officers, and incident commanders engage in while operating within hazardous work environments.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Fire service organizations such as the National Fallen Firefighters Foundation (NFFF), the United States Fire Administration (USFA), International Association of Fire Chiefs (IAFC), International Association of Fire Fighters (IAFF), National Volunteer Fire Council (NVFC), and National Fire Protection Agency (NFPA) devote extensive resources to firefighter occupational safety and health programs (OSHPs). The NFFF, for instance, advances the Everyone Goes Home program, a set of 16 initiatives that promote life safety in the fire service [1]. Similarly, the NFPA promulgates industry standards, which include a set that address the design and implementation of occupational safety and health programs [2], comprehensive occupational medical programs [3], health-related fitness programs [4], and processes for firefighter rehabilitation during certain operations [5]. While NFPA 1500 deals broadly with OSHPs within the fire service, NFPA 1582, NFPA 1583, and NFPA 1584 focus on moments when physicians, health care providers, fitness professionals, emergency medical services (EMS) personnel, and fire officers evaluate whether prospective and current firefighters are medically or physically qualified for duty. If a cardiac dysrhythmia that only presents when a firefighter’s heart rate is elevated is not detected, a crew member could sustain a cardiac injury while performing operations on a fire-ground. If symptoms of cardiac disease are left undiagnosed or unexplained, opportunities for a firefighter to develop plans for managing or ameliorating those symptoms are lost. If a firefighter begins an exercise regimen without the support of fitness professionals, s/he might practice those activities in ways that cause or exacerbate injuries. If an incident manager initiates a rehab process during a structure fire, but a line officer tells a crew that they can return to work without having their vital signs checked by EMS personnel, a firefighter exhibiting symptoms of hydrogen cyanide poisoning could collapse on scene. These examples not only emphasize the critical role that information plays within firefighter comprehensive medical and fitness programs (CMFPs), but also illuminate how user experience (UX) research can be used to improve firefighters’ interactions with and access to the types of care and information offered within such programs.
One comprehensive firefighter health and fitness program is the Firefighter Testing Program (FTP) housed within the Human Performance Clinical Research Laboratory (HPCRL) at Colorado State University (CSU). As a longstanding CMFP that has been in existence for over ten years, the FTP has served over 2,000 Coloradan firefighters affiliated with 30 participating agencies. Like other firefighter medical and fitness programs, the FTP seeks to identify behavioral and physiological health risks in firefighters. Yet, the FTP is distinctive because it utilizes a literate care model where firefighters are provided with information and support to develop actionable, evidence-based plans for self-managing their health, fitness, and wellness [6,7,8]. Recent studies have demonstrated that participating in CMFPs like the FTP has a variety of positive benefits that range from reduced injury rates and early detection of treatable diseases to extended career longevity and increased awareness of the ways dietary, exercise, and lifestyle choices impact a firefighter’s health and fitness [9,10,11]. Unfortunately, compliance with NFPA standards is voluntary, and 60-70% of U.S. firefighters do not participate in a comprehensive medical and fitness program [12]. Moreover, little is known about the degree to which existing CMFPs conform to NFPA standards, and CMFPs are only one context when firefighters might benefit from access to health and fitness information that enriches decision making about the ways firefighters practice work. Put simply, one strategy that fire service leaders could leverage to improve firefighter occupational health and safety outcomes is increasing firefighters’ access to the types of care and information that are offered within CMFPs such as the FTP.
In this paper, we sketch a set of ongoing participatory design projects where members of the fire service community, the director of the FTP, a UX researcher, and a team of developers are working to adapt a physiological monitoring platform for use within the fire service. The original platform, designed by a team of developers at AvidCor, consists of a physiological monitoring prototype (AC-1) that uses Bluetooth to pair with a smartphone and allows a user to independently record data about their electrocardiograms (EKGs), pulse oximetry, and body temperature. We begin by providing background on the ways socioeconomic factors influence occupational safety and health outcomes in the fire service and discuss concepts that influence our approach to occupational safety and health research. Next, we trace the genesis of our collaborative work within a larger transdisciplinary research team and sketch how the values, tools, and practices we have adapted from community-based research and participatory design methodologies inflect our stance as researchers [13]. We then turn toward a detailed discussion of two ongoing participatory design projects. While the purpose of the first project is to identify barriers and envision opportunities where the AC-1 prototype and smart-phone app could be used to facilitate increased firefighter access to information and care that can be used to manage cardiovascular risk, the purpose of the second project is to develop a second prototype, the AvidCor Fire-ground (AC-FG), which could stream real-time information about individual firefighters’ physiological performance while they are working in arduous environments to EMS professionals, firefighters, fire officers, and incident commanders. We conclude by considering the implications our ongoing work may have for other UX researchers who are working to improve systems where stakeholders offer and receive medical information and care.
