
Abstract
Countering bioterrorism, as other health threats caused by infectious agents, requires good preparedness, and early warning and response, which can be achieved by an efficient epidemiological surveillance system. In 1990, Romania inherited a functional and quite efficient epidemiological surveillance system from the former communist regime, based on pyramidal and autocratic principles where the state control was absolute. In 2001, the assessment conducted by WHO/Europe showed many unsatisfactory elements of the remaining epidemiological surveillance system for communicable diseases, with a lack of procedures, poor microbiology laboratory capacities, and overlapping responsibilities. The lack of a coordinating body was evident, especially during bioterrorist threats following 9/11 attacks in New York. In 2003 and 2004, the PHARE Project offered an important opportunity for Romania to improve the Romanian System of Epidemiological Surveillance and Control of Communicable Diseases. At the end of this project many of the technical capacities had been improved, specialized trainings of epidemiologists and microbiologists were carried out, and a coordinating body of the epidemiological surveillance network was established [1]. Furthermore, a National Plan of Action was approved by the Minister of Health with the declared objective to improve the system in order to comply with EU standards. At present, the National Institute of Public Health hosts the National Center for Communicable Diseases Surveillance and Control which coordinates the epidemiological network and serves as the Romanian focal point for international institutions such as WHO and ECDC. Each year, comprehensive reports regarding surveillance in Romania of many communicable diseases are published, including diseases potentially related to bioterrorism. Until now, no evidence of a bioterrorism event has been registered in Romania.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others



Keywords
- West Nile Virus
- Communicable Disease
- National Reference Laboratory
- General Inspectorate
- National Action Plan
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
15.1 Introduction
Regarding the global impact of public health emergencies at the international level, communicable diseases are a top priority and countries need to develop a modern system of surveillance and control of outbreaks. This has also been a priority of the public health authorities in Romania in the last 10 years and important steps have been taken in order to develop an epidemiological surveillance system based on EU standards, integrated in a national emergency system [2].
15.2 Overview
Romania is a medium sized EU member state, with the ninth largest territory, and the seventh largest population. The country has an area of 238,391 km2and an estimated population of 21.5 million people (2009) with a density of 90 people per km2.
From the administrative point of view the country is divided in 41 counties and the capital Bucharest. Each county has its own administrative structures including those for health and emergencies.
Demographic indicators from 2008 showed a negative growth of population and a relatively high infant mortality, compared to other EU member states. The birth rate is 10.3 per 1,000 inhabitants, the general mortality is 11.8 per 1,000 inhabitants. The infant mortality is 11 per 1,000 live births, but with a decreasing trend. Life expectancy is 73.3 years (69.7 years for men and 77.4 years for women). The main diseases as causes of death are listed in Table 15.1.
The specific morbidity rates of communicable diseases are shown in Table 15.2. Tuberculosis remains one of the main concerns, with about 20,000 new cases each year and an increasing percentage of multidrug-resistant cases [3].
15.3 The National System for Emergency Situations Management
The national system for emergency situations management is organized in order to prevent and to manage emergency situations, providing and coordinating human, material, financial, and other resources. Its goal is to keep or to restore the normal status of life and society. The system is organized by the national public administration and consists of a network of bodies and structures with responsibilities in emergency situations management, organized in levels and areas of competence, which have the necessary resources in order to fulfill their legal duties. The main objectives and principles of emergency management are:
Prediction and prevention,
Saving people’s lives,
Respect for human rights and freedoms,
Cooperation on a national and international level,
Continuity from local authorities to the central public administration, and
Efficiency, active cooperation, and hierarchy in decision-making.
During emergency situations or potential status of emergency, specific measures are taken in accordance with the legal framework:
Warning people and institutions of all risks,
Declaring the state of an imminent threat,
Preventive and protective measures against a specific risk and, if needed, the decision of total or partial evacuation of the affected area,
Operative intervention forces and resources available in order to limit or eliminate negative effects,
Emergency aid,
Declaring the state of emergency according to conditions stipulated in Article 93 of the Romanian Constitution, and
Requesting or providing international assistance.
The main components of the National System for Emergency Situations Management are:
National Committee for Emergency Situations,
General Inspectorate for Emergency Situations,
Ministerial emergency committees,
County and local committees for emergencies, and
Operational centres for emergency situations.
