
Abstract
Background
Surgical treatment for low rectal cancer septic complications often requires an ileostomy for fecal diversion. Delayed coloanal anastomosis (CAA) has been performed for several years to reduce septic complications and to avoid ileostomy. The aim of this study was to report the technical, functional and oncological results of delayed CAA in patients operated on for low rectal cancer focusing on pelvic septic complications.
Methods
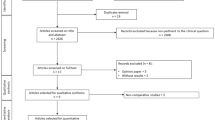
All consecutive patients operated on for low rectal cancer suitable for total mesorectal excision and two-step delayed CAA at a single institution between May 2000 and September 2013 were included in the study. Patients’ characteristics, operative and postoperative outcomes, long-term technical, functional and oncological results from a prospectively maintained database, were retrospectively analyzed.
Results
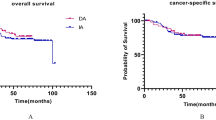
A total of 85 consecutive patients (69 men), of median age 63 years (range 42–83 years) were included. Median delay between the first and the second step of the operation was 6 days (range 2–13 days). Twenty-one patients (25%) developed pelvic sepsis, nine of them (10.6%) developed an anastomotic leak. Twenty-three patients had a definitive stoma at the end of follow-up. Seventeen patients (29%) experienced a poor functional result. Thirty-three patients (38%) presented with recurrence at a median follow-up of 59 months (range 12–135 months). Seven (8.2%) developed a local recurrence, 18 a distant metastasis (21.1%) and 8 (9.4%) both a local and distant recurrence.
Conclusions
In our series, laparoscopic total mesorectal excision with delayed coloanal anastomosis was associated with septic complications and oncologic results similar to those reported after total mesorectal excision with conventional anastomosis and ileostomy, nearly one-third of patients experience a poor functional result. A randomized trial comparing these two options for low rectal cancer is under way.



Similar content being viewed by others

References
Heald RJ, Ryall RDH (1986) Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 327:1479–1482
Nesbakken A, Nygaard K, Lunde OC (2001) Outcome and late functional results after anastomosis leakage following mesorectal excision for rectal cancer. Br J Surg 88:400–404
Eriksen MT, Wibe A, Norstein J, Haffner J, Wiig JN (2005) Anastomotic leakage following routine mesorectal excision for rectal cancer in a national cohort of patients. Colorectal Dis 7:51–57
Longo WE, Virgo KS, Johnson FE et al (1998) Outcome after proctectomy for rectal cancer in Department of Veterans Affairs Hospitals: a report from the National Surgical Quality Improvement Program. Ann Surg 228:64–70
Bell SW, Walker KG, Rickard MJ et al (2003) Anastomotic leakage after curative anterior resection results in a higher prevalence of local recurrence. Br J Surg 90:1261–1266
Walker KG, Bell SW, Rickard MJ et al (2004) Anastomotic leakage is predictive of diminished survival after potentially curative resection for colorectal cancer. Ann Surg 240:255–259
Edwards DP, Leppington-Clarke A, Sexton R, Heald RJ, Moran BJ (2001) Stoma-related complications are more frequent after transverse colostomy than loop ileostomy: a prospective randomized clinical trial. Br J Surg 88:360–363
Law WL, Chu KW, Choi HK (2002) Randomized clinical trial comparing loop ileostomy and loop transverse colostomy for faecal diversion following total mesorectal excision. Br J Surg 89:704–708
Gessler B, Haglind E, Angenete E (2012) Loop ileostomies in colorectal cancer patients—morbidity and risk factors for non reversal. J Surg Res 178:708–714
Sharma A, Deeb AP, Rickles AS, Iannuzzi JC, Monson JR, Fleming SJ (2013) Closure of defunctioning loop ileostomy is associated with considerable morbidity. Colorectal Dis 15:458–462
Musters GD, Atema JJ, van Westreenen HL, Buskens CJ, Bemelman WA, Tanis PJ (2016) Ileostomy closure by colorectal surgeons results in less major morbidity: results from an institutional change in practice and awareness. Int J Colorectal Dis 31:661–667
Man VC, Choi HK, Law WL, Foo DC (2016) Morbidities after closure of ileostomy: analysis of risk factors. Int J Colorectal Dis 31:51–57
Danielsen AK, Park J, Jansen JE et al (2017) Early closure of a temporary ileostomy in patients with rectal cancer: a multicenter randomized controlled trial. Ann Surg 265:284–290
Biondo S, Trenti L, Galvez A et al (2017) Two-stage Turnbull–Cutait pull-through coloanal anastomosis versus coloanal anastomosis with protective loop ileostomy for low rectal cancer. Protocol for a randomized controlled trial. Int J Colorectal Dis 32:1357–1362