2 Background
2.1 Socioeconomic Status and Occupational Safety and Health in Blue-Collar Industries
Research has demonstrated that a worker’s occupational class and socioeconomic status (SES) directly corresponds to rates in morbidity and mortality [14,15,16]. “Lower-status jobs,” Adler and Newman note, “expose workers to both physical and psychosocial risks” and “carry a higher risk of occupational injury and exposure to toxic substances” [14]. Like other blue-collar workers, firefighters are more likely to sustain injuries than individuals working in white-collar occupations. However, firefighting ranks among those occupations with the very highest rates of workplace injury, including injuries that result in lost-time [15,16,17,18,19,21].
CMFPs are an invaluable tool within firefighting OSHPs, then, because they provide stakeholders with information and care that can be used to make decisions about how, when, and why different individuals within fire service organizations perform certain types of work. Research indicates that firefighters are twice as likely to sustain a fatal cardiac injury than fellow Americans [22], and appear to develop certain types of cancer at higher rates [22, 23]. The diagnostic tests that are performed within CMFPs are especially critical because they are one of the few moments when firefighters have opportunities to identify medical and health conditions such as cardiac dysrhythmias or heart disease that can be treated before they manifest as injuries or fatalities within operational contexts.
Over the past decade, an annual average of 71,000 firefighters have sustained injuries on duty [24]. It appears that the growing emphasis that national and international fire service organizations have placed on CMFP participation could be having positive effects, as longitudinal data surrounding safety and health outcomes in the U.S. fire service indicates that the overall number of injuries has been declining [24]. However, NFPA researchers also caution that the rate of injury per incident has remained relatively constant over the same period of time [24]. In other words, there has been a significant decrease in the cumulative total of injuries and fires that occur each year, but the rate of injury per incident appears to be relatively static. While the human costs associated with firefighter injury and fatality are inexpressible, the National Institute for Standards and Technology (NIST) estimates the annual economic impact of firefighter injuries in the U.S. is between $2.8 and $7.8 billion [25]. UX research could be used to better understand how factors such as affordability, culture, and access influence participation rates within firefighter CMFPs. UX research can help identify and improve moments when firefighters experience health and fitness care. UX research can help improve the design of interactions between firefighters and health care providers following a literate care model that seeks to provide the types of care, information, and support that empowers these workers to develop realistic plans for managing their health and wellness [8]. UX research, in short, could improve access to the types of care and information that have far-reaching impacts for firefighters, families, fire service organizations, and communities.
2.2 Firefighter Occupational Safety and Health Outcomes: An Adaptive Challenge
Our perspectives toward firefighter occupational safety and health are not only inflected by the research we conduct as part of larger transdisciplinary team, but also our past experiences as practitioners within fire and EMS organizations. We understand that occupational safety and health outcomes in the fire service are directly tied to cardiovascular risk and health. The leading cause of firefighter fatality has been, and continues to be, sudden cardiac death [26]. However, causality is easily complicated when researchers look at the events and confluence of factors that precede a firefighter injury or fatality. NIOSH, for instance, frequently identifies issues in communication, incident management, decision making, risk perception, and situational awareness as contributing factors in investigations of incidents where firefighters sustain fatal or serious injuries [27,28,29]. In an analysis of over 2,000 incidents, a former assistant chief from Indianapolis Fire Department, found that maydays were more likely to be called when crews were working independently from their supervising officer [30]. Moreover, Smith and colleagues conducted a study at a live-fire training facility where they observed that “psychological and psychological strain…has the potential to impair cognitive function” [31]. Still, there is much unknown about the ways physiological variables relate to cognitive and operational performance during specific firefighting activities. Put simply, while we suspect CMFPs have an important and central role within OSHPs, we want to acknowledge that a firefighter’s health and fitness is not the sole factor influencing occupational safety and health outcomes in the industry.