The National Committee for Emergency Situations is acting under the authority of the Minister of Administration and Interior. When needed, it may be coordinated by the Prime Minister. An Interministerial Committee manages the ordinary activities, which is a body composed of decision makers and experts appointed by the ministries with responsibilities in managing emergencies. A Government Decision from 2004 established the organization and functioning of the National Committee [4]. The Minister of Administration and Interior is the Chairman of the National Committee for Emergency Situations, and a Secretary of State from the same Ministry is the Vice-Chairman. The members are secretaries of state from each ministry or a deputy head of each central public institution. Consultants are also included and they are experts from each ministry and central public institution. The Permanent Technical Secretariat of the National Committee for Emergency Situations functions as a specialized department within the National Operational Centre of the General Inspectorate for Emergency.
The General Inspectorate for Emergency Situations is a specialized department within the Ministry of Administration and Interior, which ensures coordination of activities for prevention and management of emergency situations. The Operational Center of the General Inspectorate is a technical body responsible for evaluation, notification, early warning and operational coordination of national level emergencies. It also ensures functioning of the Permanent Technical Secretariat of the National Committee for Emergency Situations.
The General Inspectorate coordinates and controls specialized public services in emergency situations, ensures cooperation with national civil protection, and is responsible for defence against fire and other emergency situations.
Ministerial emergency committees are established by Ministers or the heads of central public institutions and include decision makers and experts from the ministries and subordinate agencies, with responsibilities in specific emergency management activities. The Ministry of Health has its own committee able to respond and to mobilize resources for public health threats. The composition of a ministerial committee may include representatives of other ministries and institutions involved in the same area of activities.
A county committee for emergencies may be organized under the Prefect, the local representative of the government. The County Committee Board includes heads of decentralized services, local institution managers carrying out functions of county interest, and managers of relevant economic agents. The organization, powers and operational tasks of county committees are established by the decision of the Prefect. In the cities, towns, district of Bucharest, and other administrative divisions, local emergency committees may be established. A local committee is coordinated by a mayor and includes representatives of key public services and institutions from the administrative territory. The organization, powers, and functioning of local committees are established by decision of the mayor, endorsed by the prefect of the county.
15.4 Romanian System of Surveillance and Control of Communicable Diseases
The Ministry of Health (MoH) is responsible for all public health issues, including communicable diseases. The National Institute of Public Health (NIPH) was established in 2009 under the authority of the MoH [5]. Together with the National Institute of Research and Development in Microbiology and Immunology “Cantacuzino” and the National Institute for Infectious Diseases “Prof. Dr. Matei Bals”, it coordinates the surveillance and control of communicable diseases, early warning and response to health threats, the public health microbiological laboratory capacities, and preventive measures that should be taken in case of epidemics.
15.4.1 Short History
In 2001, the MoH decided to assess the capacity of early warning and response in order to better control communicable diseases. For this purpose it received technical assistance from the WHO/Regional Office for Europe, and a team of Romanian and international specialists made a comprehensive assessment of the institutional, technical and legislative situation and capacities. In order to improve the existing situation and to develop a surveillance system compatible with the EU, the MoH accepted the recommendations made by the WHO/Europe team. The opportunity to develop the surveillance system came with an EU-sponsored PHARE project “Improving the Romanian System for Epidemiological Surveillance and Control of Communicable Diseases” that lasted from early 2003 until October 2004. The beneficiaries and participants involved in the PHARE project were the MoH through the Department of Public Health, the four regional public health institutes (Bucharest, Cluj, Iasi, Timisoara) and also the 42 district public health directorates and the National Institute for Research and Development in Microbiology and Immunology “Cantacuzino” through its national reference laboratories [1]. Two other institutions with responsibilities for specific surveillance networks are the National Institute for Infectious Diseases “Prof. Dr. Matei Bals” for HIV/AIDS and the Institute for Pneumology “Marius Nasta” for tuberculosis, but they did not directly participate in the PHARE project.
