
Abstract
Purpose of Review
Breath testing for fungal respiratory infections has great promise as samples can be obtained by non-invasive, repeatable techniques that can be done on a wide range of patients including children, the confused and from those in the intensive care unit (ICU). We have reviewed progress toward development of test applicable to clinical practice.
Recent Findings
Many volatile organic compounds (VOCs) have been identified, especially from key pathogens such as Aspergillus fumigatus, but very few clinical trials have been performed. The most convincing of these demonstrated that Aspergillus species could be identified by gas chromatography with mass spectrometry in breath samples of at risk patients with high sensitivity (94%) and specificity (93%) compared with the European Organization for Research and Treatment of Cancer/Mycosis Study Group (EORTC/MSG) gold standard.
Summary
Significant progress has been made but further studies are needed to validate these recent findings and identify VOCs from other pathogenic fungi using GC-MS, and clinical trials performed using faster and less demanding analytic platforms that could be used in clinical laboratories.
Similar content being viewed by others


Introduction
Invasive filamentous fungal infections are uncommon but may cause acute, severe, life-threatening infections in the immune-compromised host. Aspergillus fumigatus is the most common mould infection worldwide in neutropenic patients, in whom the incidence parallels the duration and severity of the neutropenia, and solid organ transplant recipients, particularly lung and heart-lung transplant recipients [1,2,3,4,5]. Invasive aspergillosis (IA) also occurs in a wide range of other non-neutropenic hosts who have other forms of immune suppression including AIDS, the critically illness in intensive care units (ICU), steroid use, multiple previous antibiotic regimens, renal or hepatic failure and diabetes. Many cases in ICU follow an episode of sepsis, probably due to so-called immunoparalysis [5,6,7, 8••]. Invasive fungal disease (IFD) is very uncommon in the non-suppressed host but can cause chronic IA in patients with comorbidities such as chronic lung disease (e.g. previous tuberculosis cavities) especially with concurrent steroid therapy and aspergillus bronchitis can be seen in those with cystic fibrosis (CF), bronchiectasis [8••, 9,10,11]. IA is not increased in patients with rheumatic disease treated with biologic therapies [12].
A. fumigatus causes about 60% of all mould infection in haemopoietic stem cell transplant recipients [2]. The rest of the Aspergillus infections are made up of similar proportions of Aspergillus flavus, Aspergillus niger, Aspergillus terreus and unspecified Aspergillus infections. Mixed infections due to two Aspergillus species occurred in 12% of cases and were seen almost exclusively among patients with pulmonary aspergillosis. In solid organ transplants (heart-lung transplant, kidney, liver and small bowel), A. fumigatus is the most commonly reported species identified, with infections due to A. flavus, A. niger and A. terreus less common [2, 3].
Zygomycosis, fusariosis, phaeohyphomycosis and other moulds constituted approximately 30% of mould infections in haemopoietic stem cell transplant recipients and 20% of mould infection in solid organ transplants [2, 3, 13, 14]. Zygomycetes including mucormycosis were more common in lung transplants compared with other solid organ transplants. Early infections (those occurring <90 days after transplantation) were dominated by IA with non-Aspergillus mould infection occurring later.
Treatment and prophylaxis have improved for mould infections but nevertheless the associated mortality rates remain high (25–58%) [1,2,3,4,5,6,7, 8••, 13, 14]. In a recent study, overall 1-year survival among the haematopoietic stem cell transplantation (HSCT) cohort was the lowest for patients with Fusarium infections (6.3%) but still poor for patients with aspergillosis (25.4%) and zygomycosis (28.0%) [2]. In solid organ transplants, the 12-month survival after infection was 59% for patients with IA, 61% for infections due to non-Aspergillus moulds [3].
The poor outcome is in part due to diagnostic delay, particularly in the neutropenic host in whom rapid progression, angioinvasion and subsequent dissemination occurs [8••]. The diagnostic difficulty arises because the symptoms, signs and radiological features may be sensitive but are relatively non-specific and can represent other disease processes such as pulmonary haemorrhage, organising pneumonia or bacterial infection. The traditional approach is to perform sputum cultures, or obtain specimens by bronchoalveolar lavage (BAL), or transbronchial or percutaneous biopsy. Unfortunately, these tests also lack sensitivity although cultures from a normally sterile site are highly specific if positive. Specimens take a few days for processing, and harvesting specimens may be hazardous or contraindicated because of the risks of bleeding or pneumothorax in severely unwell patients, those with pre-existing lung disease or the effects chemotherapy. Delays in a specific diagnosis is associated with poorer outcomes and unnecessary exposure, toxicity and costs from empiric therapy.
Because of the diagnostic challenges, new diagnostic tests have been evaluated and lead to some improvements, particularly the galactomannan assay (GM). This was designed to be used on serum and does not perform well on single samples. The performance is better when high-risk patients such as those with acute myeloid leukaemia are monitored serially but meta-analyses have not demonstrated that this leads to earlier diagnosis [15]. The GM assay performs less well in non-neutropenic patients presumably because there is less angioinvasion and a lower chance of antigen reaching the blood stream. The GM assay performs best when done of BAL fluid samples, when it is sufficiently accurate to rule out IA [15]. Unfortunately, this still requires a BAL and does not rule out non-Aspergillus infections. Nucleic acid testing has lacked standardised methods and despite meticulous laboratory techniques, the potential for contamination for ubiquitous fungal contamination remains [16, 17]. There is a real need for a new test which can rule in or out fungal infections in the immunocompromised patient group.