Instead, we see occupational safety and health outcomes as an adaptive challenge. According to Heifetz & Laurie technical problems can be solved by individuals or teams who possess specialized forms of expertise, whereas adaptive challenges require stakeholders “to clarify values, develop new strategies, and learn new ways of operating” [32]. Treating firefighter occupational safety and health as an adaptive challenge is a useful approach from our perspective, because it requires researchers, stakeholders, and designers to account for the broader contexts, actors, and factors that surround firefighting. As noted above, whether individuals perform blue- or white-collar work will impact their rates of exposure to workplace hazards which, in turn, influence health and safety outcomes. However, socioeconomic factors also color the types of decisions that fire service leaders and health care providers must make when determining who is medically and physically qualified for duty. Indeed, 800,000 of the 1.1 million firefighters who serve communities in the U.S. work in volunteer fire departments [33]. These types of departments often serve communities that are economically disadvantaged and under resourced. While it is entirely sensible for national or international fire service organizations to devote resources toward prompting OSPH in the industry, it is also sensible that leaders of organizations located in communities where it is difficult to recruit and retain volunteers to resist these efforts, as CMFPs could reveal medical conditions that disqualify existing or prospective members. That is, we think that NFPA 1582 compliant CMFPs employing literate care models could be consistent with the types of stance that are necessary for engendering change in some organizations, but other organizations encounter different barriers which will require stakeholders to envision models of care that are sensitive to types of challenges and tensions that are currently impacting firefighters’ participation rates in NFPA 1582 compliant CMFPs.
3 Methodology
3.1 Transdisciplinary, Community-Based Research (CBR)
For over three years, we have been part of a larger transdisciplinary research collaborative that has been working together toward the broad goal of improving firefighter safety and health outcomes in the fire service. Transdisciplinary approaches to team science, as Moldenhauer and Johnson Sackey describe, are particularly suited for addressing adaptive challenges “that can only be tackled with researchers from a variety of disciplines from the sciences and humanities who are willing to create new ways to work together” [34]. Like Moldenhauer and Johnson Sackey, our approach to transdisciplinary research is also inflected by community-based research (CBR) and participatory design (PD) methodologies [13, 34,35,36,37]. While there is significant variance within and between these methodological traditions, Grabill observes, each “draw on the practice of working with people to answer questions and solve problems—as opposed to researching ‘on’ people and their problems” [13]. Following these researchers, we seek to enact research through practices where we identify and seek to respond to challenges alongside members of the fire service community. As researchers who also identify as practitioners—Tiffany was a medic and Tim was a firefighter and technical rescuer—participation takes on an added dimension of critical importance because it allows us to complicate and enrich our individual experiences and histories in fire and emergency medical services. Moreover, our connections to this community means that the types of “relationship building and maintenance” practices which are so vital for CBR and PD projects [13] are practices that we regularly engage in. Just as Tiffany interacts frequently with members of the fire service, Tim often spends time catching up with firefighters who he’s previously worked with as either a firefighter, fire instructor, or researcher. Above and beyond the daily activity associated with directing the FTP, Tiffany also works with fire service leaders to help them align department policies with NFPA standards on occupational safety and health. Similarly, Tim has been mentoring a fire chief in the region who is designing a research project to earn an executive fire officer credential from the National Fire Academy.
3.2 Participatory Design (PD)
Like CBR, PD “emphasizes co-research and co-design: researcher-designers must come to conclusions in conjunction with users” [36]. PD has been especially useful within the projects that we are involved in because it offers a framework for “alternating between practical work to support changes…and systematic data collection and analysis” [36]. According to Spinuzzi, PD involves three stages where “researcher-designers” employ various methods to envision and realize change by setting objectives for a project, collecting and analyzing data about an organization, and designing or testing prototypes that might be used to ameliorate work conditions or processes, and evaluating the designs (see Table 1) [36].
In the following section, we use Spinuzzi’s stages of participatory design as a heuristic for discussing how participatory design activities that our collaborative has previously participated inform and facilitate the research and design work that we are currently engaged in with fire service stakeholders. The aims of this work are to explore how the AC-1 and AC-FG physiological prototypes might fit into the fire service and to adapt the prototypes accordingly.
4 Iterating Designs to Increase Firefighter Access to Health and Fitness Information
4.1 Initial Exploration of Work
Our team possess deep knowledge of the ways the fire service operates, including the ways that firefighters experience work differently based on jurisdictional, geographic, and organizational factors. Still, we have taken steps to explore work processes and technologies associated with CMPHs with fresh eyes. For example, our team organized and co-hosted Adaptive Challenges, a one-day symposium with leaders from the Poudre Fire Authority, to co-construct shared understanding of the factors that influence firefighter safety and health outcomes. We brought in four speakers, Chief Tom DeMint (PFA), Division Chief Scott Heiss (Denver Fire Department), Dr. Ron Timmons (University of North Texas), and Dr. Bill Hart-Davidson (Michigan State University) to speak on issues that range from wearable-technologies and automation to communications, risk perception, and cultures of risk within the fire service. 70 fire service leaders participated, including fire officers responsible for overseeing firefighting training, safety and/or health programs at over distinct 25 fire department and representatives from fire service organizations such as the NVFC, NFFF, IAFC, IAFF, International Association of Black Professional Firefighters, International Association of Women in Fire and Emergency Services, Front Range Fire Consortium, Colorado Division of Fire Prevention and Control, and the Colorado Fire and Police Pension Association. During breakout sessions at the symposium, participants spent time rotating through stations focused on topics that influence occupational safety and health outcomes such as blue-collar identity, firefighter education and training, access to CMFPs and mental health care, and emergent technologies. Members of our research team facilitated discussion and recorded notes, as participants envisioned solutions and discussed barriers.