Turnbull RB (1966) Pull-through resection of the rectum, with delayed anastomosis, for cancer or Hirschsprung’s disease. Surgery 59:498–502
Cutait DE, Cutait RMD, Ioshimoto MMD, Da Silva JHMD, Manzione AMD (1985) Abdominoperineal endoanal pull-through resection: a comparative study between immediate and delayed colorectal anastomosis. Dis Colon Rectum 28:294–299
Hallet J, Milot H, Drolet S, Desrosiers E, Gregoire RC, Bouchard A (2014) The clinical results of the Turnbull–Cutait delayed coloanal anastomosis: a systematic review. Tech Coloproctol 18:579–590
Olagne E, Baulieux J, de la Roche E et al (2000) Functional results of delayed coloanal anastomosis after preoperative radiotherapy for lower third rectal cancer. J Am Coll Surg 191:643–649
Jarry J, Faucheron JL, Moreno W, Bellera CA, Evrard S (2011) Delayed colo-anal anastomosis is an alternative to prophylactic diverting stoma after total mesorectal excision for middle and low rectal carcinomas. Eur J Surg Oncol 37:127–133
Remzi FH, El Gazzaz G, Kiran RP, Kirat HT, Fazio VW (2009) Outcomes following Turnbull–Cutait abdominoperineal pull-through compared with coloanal anastomosis. Br J Surg 96:424–429
Bianco F, Belli A, De Franciscis S et al (2016) “Scarless” and no-stoma surgery for low rectal cancer: the laparoscopic pull-through delayed “high” colo-anal anastomosis. Update Surg 68:99–104
Xiong Y, Huang P, Ren QG (2016) Transanal pull-through procedure with delayed versus immediate coloanal anastomosis for anus-preserving curative resection of lower rectal cancer: a case-control study. Am Surg 82:533–539
Jarry J, Faucheron JL (2011) Laparoscopic rectosigmoid resection with transanal colonic pull-through and delayed coloanal anastomosis: a new approach to adult Hirschsprung disease. Dis Colon Rectum 54:1313–1319
Fixot K, Galifet M, Scherrer ML et al (2014) Abdominoperineal pull-through resection with delayed coloanal anastomosis as treatment option for complex recto-urinary fistulas. Int J Colorectal Dis 29:407–409
Patsouras D, Yassin NA, Phillips RK (2014) Clinical outcomes of colo-anal pull-through procedure for complex rectal conditions. Colorectal Dis 16:253–258
Denost Q, Rouanet P, Faucheron JL et al (2017) To drain or not to drain infraperitoneal anastomosis after rectal excision for cancer: the GRECCAR 5 randomized trial. Ann Surg 265:474–480
Rahbari NN, Weitz J, Hohenberger W et al (2010) Definition and grading of anastomotic leakage following anterior resection of the rectum: a proposal by the International Study Group of Rectal Cancer. Surgery 147:339–351
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–212
Jorge JM, Wexner SD (1993) Etiology and management of fecal incontinence. Dis Colon Rectum 36:77–97
McCulloch P, Altman DG, Campbell WB et al (2009) No surgical innovation without evaluation: the IDEAL recommendations. Lancet 374:1105–1112
Mattiessen P, Hallböök O, Rutegård J, Simert G, Sjödahl R (2007) Defunctioning stoma reduces symptomatic anastomotic leakage after low anterior resection of the rectum for cancer. Ann Surg 246:207–214
Peeters KC, Tollenaar RA, Marijnen CA et al (2005) Risk factors for anastomotic failure after total mesorectal excision of rectal cancer. Br J Surg 92:211–216
Paun BC, Cassie S, MacLean AR, Dixon E, Buie WD (2010) Postoperative complications following surgery for rectal cancer. Ann Surg 251:807–818
Bertelsen CA, Andreasen AH, Jørgensen T, On Behalf of the Danish Colorectal Cancer Group et al (2010) Anastomotic leakage after curative anterior resection for rectal cancer: short and long term outcome. Colorectal Dis 12:e76–e81
Snidjers HS, Van den Broek CBM, Wouters MWJM et al (2013) An increasing use of defunctioning stoma after low anterior resection for rectal cancer. Is it the way to go? Eur J Surg Oncol 39:715–720
Jayne DG, Guillou PJ, Thorpe H et al (2007) Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol 25:3061–3068
Laurent C, Leblanc F, Wütrich P et al (2009) Laparoscopic versus open surgery for rectal cancer: long-term oncologic results. Ann Surg 250:54–61
Lujan J, Valero G, Hernandez Q et al (2009) Randomized clinical trial comparing laparoscopic and open surgery in patients with rectal cancer. Br J Surg 96:982–989
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed consent
For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Sage, PY., Trilling, B., Waroquet, PA. et al. Laparoscopic delayed coloanal anastomosis without diverting ileostomy for low rectal cancer surgery: 85 consecutive patients from a single institution. Tech Coloproctol 22, 511–518 (2018). https://doi.org/10.1007/s10151-018-1813-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-018-1813-2