Potential and Pitfalls of Volatile Organic Compound Detection for Diagnosis of Fungal Infection
The primary goal for any diagnostic test is that it should have a sufficiently high sensitivity and specificity to confirm or exclude a diagnosis. This is dependent on the pre-test probability of a positive result. In the acute setting, such as HSCT infection, where fungal infections are relatively uncommon, rapidly progressive, life threatening, and fungal colonisation is unlikely, the requirements are different from a chronic condition where colonisation is common making a false positive test more likely. For example, A. fumigatus colonisation is common in chronic lung disease and has been reported to be between 6 and 58% in patients with CF but Aspergillus bronchitis is less common, but important as it may contribute to the development of bronchiectasis. The ideal test in these circumstances would be able to distinguish between colonisation and invasion with minimal false positive results. This would require differential expression genes required for invasion and VOC production which may occur but is yet to be explored. Other problems affecting the specificity are contamination of equipment, occurrence of VOC’s in ambient air, smoking in the subject and recent food consumption. Detection of a breath print may be more robust than identification of a single target VOC in some circumstances but ultimately, the value of a test depends on the accuracy as determined in well-conducted clinical trials [18].
Volatiles Produced by Invasive Moulds Causing Human Disease
VOCs are carbon-based compounds that readily enter the gas phase, vaporising at 0.01 kPa at 20 °C [19]. Over 1000 volatile organic compounds have been described that originate from a wide range of bacterial and fungal genera and species [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39]. Fungal VOCs detected to date are mainly alcohols, benzenoids, aldehydes, alkenes, acids, esters and ketones and are derived from primary and secondary metabolism pathways [19, 21]. The released volatiles can serve as signalling molecules (semiochemicals) that functions as attractants and deterrents to insects and other invertebrates, and bacteria [19].
Scores of VOC’s have been described in the headspace of cultures of A. fumigatus alone. A comprehensive list would be very long and exceed the list of over 300 VOC’s reported by Siddiquee et al. for A. niger alone [22••]. Volatile production from any microorganism can change when elements of the environment are changed, for example differing oxygen tension, moisture, pH and growth media [20, 23•]. Co-culturing fungi with bacteria such as Pseudomonas aeruginosa results in the release of further differing volatiles as a response to growth in the presence of another microorganism [24]. This creates a potential for VOC’s from a pathogen to change with the local microbiological environment which may occur in mixed infection such as in CF or ventilator-associated pneumonia in the ICU.
To date, there are no reports on volatiles released from Zygomycetes or Phaeohyphomycetes and is an unexplored area. Therefore, whether the detection of VOCs produced by these organisms in patients will help in the diagnosis of mucormycosis is unknown [40].
Platforms
Not only are large numbers of VOC’s produced by fungal species but the human breath contains 2000–3000 VOC’s derived from human metabolism and metabolism of the microbiome. Because of the complexity of potential targets, investigators have used various strategies to determine possible targets. In many cases, a biological approach to identification of VOC’s in the headspace of fungal cultures has been used [41, 42]. Cultures with media that most closely resembles the infecting site are preferable to identify possible diagnostics targets. Others have used an empiric approach comparing VOC’s in breath of infected with those of non-infected subjects [43]. To minimise contamination from the upper airways, various strategies have been adopted. These include using changes in pressure and CO2 concentrations to trigger pumps to capture alveolar gas, nasal sampling to avoid mouth contamination and confining targets to those thought to be only produced by a particular pathogen [41, 44].
Electronic Nose
Electronic noses (eNose) were developed to mimic the mammalian olfactory system and work on the basis of identifying a complex mixture of volatiles within one sample [45]. They are typically composed of an information-processing unit such as an artificial neural network, software that has digital pattern-recognition algorithms, and a cross-referencing library [46]. When sampling a gas, the response from the eNose is due to the pattern of an overall response of a sensor array that defines a chemical fingerprint of a particular VOC [47]. Advantages of the eNose are that it can produce rapid results less expensively than other analytical instruments, and is easy to operate. However, temperature and humidity can cause negative effects on sampling and there can be reproducibility issues alongside interference with other gases [48].
Selective Ion Flow Tube Mass Spectrometry
Selective ion flow tube mass spectrometry (SIFT-MS) uses soft chemical ionisation which is coupled to mass spectrometric detection and gives real-time analytic results. It relies on chemical ionisation of the trace gas molecules in air/breath samples introduced into helium gas using precursor ions [49]. Online breath monitoring is a major advantage over GC-MS; however, sensitivity can be an issue and overall SIFT-MS is less sensitive than GC-MS analysis.