The recommendations made by the international expert team involved in the PHARE project were taken into account in developing a national action plan for the improvement of the communicable disease surveillance system in Romania. The main point was to establish a national competent body, which should be able to:
Be responsible for the funding and performance management of the regional and district public health structures;
Maintain consolidated national health surveillance databases for communicable diseases;
Use surveillance data for the development, publication and dissemination of national policies and good practices in the field of public health;
Represent the interests of the MoH, in respect of training in the field of communicable diseases, with all national training bodies (undergraduate and postgraduate);
Represent Romania in all specialist public health functions related to communicable diseases necessary for international cooperation and legal purposes.
The MoH, through Order 123/2003, approved the national action plan. Based on those recommendations, a National Centre for Communicable Diseases Surveillance and Control (NCCDSC) was established. This centre became operational in January 2005. It was located in the Institute of Public Health Bucharest, with the main objective to coordinate the whole national communicable diseases network. Other roles mentioned in the national action plan included monitoring of the national immunization programmes, coordinating the system of early warning and rapid response at the national level, and the management of a dedicated information system.
15.4.2 Current Situation
At present, the NIPH is a coordinating body of a communicable diseases network (Fig. 15.1), through the NCCDSC. NIPH is a body designated to represent the Romanian Government for the purposes set out in the EU decisions 2119/98/EC, 2000/57/EC and all subsequent amendments, and in the reporting functions designated in 2003/542/EC. Recently, NIPH has been designated an ECDC Coordinating Competent Body. Main tasks of the NIPH are:
Coordination of the national surveillance and control of communicable diseases network;
Technical coordination of the national alert system for communicable diseases;
Technical coordination of the rapid response in case of outbreaks or other public health events;
Surveillance, response, threat detection and training;
Monitoring and evaluation of the national immunization programme;
Coordination of the information system on communicable diseases, reporting to international organizations.
The regional public health institutes are responsible for:
Coordination of the epidemiological activities of the district public health directorates;
Surveillance and analysis, and coordination of interventions when needed at a regional level;
Technical assistance to the district public health directorates;
Diagnosis of communicable diseases, if expert level is needed;
Training activities in the field of public health.
The district public health directorates are subordinated to the NCCDSC and the regional public health institutes. The district public health directorates:
Collect data from the existing sources within the territory and analyze communicable diseases data based on time, place, person, and trend for early warning and rapid response;
Participate in risk assessments for events threatening public health and having a potential national and international spread, organize and administer local communicable diseases databases;
Report, according to legal regulations, the notifiable communicable diseases;
Collaborate with NGOs in the process of communicable diseases surveillance;
Verify how family doctors detect and report cases of communicable diseases;
Monitor and verify how methodologies and protocols for etiological diagnosis of communicable diseases are implemented;
Organize epidemiological investigations, identify and coordinate the required measures in order to limit outbreaks of communicable diseases in communities;
Develop specific activities within the framework of emergency intervention plans.
Fig. 15.1 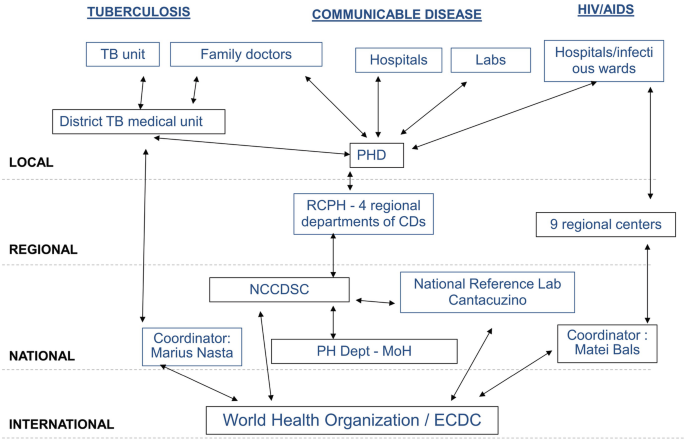
Structure of the communicable diseases network in Romania


Infectious disease hospitals report HIV/AIDS data to the eight regional HIV centres (Bucharest, Brasov, Cluj, Timisoara, Craiova, Constanta, Iasi, and Targu-Mures). These centres then report to the national level at the Institute for Infectious Diseases, where data are processed in the HIV/AIDS Monitoring and Evaluation Department. At the district level, forms are also sent to the district public health directorates, which also gather information on HIV testing activities in blood centres and laboratories.
