
Abstract
Background
Previous interventions in achalasia such as pneumatic dilation (PD) might lead to difficulties with peroral endoscopic myotomy (POEM) along with sub-optimal outcomes. There are limited data in the literature on outcomes of POEM after PD, especially from the western hemisphere. Hence, we aimed to determine the safety and efficacy of POEM for recurrent symptoms after PD compared to treatment naïve achalasia patients.
Methods
Medical records of achalasia patients who underwent POEM at our institution between April 2014 and October 2019 were reviewed. Patients who had POEM for recurrent symptoms after prior PD were matched at 1:2 ratio with treatment naïve achalasia patients using propensity score matching. Patients who had prior Heller myotomy were excluded. Patient demographics, Eckardt scores, timed barium swallow (TBE), high-resolution esophageal manometry (HREM), and pH study findings were compared between the two groups, pre- and 2 months post-POEM. Treatment success was defined as reduction of Eckardt score to ≤ 3.
Results
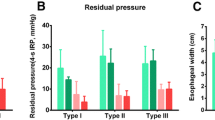
A total of 39 patients (prior PD = 13; treatment naïve = 26) were included. Patient demographics, procedural, and peri-procedural outcomes were similar in both groups. Treatment success was similar in both groups, 100.0% in prior PD vs 91.7% in treatment naïve group (p = 0.53). On adjusted analysis, there was no significant difference in the pre–post-POEM improvement in Eckardt scores, TBE, and HREM parameters in the two groups. Gastroesophageal reflux disease rates were also similar in both groups.
Conclusions
In achalasia with recurrent symptoms after PD, POEM is a safe and highly effective treatment modality. Prior PD does not seem to influence the outcomes or efficacy of POEM.




Similar content being viewed by others


References
Park W, Vaezi MF (2005) Etiology and pathogenesis of achalasia: the current understanding. Am J Gastroenterol 100:1404. https://doi.org/10.1111/j.1572-0241.2005.41775.x
Piñeiro-Carrero VM, Sullivan CA, Rogers PL (2001) Etiology and treatment of achalasia in the pediatric age group. Gastrointest Endosc Clin N Am 11(2):387–408
Wadhwa V, Thota PN, Parikh MP, Lopez R, Sanaka MR (2017) Changing trends in age, gender, racial distribution and inpatient burden of achalasia. Gastroenterol Res 10(2):70–77. https://doi.org/10.14740/gr723w
Inoue H, Minami H, Kobayashi Y et al (2010) Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy 42(4):265–271. https://doi.org/10.1055/s-0029-1244080
Kilic A, Schuchert MJ, Pennathur A, Gilbert S, Landreneau RJ, Luketich JD (2009) Long-term outcomes of laparoscopic Heller myotomy for achalasia. Surgery. 146(4):826–831. https://doi.org/10.1016/j.surg.2009.06.049discussion 831–833
Emami MH, Raisi M, Amini J et al (2008) Pneumatic balloon dilation therapy is as effective as esophagomyotomy for achalasia. Dysphagia 23(2):155–160. https://doi.org/10.1007/s00455-007-9115-2
Pasricha PJ, Hawari R, Ahmed I et al (2007) Submucosal endoscopic esophageal myotomy: a novel experimental approach for the treatment of achalasia. Endoscopy 39(9):761–764. https://doi.org/10.1055/s-2007-966764
Ramzan Z, Nassri AB (2013) The role of Botulinum toxin injection in the management of achalasia. Curr Opin Gastroenterol 29(4):468–473. https://doi.org/10.1097/MOG.0b013e328362292a
Boeckxstaens G, Annese V, Des VS et al (2011) European Achalasia Trial I (2011) Pneumatic dilation versus laparoscopic Heller’s myotomy for idiopathic achalasia. N Engl J Med 364:1807–1816
Ling T, Guo H, Zou X (2014) Effect of peroral endoscopic myotomy in achalasia patients with failure of prior pneumatic dilation: a prospective case-control study. J Gastroenterol Hepatol 29(8):1609–1613. https://doi.org/10.1111/jgh.12570
Kumbhari V, Behary J, Szczesniak M, Zhang T, Cook IJ (2013) Efficacy and safety of pneumatic dilatation for achalasia in the treatment of post-myotomy symptom relapse. Am J Gastroenterol 108(7):1076–1081. https://doi.org/10.1038/ajg.2013.32
Borges AA, de Lemme EM, Abrahao LJ et al (2014) Pneumatic dilation versus laparoscopic Heller myotomy for the treatment of achalasia: variables related to a good response. Dis Esophagus 27(1):18–23. https://doi.org/10.1111/dote.12064
Gockel I, Junginger T, Bernhard G, Eckardt VF (2004) Heller myotomy for failed pneumatic dilation in achalasia: how effective is it? Ann Surg 239(3):371–377. https://doi.org/10.1097/01.sla.0000114228.34809.01
Lynch KL, Pandolfino JE, Howden CW, Kahrilas PJ (2012) Major complications of pneumatic dilation and heller myotomy for Achalasia: single-center experience and systematic review of the literature. Am J Gastroenterol 107(12):1817–1825. https://doi.org/10.1038/ajg.2012.332
