
Abstract
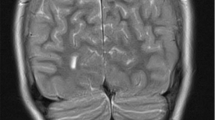
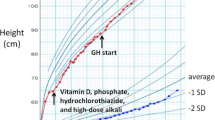
Autoimmune polyendocrinopathy-can-didiasis-ectodermal dystrophy (APECED) is an inherited disease which may comprise many endocrine and non-endocrine components. GH insufficiency has not been recognised as a classical manifestation of this syndrome. We describe the case of a girl with APECED, who presented with four endocrine (hypoparathyroidism, Addison’s disease, hypothyroidism, gonadal failure) and three non-endocrine components (candidiasis, ectoder-mal dystrophy and lichen ruber planus). In addition, growth failure was documented beginning at approximately 8 years; bone age was delayed and stimulated GH peaks after clonidine and arginine were 2.2 and 9.2 μg/l, respectively. A partial empty sella was found on a computed tomography scan of the hypothalamic-pituitary region. At 10.5 years rhGH therapy was started and height gain of 26 cm was observed after 2.7 years of treatment. Puberty started at 11.2 years and menarche occurred at 12.7 years. At 13.25 years rhGH therapy was discontinued owing to frequent hypocal-cemic crises; serum IGF-1 levels were persistently low in the following years (between 160 and 180 μg/l, normal range for age 250–600 μg/l). The patient attained a final height of 160.8 cm, which was appropriate for her target height. The presence of lichen ruber planus and GH insufficiency probably secondary to empty sella are two unusual findings in patients with APECED.
Similar content being viewed by others
References
Ahonen P., Myllarniemi S., Sipila I., Perheentupa J. Clinical variation of autoimmune polyendocrinopa-thy-candidiasis — ectodermal dystrophy (APECED) in a series of 68 patients. N. Engl. J. Med. 322: 1829, 1990.
Perheentupa J. Autoimmune Polyendocrinopathy-Candidiasis-Ecto-derm Dystrophy (APECED). Horm. Metab. Res. (Suppl.) 28: 353, 1996.
Gourmelen M., Pham-Huu-Trung M.T., Girard F. Transient partial hGH deficiency in prepubertal children with delay of growth. Pediatr. Res. 13: 221, 1979.
Bourguignon J-P. Linear growth as a function of age at onset of puberty and sex steroid dosage: therapeutic implications. Endocr. Rev. 9: 467, 1988.
Stamoyannou L., Karachaliou F., Gioureli E., Voskaki E., Mengreli C., Bartsocas C.S., Koutselinis A. Effect of growth hormone therapy on bone metabolism of growth hormone deficient children. Eur. J. Pediatr. 156: 592, 1997.
Ohlsson C., Bengtsson B.-A., Isaksson O.G.P., Andreassen T.T., Slootweg M.C. Growth hormone and bone. Endocr. Rev. 19: 55, 1998.
Shulman D.I., Martinez C.R., Bercu B.B., Root A.W. Hypothalamic-pituitary dysfunction in primary empty sella syndrome in childhood. J. Pediatr. 108: 540, 1986.
Rappaport R., Logrono R. Primary empty sella syndrome in childhood: association with precocious puberty. Clin. Pediatr. 30: 466, 1991.
Ridgway E.C., Kourdes I.A., Kliman B., Biges T., Maloof F. Thyrotropin and prolactin pituitary reserve in the “empty sella syndrome”. J. Clin. Endocrinol. Metab. 41: 968, 1975.
Zucchini S., Ambrosetto P., Carla G., Tani G., Franzoni E., Cacciari E. Primary empty sella: differences and similarities between children and adults. Acta Paediatr., 84: 1382, 1995.
Komatsu M., Kondo T., Yamauchi K., Yokokawa N., Ichikawa K., Ishiara M., Aizawa T., Yamada T., Imai Y., Tanaka K., Taniguchi K., Watanabe T., Taka-hashi Y. Antipituitary antibodies in patients with the primary empty sella syndrome. J. Clin. Endocrinol. Metab. 67: 633, 1988.
Arvanitakis C., Knouss R.F. Selective hypopituitarism. Impaired cell-mediated immunity and chronic mucocutaneous candidiasis. JAMA 225: 1492, 1973.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Franzese, A., Valerio, G., Di Maio, S. et al. Growth hormone insufficiency in a girl with the autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Endocrinol Invest 22, 66–69 (1999). https://doi.org/10.1007/BF03345481
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03345481