For tuberculosis, suspected cases are diagnosed and confirmed by the tuberculosis district hospital. Both family physicians and tuberculosis specialists from the nearest tuberculosis centre are responsible for case notification and for completing the case management form. The completed form is forwarded to the district tuberculosis dispensary, and from there to the district health statistics office and to the national level at the Institute of Pneumology.
15.5 Public Health Microbiological Laboratories
The public health network has three levels of microbiological diagnostic activities: national (through the national reference laboratories), regional, and local. At the national level there is the National Institute for Research and Development in Microbiology and Immunology “Cantacuzino”. Established in 1923, the “Cantacuzino” Institute is a well known Romanian medical institution highly specialized in microbiological diagnostics and in vaccine production. Within the Institute, there are three units responsible for public health, vaccine production and R&D. The national reference laboratories were refurbished and equipped through the PHARE and World Bank projects between 2003 and 2005.
There are ten national reference laboratories, some of them with distinct units inside (see Table 15.3). The staff is 120, and 59 are highly qualified (medical doctors, biologists, biochemists). Microbiological diagnostics at the “Cantacuzino” Institute started in 1950 and continued in various organizational formats. Available services for microbiological diagnosis include 107 usual tests, 39 serology tests, and 53 highly specialized diagnostic procedures. A BSL-3 laboratory is under development through a World Bank project [6].
The number of tests performed by national reference laboratories is around 40,000 per year, but the estimated capacities are at least three times higher, 125,000 per year being a reasonable work load. The problem regarding the relative small number of tests performed, especially those regarding the circulation of microbial strains in Romania, is linked to the financing model of the “Cantacuzino” Institute which is not a state budget institution and needs to have dedicated contracts with regional and local public health authorities in order to perform microbiological investigations. This subject is under discussion and a direct financing from the state budget should be implemented.
The quality of work done by the national reference laboratories is certified by External Quality Assessment (EQA) schemes for many of the microbiological diagnostic procedures performed: polio, influenza, measles, HIV, diphtheria, Salmonellaand other gram-negatives, gram-positives, parasitology, antibiotic susceptibility testing, and Legionella, Borreliaand pertussis.
Many public health diagnostic activities were performed, and all important epidemiological threats were controlled by the national reference laboratories. Among these threats were West Nile Virus epidemics in 1996 and 2010, anthrax suspect samples (hundreds of tests performed in 2001 and 2002), SARS in 2003, measles in 2005, avian influenza in 2006, H1N1 influenza pandemic in 2009.
The “Cantacuzino” Institute is a member of various WHO and ECDC networks:
WHO: FLUNET (Influenza Surveillance Network), Global Polio Eradication Initiative;
ECDC: EVD (emerging and vector borne diseases), VPD (vaccine preventable diseases), FWD (food and water borne diseases), AMR (antimicrobial resistance), HAI (healthcare associated infections), influenza, invasive bacterial infections, zoonoses;
Research/public health networks: FLUSECURE, REVERSE.
The “Cantacuzino” Institute is also a member of the Pasteur and Associated Institutes Network, many of its specialists having been trained in this network, beginning in 1991. Other roles of the “Cantacuzino” Institute include: national bacterial strains collection, reference material source, and scientific advisor for the MoH and other interested stakeholders. Specialists from the “Cantacuzino” Institute represent Romania in different international technical bodies at the UN, WHO, and ECDC.
The regional centres for public health in Cluj, Iasi, and Timisoara have important microbiological laboratory capacities in terms of staff and equipment, and are responsible for complex diagnostics of communicable diseases in their catchment areas. The “Cantacuzino” Institute is functioning also as a regional centre for the southern part of Romania.
Local district public health directorates have various microbiological laboratory facilities. Some of them, and especially those located at medical universities, are well equipped and have trained personnel. Others use the resources of the regional public health institutes and perform only basic tests themselves.
15.6 National Network for Treatment of Communicable Diseases
The National Institute for Infectious Diseases “Prof. Dr. Matei Bals” is a coordinating body of a network of nine regional centres for the treatment of communicable diseases. The centres were developed in 2007, after the threat of avian flu epidemics. The network is part of a World Bank project which financed necessary investments for care and treatment facilities, including intensive care units, microbiological laboratory equipment, and other logistic needs.