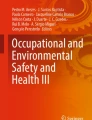
After the symposium, we developed activity system diagrams [37] of OSHPs (see Fig. 1) and mapped out contexts when firefighters might receive feedback about their health or fitness according to NFPA standards (see Fig. 2). These analytical tools allow researcher-designers to visualize how components of CMFPs might fit might within a local OSHP and identify moments when increasing access to the types of information and care provided within CMFPs could enrich decision making processes. For instance, NFPA 1584 calls on organizational managers to enact firefighter rehabilitation processes during operations and trainings that pose an increased risk to personnel. The standard protocols state that after firefighters have performed work for an extended period of time, they should have their vitals evaluated by EMS personnel before they return to work. In practice, however, there are incidents where rehabilitation processes are rarely, if ever, enacted, which mark missed opportunities for personnel to receive timely care or feedback regarding their health and/or fitness. Firefighters exhibiting symptoms of hydrogen cyanide poisoning at a structure fire, for instance, could miss an opportunity to receive care that is essential for managing those exposures.

Activity system diagram of firefighter occupational safety and health programs

Contexts when firefighters might receive feedback about their health and fitness
Moreover, these tools enable researcher-designers to approach CMFPs as systems that are enacted through situated practices and identify elements or stakeholders that might be overlooked within them. For example, mental health care providers are often not discussed as stakeholders who could play important roles with OSHPs and CMFPs. By mapping these systems, researcher-designers illuminate moments and locations within these systems when firefighters, line officers, executive fire officers and care providers might benefit by receiving the types of care and information necessary for maintaining fitness or developing health intervention strategies.
4.2 Discovery Processes
The primary aim of the Adaptive Challenge symposium was to bring stakeholders from the industry together to envision solutions to occupational safety and health challenges they face today. One particular tension that we hoped to investigate with stakeholders was how emerging technologies like automation, physiological wearables, augmented and virtual reality, and the internet of things might fit into a profession with deeply held blue-collar traditions and cultures. For instance, during breakout sessions, stakeholders participated in focus groups which explored trends in fitness and health and discussed ways that they thought physiological monitoring devices might be integrated within various work activities. However, stakeholders also articulated factors that could influence whether firefighters are likely to adopt or embrace these tools in work practices and sketched examples of problematic ways that the tools could be used to surveil workers or compromise private medical information.
While our collaborative has since built on the foundational work that occurred during the symposium, a particularly serendipitous outcome is that we were introduced to a team of designers who had developed an affordable physiological monitoring platform. The AvidCor team was interested in exploring whether the platform could be viably adapted for use in the fire service; and, we were interested in the platform because we had unable to locate an affordable technology that would enable us to collect data about firefighters’ physiological performance in actual work environments. The absence of such a device was a barrier that has impeded our ability to better understand the links that might exist between physiological, communicative, and operational performance.
To further explore if and how a device like the AvidCor monitor might fit within the fire service, we continued the process of participatory discovery by pursuing a collaborative research and writing project [38]. During the project, we conducted a review of literature related to emerging wearable technologies in the fire service and composed two case studies of moments when (what had once been) two new wearable technologies—self-contained breathing apparatus (air tanks) and heat resistant hoods—had been introduced to the industry. This inquiry enabled our team to better appreciate how introducing new tools to the industry can impact the work that firefighters perform in unanticipated ways. Thereafter, we used the case studies to facilitate open-ended conversations to explore how firefighter physiological monitoring platforms might be used in the future and identify barriers that designers and users will need to consider if they are going to avoid the types of unintended consequences that have accompanied the introduction of new protective designs in the past.
4.3 Prototyping
Having developed a broad sense of how physiological wearables could be integrated in the fire service, our team of researcher-designers has since moved on toward prototyping and usability testing. This stage connects back directly to work we have performed during earlier stages, as we have identified a number of contexts (see Fig. 2) where we believe the prototype could be adapted to enrich firefighters’ access to feedback about their health and fitness.
Rurally and Geographically Remote Communities (AV-1).
