
Abstract
Summary
Fracture risk scores generated from population-based administrative healthcare data showed comparable or better discrimination than the Fracture Risk Assessment Tool (FRAX) scores computed without bone mineral density for predicting incident major osteoporotic fracture. Administrative data may be useful to identify individuals at high fracture risk at the population level.
Purpose
To evaluate the discrimination of fracture risk scores defined using inputs available from administrative data for predicting incident major osteoporotic fracture (MOF) and hip fracture (HF) alone.
Methods
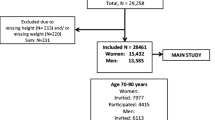
Using the Manitoba Bone Mineral Density (BMD) Database (1997–2013), we identified 61,041 individuals aged 50 years or older with healthcare coverage following their first BMD test. We calculated two-modified FRAX)scores based on administrative data: FRAX-A and FRAX-A+. The FRAX-A modification used all FRAX inputs, except for BMD, body mass index, and parental HF, while the FRAX-A+ modification using all FRAX-A inputs plus a comorbidity score, number of hospitalizations in the 3 years prior to the BMD test, depression diagnosis, and dementia diagnosis. FRAX scores computed with BMD (i.e., FRAX [BMD]) and without BMD (i.e., FRAX [no-BMD]) were the comparators.
Results
During a mean of 7 years of follow-up, we identified 5306 (8.7%) incident MOF and 1532 (2.5%) incident HF. The c-statistic for MOF associated with FRAX-A was lower than FRAX (BMD) (0.655 vs 0.675; P < 0.05) and comparable to FRAX (no-BMD) (0.654; P = 0.07). The c-statistic for MOF using FRAX-A+ (0.663) was lower than FRAX (BMD) but higher than FRAX (no-BMD) (both P < 0.05). For predicting incident HF, c-statistics associated with FRAX-A (0.762) and FRAX-A+ (0.767) were lower than FRAX (BMD) (0.789) and FRAX (no-BMD) (0.773; both P < 0.05).
Conclusions
FRAX-A and FRAX-A+ showed comparable or better discrimination than FRAX without BMD for predicting incident MOF, but slightly lower discrimination for HF alone.
Similar content being viewed by others
References
Wiktorowicz ME, Goeree R, Papaioannou A, Adachi JD, Papadimitropoulos E (2001) Economic implications of hip fracture: health service use, institutional care and cost in Canada. Osteoporos Int 12:271–278
Papaioannou A, Wiktorowicz ME, Adachi JD, Goeree R, Papadimitropoulos E, Bedard M (2000) Mortality, independence in living, and re-fracture, one year following hip fracture in Canadians. J Soc Obstet Gynaecol Can 22:591–597
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17:1726–1733
Tenenhouse A, Joseph L, Kreiger N, Poliquin S, Murray TM, Blondeau L, Berger C, Hanley DA, Prior JC, Grp CR (2000) Estimation of the prevalence of low bone density in Canadian women and men using a population-specific DXA reference standard: the Canadian multicentre osteoporosis study (CaMos). Osteoporos Int 11:897–904
Kanis JA, Borgstrom F, De Laet C, Johansson H, Johnell O, Jonsson B, Oden A, Zethraeus N, Pfleger B, Khaltaev N (2005) Assessment of fracture risk. Osteoporosis Int 16:581–589
Kanis JA, Oden A, Johansson H, Borgstrom F, Strom O, McCloskey E (2009) FRAX and its applications to clinical practice. Bone 44:734–743
Shepstone L, Lenaghan E, Cooper C, Clarke S, Fong-Soe-Khioe R, Fordham R, Gittoes N, Harvey I, Harvey N, Heawood A, Holland R, Howe A, Kanis J, Marshall T, O'Neill T, Peters T, Redmond N, Torgerson D, Turner D, McCloskey E, Shepstone L, Lenaghan E, Cooper C, Clarke S, Fong-Soe-Khioe R, Fordham R, Gittoes N, Harvey I, Harvey N, Heawood A, Holland R, Howe A, Kanis J, Marshall T, O'Neill T, Peters T, Redmond N, Torgerson D, Turner D, McCloskey E, Crabtree N, Duffy H, Parle J, Rashid F, Stant K, Taylor K, Thomas C, Knox E, Tenneson C, Williams H, Adams D, Bion V, Blacklock J, Dyer T, Bratherton S, Fidler M, Knight K, McGurk C, Smith K, Young S, Collins K, Cushnaghan J, Arundel C, Bell K, Clark L, Collins S, Gardner S, Mitchell N (2018) Screening in the community to reduce fractures in older women (SCOOP): a randomised controlled trial. Lancet 391:741–747
Ettinger B, Ensrud KE, Blackwell T, Curtis JR, Lapidus JA, Orwoll ES, Osteoporotic Fracture in Men Study Research G (2013) Performance of FRAX in a cohort of community-dwelling, ambulatory older men: the Osteoporotic Fractures in Men (MrOS) study. Osteoporos Int 24:1185–1193