At present, the network is functional and some locations were tested during the H1N1 influenza pandemic that also affected Romania, when hundreds of patients were hospitalized and treated, especially in the central unit, the National Institute for Infectious Diseases “Prof. Dr. Matei Bals”.
The network was developed based on the existing one for surveillance and treatment of HIV/AIDS. After 1990, Romania registered an important number of HIV/AIDS cases, affecting especially children. This situation required extraordinary measures, and one of them was to organize a medical network able to treat and to offer counseling and preventive measures to affected people. This network, coordinated by the National Institute for Infectious Diseases “Prof. Dr. Matei Bals”, is hosting the database of HIV/AIDS infected people and has achieved important results in the control of the disease [5]. The Romanian government has given significant financial resources and HAART therapy is offered to more than 8,000 patients.
The Institute of Pneumology “Marius Nasta” has similar responsibilities regarding surveillance and treatment of tuberculosis infections. At the local level many facilities (hospitals, laboratories) are dedicated to these patients. Tuberculosis represents one of the main challenges for the public health system in Romania, with more than 20,000 new cases each year, important national and international (Global Fund) resources being allotted.
Both institutes are working together with NCCDSC. Epidemiological data from the local level for HIV/AIDS and tuberculosis are sent periodically to district public health directorates and to NCCDSC.
15.7 Surveillance of Communicable Diseases
The communicable diseases surveillance network is financed by the state budget under the National Programme on Community Health. Treatment of communicable diseases is covered by the public health insurance funds.
The reporting system covers 65 communicable diseases. These are classified as: (1) Diseases with nominal immediate notification by phone; (2) Diseases with nominal notification within 24 h after detection; and (3) Diseases with numerical periodic reporting (weekly, monthly, quarterly, and annually). Detection and notification of communicable diseases are among the responsibilities of family doctors, of ambulatory units and of hospitals, mainly of the infectious diseases hospitals, or other specialized units [7].
The confirmation of cases is done in districts and in Bucharest by the laboratories of the local district public health directorate, and/or by the regional and national reference laboratories. The transmission of data is by phone or by fax, and the notification forms for each communicable disease case are sent by mail or courier service. Data analysis is carried out in a few districts at the local level; usually data analysis is conducted at regional and national levels and the feedback to the district is limited. The surveillance of certain communicable diseases (tuberculosis, HIV/AIDS) is done also in parallel systems using a separate informational flow.
A group of 11 communicable diseases – wild polio virus infection, influenza with a new virus subtype, cholera, plague, hemorrhagic fevers, yellow fever, smallpox, varioloid, SARS, an unexpected infectious disease, and an unexpected health event – are reported immediately; the district public health directorates report immediately to the Bureau for International Health Regulation and Toxicology Information (BIHRTI), an office within the National Institute of Public Health (which is the focal point for IHR). NCCDSC verifies the information and together with BIHRTI informs the MoH which notifies the WHO. These cases have to be confirmed by national reference laboratories [7].
Another group of 25 communicable diseases has to be reported immediately by phone to the district public health directorates by all medical assistance providers. Within 24 h, the district public health directorate sends the report to the regional public health institute. Further reports are sent to the NCCDSC and BIHRTI, which inform the MoH, after evaluating the level of importance for the epidemiological event. Written forms are also sent to the authorities mentioned.
There are ten communicable diseases which are reported on a monthly basis to the district public health directorates by all the medical assistance providers. Aggregated data on influenza, acute respiratory infections, acute diarrheal disease, West Nile meningo-encephalitis, and other communicable diseases are reported on weekly basis, using specific methodologies.
For all communicable diseases the medical assistance providers send to the district public health directorates a notification form 5 days after detection. District public health directorates send the duplicates of the notification forms to the regional public health institutes, which send the regional data to NCCDSC.
NCCDSC, the competent body for communicable diseases surveillance, reports to ECDC the diseases under 2119/98/EC Decision, after the validation of cases. The regional public health institutes provide quarterly and annual reports for the regions. NCCDSC and BIHRTI also provide quarterly and annual reports, which are sent to the MoH.