Many of the fire departments located outside of the I-25 and I-70 corridors of Colorado—identified as rural and geographically remote communities—do not participate in the FTP. We suspect that the AC-1 could be used to increase these firefighters’ access cardiac monitoring, because using the device is fairly simple and provides a reliable means for gathering data about an individual’s health (e.g., EKG; oxygen saturation; heart rate and rhythm) that can be signs of heart disease or life-threatening dysrhythmia. The smart-phone app enables individuals to share the tracing with a care provider s/he trusts and, if the tracing indicates any abnormalities, sends an alert message that the user should seek medical care. To further explore if the AC-1 exists as a viable prototype, we are working with firefighters to investigate how the existing hardware, software, and documentation can be redesigned to facilitate usability. To perform this design-research, we have partnered with three fire departments located in three rurally or geographically remote areas of the state. At each department, we have recruited or seek to recruit 7-20 participants to complete a series of tasks where they set up the device, place electrodes on their body, pair the monitor with an app, and follow the user documentation to acquire an EKG tracing. As firefighters attempt to take a tracing, researcher-designers observe and note moments when the individuals completing the task appear to struggle with the app, hardware, or documentation.
Thereafter, we recruit 4–7 of the phase-one participants to provide feedback on the design of the AC-1 platform and offer feedback on barriers to its use in the fire service during focus group interviews that span 30–45 min. There are two prompts that participants respond to during a focus group interview. The first prompt asks participants to share feedback on their experiences using the hardware, app, or documentation and to offer solutions that would improve the design of platform components. The second prompt asks participants to consider socioeconomic and cultural factors that could impact whether firefighters in a department located in a community similar to their own might be reluctant to participate in CMFPs or use a platform like the AC-1. In order to encourage co-research and co-design, the focus group facilitator encourages firefighters to forward follow-up questions to one another, to collaboratively envision solutions to the types of barriers they have identified, and to expand on points that other participants have forwarded during previous points in the discussion.
Real-Time Physiological Monitoring of Personnel in Work Environments, Including Firefighter Rehabilitation Processes (AV-FG).
One of the major factors that we suspect impacts occupational safety and health outcomes in the fire service is that information and data that provides feedback about a firefighter’s health or fitness is sporadic. In some departments, firefighter candidates participate in an agility test and complete a physical—that may or may not be rise to the standard of care outlined in NFPA 1582—before they are officially hired. However, they might never be required to complete a physical or participate in an agility test again by their department. Thus, NFPA 1584 has been an invaluable tool for some jurisdictions, because it has enabled incident commanders to ensure that personnel who have been working for extended periods of time are evaluated by EMS personnel before returning to work during high risk incidents or trainings. While all incidents or trainings in the fire service carry some degree of risk, extended and high-risk operations inherently increase the likelihood of sudden cardiac events because firefighters often work up to and beyond their cardiovascular threshold.
Developing technologies that provide real-time physiological monitoring could have a powerful impact on occupational safety and health outcomes in the industry because the tools could provide incident commanders, fire officers, firefighters, and EMS with opportunities for the early identification of medical problems or emergencies, which may happen at any time. The data and information that these tools provide could not only be used to intervene if a firefighter or crew is under extreme physiological duress during firefighting or rescue operations, but could also engender firefighters, officers, and incident commanders to develop “data-driven science-based tactics” that reduce or lessen firefighters’ exposure to extreme physiological- and heat-stress [39]. Predicting when a life-threatening event could occur is, of course, challenging in a high-risk mission-oriented profession like firefighting, but developing tools that facilitate continuous real-time physiological monitoring could eliminate the perception that cardiac events can only happen in high risk environments. That is, these tools might engender opportunities for passively monitoring a firefighters’ physiological performance throughout their duty tours rather than sporadically enacting active surveillance as part of firefighter rehabilitation processes during high risk incidents and trainings.
To further explore how a device like the AV-FG might fit within the fire service, we are currently in the process of rapidly iterating prototypes and performing usability testing at the HPCRL. AvidCor developers have designed a prototype that uses two-leads to take an EKG tracing. During the first phase of usability testing, 30 firefighters visiting the FTP as part of periodic screening are being recruited. While participants complete a maximal treadmill protocol wearing the 12-lead gold-standard that is part of the regular screening test at the FTP, they also don two additional leads and a small puck-like device. EKG tracings are taken and compared. Comparative analysis of the 12-lead and 2-lead EKGs tracings gathered during the first 15 usability tests conducted by an AvidCor cardiologist suggested that the device is taking accurate measurements of heart rate and rhythm. During usability tests, clinicians also take notes of the technical difficulties they encounter while operating the platform and communicate them to one of the project managers responsible for passing information to developers. Currently, the developers are addressing technical issues that clinicians have identified before a second sequence of 15 usability tests is performed. Plans for field testing the device are in place, where we will iterate back through the discovery process and prototyping stages of participatory design using observational methods and focus groups.