Briot K, Paternotte S, Kolta S, Eastell R, Felsenberg D, Reid DM, Gluer CC, Roux C (2013) FRAX(R): prediction of major osteoporotic fractures in women from the general population: the OPUS study. PLoS One 8:e83436
Kanis JA, Harvey NC, Johansson H, Oden A, Leslie WD, McCloskey EV (2015) FRAX and fracture prediction without bone mineral density. Climacteric 18(Suppl 2):2–9
Reber KC, Konig HH, Becker C, Rapp K, Buchele G, Machler S, Lindlbauer I (2018) Development of a risk assessment tool for osteoporotic fracture prevention: a claims data approach. Bone 110:170–176
Rubin KH, Moller S, Holmberg T, Bliddal M, Sondergaard J, Abrahamsen B (2018) A new fracture risk assessment tool (FREM) based on public health registries. J Bone Miner Res 33:1967–1979
Leslie WD, Metge C (2003) Establishing a regional bone density program: lessons from the Manitoba experience. J Clin Densitom 6:275–282
Leslie WD, Caetano PA, MacWilliam LR, Finlayson GS (2005) Construction and validation of a population-based bone densitometry database. J Clin Densitom 8:25–30
Lix LM, Azimaee M, Osman BA, Caetano P, Morin S, Metge C, Goltzman D, Kreiger N, Prior J, Leslie WD (2012) Osteoporosis-related fracture case definitions for population-based administrative data. BMC Public Health 12:301
O'Donnell S (2013) Use of administrative data for national surveillance of osteoporosis and related fractures in Canada: results from a feasibility study. Arch Osteoporos 8:143
Leslie WD, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA, Manitoba Bone Density P (2010) Independent clinical validation of a Canadian FRAX tool: fracture prediction and model calibration. J Bone Miner Res 25:2350–2358
Fraser LA, Langsetmo L, Berger C, Ioannidis G, Goltzman D, Adachi JD, Papaioannou A, Josse R, Kovacs CS, Olszynski WP (2011) Fracture prediction and calibration of a Canadian FRAX® tool: a population-based report from CaMos. Osteoporos Int 22:829–837
Haller B, Schmidt G, Ulm K (2013) Applying competing risks regression models: an overview. Lifetime Data Anal 19:33–58
Brier GW (1950) Verification of forecasts expressed in terms of probability. Mon Weather Rev 78:1–3
Delong ER, Delong DM, Clarke-Pearson DL (1988) Comparing areas under two or more correlated reciever operating characteristics curves: a nonparamentric approach. Biometrics 44:837–845
Turner DA, Khioe RFS, Shepstone L, Lenaghan E, Cooper C, Gittoes N, Harvey NC, Holland R, Howe A, McCloskey E, O’Neill TW, Torgerson D, Fordham R, the SCOOP Study Team (2018) The cost-effectiveness of screening in the community to reduce osteoporotic fractures in older women in the UK: economic evaluation of the SCOOP study. J Bone Miner Res 33:845–851
Rubin KH, Rothmann MJ, Holmberg T, Høiberg M, Möller S, Barkmann R, Glüer CC, Hermann AP, Bech M, Gram J, Brixen K (2018) Effectiveness of a two-step population-based osteoporosis screening program using FRAX: the randomized risk-stratified osteoporosis strategy evaluation (ROSE) study. Osteoporos Int 29:567–578
Rothmann MJ, Moller S, Holmberg T et al (2017) Non-participation in systematic screening for osteoporosis-the ROSE trial. Osteoporos Int 28:3389–3399
Yang S, Leslie WD, Yan L, Walld R, Roos LL, Morin SN, Majumdar SR, Lix LM (2016) Objectively verified parental hip fracture is an independent risk factor for fracture: a linkage analysis of 478,792 parents and 261,705 offspring. J Bone Miner Res 31:1753–1759
Acknowledgements
This study was not funded. The authors acknowledge the Manitoba Centre for Health Policy for use of data contained in the Population Health Research Data Repository (HIPC# 2016/2017–29). The results and conclusions are those of the authors and no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health, Healthy Living and Seniors, or other data providers is intended or should be inferred.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
Shuman Yang, William D. Leslie, and Lisa M. Lix declare that they have no conflict of interest.
Suzanne N. Morin declares that she has received research grants from Amgen and Merck.
Electronic supplementary material
ESM 1
(DOCX 19 kb)
Rights and permissions
About this article

Cite this article
Yang, S., Leslie, W., Morin, S. et al. Administrative healthcare data applied to fracture risk assessment. Osteoporos Int 30, 565–571 (2019). https://doi.org/10.1007/s00198-018-4780-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-018-4780-6