15.8 Early Warning System
In 2005, the Minister of Health ordered the methodology for early warning and rapid response. The list of communicable diseases included in this system are smallpox, plague, acute hemorrhagic fevers, SARS, syndromes that could raise the suspicion of a communicable disease: acute watery diarrhea for cholera suspicion, acute diarrhea with or without blood, acute icteric syndrome, acute infections of the lower respiratory tract, rubella suspicion, meningitis/encephalitis suspicion, malaria suspicion, fever of unknown origin and unknown disease occurring in a cluster. The methodology is based on case definitions, alert thresholds, defining responsibilities and information flow, and providing the reporting format [7].
Family doctors detect, notify and report the case and transfer the patient to the specialist for infectious diseases, who notifies by phone the event and fills a dedicated warning report submitted to the district public health directorate.
The infectious diseases hospital confirms or invalidates the suspicion and notifies the district public health directorate, which, through its epidemiology unit, analyses data from health care providers and takes the measures of active detection of cases and control and sends a preliminary report of epidemiological warning to the regional public health institute, and further on to NCCDSC. Diagnosis is confirmed by national reference laboratories.
Local measures are taken by district public health directorates, with technical assistance from the regional level. If the outbreak is spreading and affects more than one region the NCCDSC takes the lead and organizes measures, reporting to the MoH and to the international organizations.
Table 15.4presents the list of confirmed and suspect cases of communicable diseases in 2010 which represent a main threat for public health and are of bioterrorism concern [3]. Until now, no evidence of bioterrorism has been registered in Romania.
15.9 Conclusions
The capacity of the Romanian authorities to respond to different health threats due to communicable diseases has improved in the last few years in terms of diagnostic capacities and organizational matters. Early warning and efficiency of response of the epidemiological surveillance system was proven during the H1N1 influenza pandemic and in other communicable diseases emergencies.
The improvements registered in the last few years include data collection and reporting methodology for communicable diseases surveillance, information flow of the unique notification form for communicable diseases, and establishment of the National Electronic Register for Communicable Diseases.
The district public health authorities are the focal point for all the communicable diseases notified in the district and data are validated at the regional and national level.
The main threats are represented by emerging and re-emerging communicable diseases due to intensified international traffic of persons and goods and bioterrorist events.
From an organizational point of view, education of family doctors should improve their capability to recognize and report communicable diseases and apply control measures at the source. Elaboration of the national surveillance manual is needed as well as enhancing the laboratory capacities and implementing a reliable information system for communicable diseases based on a new technological platform.
Strengthening cooperation with emergency staff from the Ministry of Admin-istration and Interior and from other government bodies responsible for security of social and economic activities is desired.
References and Further Reading
Stevens R (2004) Final report to delegation of EC in Bucharest regarding PHARE project, EuropeAid/113121/D/SV/RO, technical assistance for improving the Romanian system for epidemiological surveillance and control of communicable diseases, Bucharest
The Dubrovnik pledge on surveillance and prioritization of infectious diseases – report on a WHO meeting, Bucharest, Romania, 21–23 Nov 2002
National Institute of Public Health Bucharest (2011) Report on communicable diseases 2009, report of NCCDSC activity, 2011, www.insp.gov.ro
General inspectorate for emergency situations (Government Decisions 1489, 1490/2004, 1514/2005)
Vladescu C, Scîntee G, Olsavszky V, Allin S, Mladovsky P (2008) Romania: health system review. Health systems in transition 10(3):1–172
Ionescu G, Codita I, Canton A (2010) Role of the microbiology NRLs in the European context, updated presentation on 23rd meeting of the ECDC advisory forum, 29–30 Sept 2010
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media Dordrecht
About this paper
Cite this paper
Rafila, A., Pitigoi, D. (2013). Case Study – Romania. In: Hunger, I., Radosavljevic, V., Belojevic, G., Rotz, L. (eds) Biopreparedness and Public Health. NATO Science for Peace and Security Series A: Chemistry and Biology. Springer, Dordrecht. https://doi.org/10.1007/978-94-007-5273-3_15
Download citation
DOI: https://doi.org/10.1007/978-94-007-5273-3_15
Published:
Publisher Name: Springer, Dordrecht
Print ISBN: 978-94-007-5272-6
Online ISBN: 978-94-007-5273-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)