Clinical Settings for Performing CMFP Evaluations (AV-FG).
While there are many clinical settings that could accommodate CMFP evaluations, less common are physician practices that embrace these types of evaluations as standard practice. We suspect that firefighters may experience versions of CMFPs that do not administer many of the types of tests that NFPA 1582 proscribes. Within the industry, there are two moments when firefighters typically have their medical health and physical fitness evaluated as part of a CMFP: When prospective firefighter candidates are hired, or when an existing firefighter returns to work following an injury, illness, or extended leave (See Fig. 2). In both cases, these types of CMFP evaluations may be viewed by firefighters and care providers as either preventative care or within the realm of the primary care practice. As such, executive fire officers or fire officers vested with the responsibility of administrating OSHPs for a fire department may not encourage these evaluations or place significant weight on whether the evaluations conform to the types of processes NFPA 1582 sees as necessary for reaching a determination about a firefighter’s medical and physical fitness for duty.
As previously mentioned, the FTP at CSU is housed within a clinical research laboratory. This facility is not a point of care. However, it provides the ability for firefighters to participate in the tests that comprise a CMFP evaluation within a fee-for-service model. While there are several agencies that promote annual physicals for firefighters including the NFPA and IAFC, many firefighters do not complete an annual physical or participate in CMFPs that mandate annual physicals. In fact, firefighters who “feel fine” may not see the value in these types of screenings. While we believe that leaders of fire departments and communities have a responsibility to ensure members participate within annual CMFP evaluations that follow the standard of care outlined in NFPA 1582, we want to stress that we think that evaluations which are conducted through a literate care model that empowers firefighters to develop strategies and concrete plans for managing their long-term health, fitness, and wellness are needed in the occupation.
At this point, we have not yet started a systematic exploration of how the AV-FG could be integrated within clinical settings. However, we are aware there are many jurisdictions that have difficulty accessing clinics like the HPCRL where tests like a maximal treadmill protocol can be administered as part of a CMFP that is NFPA 1582 compliant. If the AV-FG can be adapted to take EKG tracings for firefighters as they complete the maximal treadmill protocol that mirror the quality and accuracy of those performed using 12-lead in clinical settings, it might be possible for fire departments or healthcare providers to administer these tests independently and send the results to a physician for analysis. Ultimately, these types of evaluations are an investment in a fire department’s most valuable asset: the firefighter.
5 Conclusion
Looking across the various contexts where firefighters might have access to care and feedback about their fitness and health (see Fig. 2) suggests that there are a multitude of ways that firefighters might experience CMFPs as end users. Whereas one firefighter might have an entry physical over the course of her career, another might undergo fitness and medical testing annually. Like Opel and Hart-Davidson [8], we think UX research is a useful tool for improving how health care experiences are designed, enacted, and maintained. UX researchers have a great deal to offer these systems, as the robust set practices, tools, and perspectives this discipline uses can be adapted to explore the ways that humans experience care and interact with information within these settings. For instance, firefighters who participate in CMFPs where the sole aim of interactions between care providers and firefighters is to reach a determination about fitness for duty differ markedly from those that are also accompanied by the information and insight offered by fitness professionals at the FTP. CMFPs which follow a literate care model can be used to empower firefighters by positioning them as active participants within these programs. Moreover, literate care models approach health, fitness, and wellness as a dynamic constellation of factors, many of which hinge on behavioral and lifestyle choices that can be adapted.
The quality of experiences firefighters have within CMFPs matters not only because these programs are tools that fire departments use to improve occupational safety and health outcomes, but because firefighters’ access to the types of care and information provided within these programs can identify conditions that determine whether a mother, father, son, daughter, or community member goes home alive when they leave the fire station. We believe that access to quality medical care, quality CMFPs, and quality OSHPs should be understood as a social justice issue because firefighters—and other blue-collar workers—are exposed to risk in occupational settings at disproportionate rates in comparison to white-collar workers. UX researchers—especially those who adapt community-based research and participatory design methodologies—can improve the ethical quality of interactions that occur within OSHPs and CMFPs by working alongside stakeholders to account for the types of experiences that blue-collar workers have within them, by envisioning technological or process improvements that could increase access to the types of care and information that are provided within them, and by advocating for designs that position workers as stewards of their own safety, health, and wellness.