Parikh MP, Gupta NM, Sanaka MR (2019) Esophageal third space endoscopy: recent advances. Curr Treat Opt Gastroenterol. https://doi.org/10.1007/s11938-019-00217-6
Raja S, Murthy SC, Tang A et al (2018) Per Oral Endoscopic Myotomy (POEM): another tool in the toolbox. J Thorac Cardiovasc Surg. https://doi.org/10.1016/j.jtcvs.2018.11.132
von Renteln D, Inoue H, Minami H et al (2012) Peroral endoscopic myotomy for the treatment of achalasia: a prospective single center study. Am J Gastroenterol 107(3):411–417. https://doi.org/10.1038/ajg.2011.388
Ngamruengphong S, Inoue H, Ujiki MB et al (2017) Efficacy and safety of peroral endoscopic myotomy for treatment of achalasia after failed heller myotomy. Clin Gastroenterol Hepatol 15(10):1531–1537.e3. https://doi.org/10.1016/j.cgh.2017.01.031
Wu QN, Xu XY, Zhang XC et al (2017) Submucosal fibrosis in Achalasia patients is a rare cause of aborted peroral endoscopic myotomy procedures. Endoscopy 49(8):736–744. https://doi.org/10.1055/s-0043-113440
Liu X-Y, Cheng J, Chen W-F et al (2020) A risk-scoring system to predict clinical failure for patients with achalasia after peroral endoscopic myotomy. Gastrointest Endosc 91(1):33–40.e1. https://doi.org/10.1016/j.gie.2019.07.036
Tang X, Gong W, Deng Z et al (2017) Feasibility and safety of peroral endoscopic myotomy for achalasia after failed endoscopic interventions. Dis Esophagus 30(3):1–6. https://doi.org/10.1111/dote.12457
Nabi Z, Ramchandani M, Chavan R et al (2018) Peroral endoscopic myotomy in treatment-naïve achalasia patients versus prior treatment failure cases. Endoscopy 50(4):358–370. https://doi.org/10.1055/s-0043-121632
Jones EL, Meara MP, Pittman MR, Hazey JW, Perry KA (2016) Prior treatment does not influence the performance or early outcome of per-oral endoscopic myotomy for achalasia. Surg Endosc 30(4):1282–1286. https://doi.org/10.1007/s00464-015-4339-y
Orenstein SB, Raigani S, Wu YV et al (2015) Peroral endoscopic myotomy (POEM) leads to similar results in patients with and without prior endoscopic or surgical therapy. Surg Endosc 29(5):1064–1070. https://doi.org/10.1007/s00464-014-3782-5
Sharata A, Kurian AA, Dunst CM, Bhayani NH, Reavis KM, Swanström LL (2013) Peroral endoscopic myotomy (POEM) is safe and effective in the setting of prior endoscopic intervention. J Gastrointest Surg 17(7):1188–1192. https://doi.org/10.1007/s11605-013-2193-6
Kahrilas PJ, Bredenoord AJ, Fox M et al (2015) The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil. 27(2):160–174. https://doi.org/10.1111/nmo.12477
Guardino JM, Vela MF, Connor JT, Richter JE (2019) Pneumatic dilation for the treatment of achalasia in untreated patients and patients with failed Heller myotomy. J Clin Gastroenterol 38(10):855–860
Sanaka MR, Thota PN, Parikh MP et al (2018) Peroral endoscopic myotomy leads to higher rates of abnormal esophageal acid exposure than laparoscopic Heller myotomy in achalasia. Surg Endosc. https://doi.org/10.1007/s00464-018-6522-4
Kumbhari V, Familiari P, Bjerregaard N et al (2017) Gastroesophageal reflux after peroral endoscopic myotomy: a multicenter case–control study. Endoscopy 49(07):634–642. https://doi.org/10.1055/s-0043-105485
Repici A, Fuccio L, Maselli R et al (2018) GERD after per-oral endoscopic myotomy as compared with Heller’s myotomy with fundoplication: a systematic review with meta-analysis. Gastrointest Endosc 87(4):934–943.e18. https://doi.org/10.1016/j.gie.2017.10.022
Acknowledgements
This study was presented in the abstract form at the annual scientific meeting of the American College of Gastroenterology at Philadelphia, PA, USA in October 2018.
Funding
No financial support.
Author information
Authors and Affiliations
Contributions
All authors have contributed to and approved the final version of the manuscript. All authors studied the concept and design of the study. RL performed the data analysis. All authors interpreted the results. GK and MP drafted the manuscript. All authors participated in critical revision of final of the manuscript.
Corresponding author
Ethics declarations
Disclosure
Dr. Sanaka, Dr. Khoudari, Dr. Parikh, Dr. Thota, Ms. Lopez, Dr. Gupta, Dr. Gabbard, Dr. Ray, Dr. Murthy, and Dr. Raja have no conflicts of interest and nothing to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sanaka, M.R., Khoudari, G., Parikh, M. et al. Peroral endoscopic myotomy is highly effective for achalasia patients with recurrent symptoms after pneumatic dilatation. Surg Endosc 35, 2965–2975 (2021). https://doi.org/10.1007/s00464-020-07737-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-07737-8