References
NFFF: Everyone Goes Home. https://www.everyonegoeshome.com/. Accessed 21 Feb 2018
NFPA: NFPA 1500: Standard on Fire Department Occupational Safety, Health, and Wellness Program, 2018 edn. NFPA, Quincy (2018)
NFPA: NFPA 1582: Standard on Comprehensive Occupational Medical Program for Fire Departments, 2018 edn. NFPA, Quincy (2018)
NFPA: NFPA 1583: Standard on Health-Related Fitness Programs for Fire Department Members, 2015 edn. NFPA, Quincy (2015)
NFPA: NFPA 1584: Standard on the Rehabilitation Process for Members During Emergency Operations and Training Exercises, 2015 edn. NFPA, Quincy (2015)
Office of Disease Prevention and Health Promotion: Health Literate Care Model. https://health.gov/communication/interactiveHLCM/. Accessed 21 Feb 2018
Koh, H., Brach, C., Harris, L.M., Parchman, M.L.: A proposed ‘health literate care model would constitute a systems approach to improving patients’ engagement in care. Health Aff. 2, 357–367 (2013)
Opel, D.S., Hart-Davidson, W.: Challenges to patient experience: documenting evidence-based practice in the family health center. In: Marcus, A., Wang, W. (eds.) DUXU 2017. LNCS, vol. 10290, pp. 702–712. Springer, Cham (2017). https://doi.org/10.1007/978-3-319-58640-3_50
Winter, F.D., Seals, N., Martin, J., Russell, B.: Implementation of first wellness-fitness evaluation for the Dallas Fire-Rescue Department. Proc. Bayl. Univ. Med. Cent. 23(3), 235–238 (2010)
Smith, D.L.: Firefighter fitness: Improving performance and preventing injuries and fatalities ties. Curr. Sports Med. Rep. 10(3), 167–172 (2011)
Leffer, M., Grizzell, T.: Implementation of a physician-organized wellness regime (POWR) enforcing the 2007 NFPA standard 1582: Injury rate reduction and associated cost savings. J. Occup. Environ. Med. 52(3), 336–339 (2010)
NFPA: Fourth Needs Assessment of the U.S. Fire Service. NFPA, Quincy (2016)
Grabill, J.T.: Community-based research and the importance of research stance. In: Nickoson, L., Sheridan, M.P. (eds.) Writing Studies Research in Practice: Methods and Methodologies, pp. 210–219. Southern Illinois University Press, Carbondale (2012)
Adler, N.E., Newman, K.: Socioeconomic disparities in health: Pathways and policies. Health Aff. 21(2), 60–76 (2002)
Piha, K., Laaksonen, M., Marrtikainen, P., Rahkonen, O., Lahelma, E.: Socio-economic and occupational determinants of work injury absence. Eur. J. Public Health 23(4), 693–698 (2012)
World Health Organization: Environment and Health Risks: A Review of the Influence and Effects of Social Inequalities. WHO, Copenhagen (2010)
Griffin, S.C., Regan, T.L., Harber, P., Lutz, E., Chengcheng, H., Peate, W., Burgess, J.: Evaluation of a fitness intervention for new firefighters: injury reduction and economic benefits. Inj. Prev. 22(3), 181–188 (2016)
Macquire, B.L., Hunting, K.L., Guidotti, T.L., Smith, G.S.: Occupational injuries among emergency medical services personnel. Prehosp. Emerg. Care 9(4), 405–411 (2005)
Reichard, A.A., Marsh, S.M., Moore, P.H.: Fatal and nonfatal injuries among emergency medical technicians and paramedics. Prehosp. Emerg. Care 15(4), 511–517 (2011)
US Department of Labor, Bureau of Labor Statistics: Workplace Injury and Illness Summary (2013). https://www.bls.gov/news.release/osh.nr0.htm. Accessed 21 Feb 2018
Fahy, R.F., LeBlanc, P.R., Molis, J.L.: Firefighter Fatalities in the United States (2016)
LeMasters, G.K., Genaidy, A.M., Succop, P., Deddens, J., Sobeih, T., Barriera-Viruet, H., Dunning, K., Lockey, J.: Cancer risk among firefighters: a review and meta-analysis of 32 studies. J. Occup. Environ. Med. 48(11), 1189–1202 (2006)
Daniels, R.D., Bertke, S., Dahm, M.M., Yiin, J.H., Kubale, T.L., Hales, T.R., Baris, D., Zahm, S.H., Beaumont, J.J., Waters, K.M., Pinkerton, L.E.: Exposure-response relationships for select cancer and non-cancer health outcomes in a cohort of US firefighters from San Francisco, Chicago, and Philadelphia (1950-2009). Occup. Environ. Med. 72(10), 699–706 (2015)
Haynes, H.J.G., Molis, J.L.: United States Firefighter Injuries—2016. NFPA, Quincy (2017)
TriData Corporation: The economic consequences of firefighter injuries and their prevention (NIST GCR 05-874). NIST, Gaithersburg (2004)
Yang, J., Teehan, D., Farioli, A., Baur, D.M., Smith, D., Kales, S.N.: Sudden cardiac death among firefighters < 45 years of age in the United States. Am. J. Cardiol. 112(12), 1962–1967 (2013)
NIOSH: Career probationary fire fighter and captain die as result of rapid fire progression in a wind-driven residential structure fire—Texas (F2009-11). Death in the line of duty: A summary of a NIOSH fire fighter fatality investigation. NIOSH, Morgantown (2010)
NIOSH: Career lieutenant and fire fighter killed and two fire fighters injured by wall collapse at a large commercial structure fire (F2012-13). Death in the line of duty: A summary of a NIOSH fire fighter fatality investigation—Pennsylvania. NIOSH, Morgantown (2013)
NIOSH: Career fire fighter dies during fire-fighting operations at a multi-family fatality investigation—Massachusetts (F2011-31). Death in the line of duty: A summary of a NIOSH fire fighter fatality investigation. NIOSH, Morgantown (2013)
Abbot, D.: Project mayday. http://projectmayday.net/. Accessed 21 Feb 2018
Smith, D.L., Manning, T.S., Petruzzello, S.J.: Effect of strenuous live-fire drills on cardiovascular and physiological responses of recruit firefighters. Ergonomics 44(3), 244–254 (2001)
Heifetz, R.A., Laure, D.L.: The work of leadership. Harv. Bus. Rev. 75(1), 124–134 (1997)
NIOSH: Fire Fighter Fatality Investigation and Prevention. https://www.cdc.gov/niosh/fire/default.html. Accessed 21 Feb 2018
Moldenhauer, J.A., Sackey, D.J.: Transdisciplinarity, community-based participatory research, and user-based information design research. In: Marcus, A. (ed.) DUXU 2016. LNCS, vol. 9746, pp. 323–332. Springer, Cham (2016). https://doi.org/10.1007/978-3-319-40409-7_31
Blythe, S., Grabill, J.T., Riley, K.: Action research and wicked environmental problems: Exploring appropriate roles for researchers in professional communication. J. Bus. Tech. Commun. 22(3), 272–298 (2018)
Spinuzzi, C.: The methodology of participatory design. Tech. Commun. 52(2), 163–174 (2005)
Spinuzzi, C.: Topsight: A Guide to Studying, Diagnosing, and Fixing Information Flow in Organizations. Amazon Createspace, Austin (2013)
Amidon, T.R., Williams, E.A., Lipsey, T., Callahan, R., Nuckols, G., Rice, S.: Sensors and gizmos and data, oh my: Informating firefighters’ personal protective equipment. Commun. Des. Q. 5(4), 15–30 (2017)
Grant, C., Hamins, A., Bryner, N., Jones, A., Koepke, G.: Research Roadmap for Smart Fire Fighting: Summary Report. NIST Special Publication 1191. NIST (2015)
Acknowledgments
Funding for the Adaptive Challenges symposium was provided by the Office of Vice President for Research at CSU as part of the Pre-Catalyst for Innovative Partnerships (PRECIP) program. Funding for the promoting access to baseline cardiovascular health in rurally and geographically remote communities project is provided by the National Institution for Occupational Safety and Health via the Center for Work, Health, and Environment as part of a Total Worker Health Pilot Grant (U19OH011227-02). Funding for the fire-ground project physiological monitoring project is provided by the National Science Foundation under a SBIR Grant (1722014). We thank Dr. Genesea Carter for providing feedback on a draft of this paper.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG, part of Springer Nature
About this paper

Cite this paper
Amidon, T.R., Lipsey, T. (2018). Blue-Collars/Tough Designs: UX Within Fire Service Occupational Safety and Health Programs. In: Marcus, A., Wang, W. (eds) Design, User Experience, and Usability: Users, Contexts and Case Studies. DUXU 2018. Lecture Notes in Computer Science(), vol 10920. Springer, Cham. https://doi.org/10.1007/978-3-319-91806-8_45
Download citation
DOI: https://doi.org/10.1007/978-3-319-91806-8_45
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-91805-1
Online ISBN: 978-3-319-91806-8
eBook Packages: Computer ScienceComputer Science (R0)