Secondary Electrospray Ionization-Mass Spectrometry
Secondary electrospray ionization-mass spectrometry (SESI-MS) rapidly detects volatile compounds without the need for pre-treatment. SESI occurs by proton transfer reactions between the electrospray solution and the volatile analyte not unlike traditional electrospray ionization (ESI). However, unlike standard ESI, the proton transfer process of SESI occurs in the vapour and as such makes SESI best suited for detecting organic volatiles [50]. Using SESI-MS, Zhu et al. collected the mass spectra of the headspace volatiles produced by four genera of bacteria, represented by P. aeruginosa, Staphylococcus aureus, Escherichia coli and Salmonella typhimurium [51].
Gas Chromatography Coupled with Mass Spectrometry
Gas chromatography coupled with mass spectrometry (GC-MS) is a sensitive technique for the detection of volatiles in very low concentrations. It allows for the structural determination of unknown compounds by matching their spectra with reference spectra and/or a reference standard. Depending on the volatile in question, either electron impact (EI) or the softer chemical ionisation (CI) can be used. While GC-MS is very sensitive, its main limitation is that samples need to be run by a trained highly skilled operator and is not portable.
In Vitro Studies of Volatile Organic Compounds Produced by Fungal Species
Electronic Nose
The eNose has been shown to quickly and reliably discriminate between the VOC's found the headspace of cultures of a single strain of the 10 commonest causes of ventilator-associated pneumonia including nine bacterial species and A. fumigatus. Unfortunately, there is no systematic study of clinically relevant fungal species, but this technique precludes identification of the VOC’s detected [42].
Selective Ion Flow Tube Mass Spectrometry
The capabilities of SIFT-MS have been extensively reviewed by Smith et al. [52]. Limited studies have been performed in vitro on bacterial and fungal metabolites [53]. The major paper describes the headspace VOC’s produced by clinical strains of A. fumigatus inoculated into brain heart infusion broth and incubated at 37 °C and analysed after 24, 48 and 72 h [54]. Principal component analysis of the headspace showed that multiple small VOC’s were detectable and commonly seen with bacterial cultures; together with a distinctive appearance of the organosulfur compounds methanethiol, dimethyl sulphide (DMS) and dimethyl disulphide (DMDS) reach their maximum headspace concentration, after 48 h of culture. These compounds were also seen in co-cultures studies with S. aureus and Streptococcus pneumoniae, but are not unique to fungal species.
Secondary Electrospray Ionization-Mass Spectrometry
This technique is very promising and has been shown to be successful in distinguishing multiple bacterial species as a combination of VOCs creates a unique pattern for each genus. In addition, principal component analysis (PCA) has been applied for the purpose of species or serovar discrimination. These profiles may be independent of the growth medium of the organism. This technique may be applicable to detection of VOC’s produced by fungi that cause human disease but we are unaware of any data on these organisms [55].
Gas Chromatography with Mass Spectrometry
Multiple studies from environmental research groups have demonstrated a range of VOCs produced by medically and environmentally important fungal species cultured on a variety of substrates have identified a large array of metabolites. Some such as as 2-pentylfuran, have been investigated as potential breath markers but this has been found unsuitable as it is produced by spontaneous breakdown of lineloic acid, is found in food and may be found in environmental air samples [44, 56, 57]. Sesquiterpenes have been identified in several studies although a major metabolite, β-trans-bergamotene, was initially misidentified as β-farnesene in these studies, because of the similarity in fragmentation patterns and the absence of β-trans-bergamotene from the National Institute of Standards and Technology (NIST) library [58,59,60]. However, VOC’s have not been studied systematically for all the species that cause disease in humans, in particular the Zygomycetes, Fusarium species and Scedosporium species.
Clinical Diagnostics Studies of VOC’s
Electronic Nose
The success of intro studies have lead investigators to perform clinical studies of ventilator-associated pneumonia (VAP) but the technique lacked sufficient sensitivity and specificity for a confident diagnosis of VAP to be made (sensitivity was 88% with a specificity of 66%) [43].
The eNose have also been used as a platform for the diagnosis of invasive fungal infections in two prospective proofs of concept studies. In the first of these, 27 patients with CF attending a routine outpatient appointment had breath samples and sputum samples taken and the results of eNose and cultures compared. Of these, nine patients were colonised by A. fumigatus and three misclassified by cross validation. The sensitivity was 78% and specificity 94% [61••]. In the second study, 46 patients who were at risk of prolonged severe neutropenia for more than 7 days from chemotherapy administered for a haematological malignancy (stem cell transplant or induction/consolidation treatment for acute myeloid leukaemia) were enrolled [62••]. Of these, five were diagnosed as probable or proven aspergillosis and five had IA excluded according to the EORTC/MSG criteria. Possible IA was excluded from the analysis. The cross-validated accuracy of the eNose in diagnosing IA was 90.9% (sensitivity, 100%; specificity, 83.3%). The correlation between the discriminant scores and BAL fluid GM levels, currently the most accurate single test to diagnose invasive pulmonary aspergillosis, was not statistically significant. These preliminary data indicate a distinct exhaled VOC profile that can be detected with eNose technology and the diagnostic accuracy of the eNose for IA warrants validation.
These studies have two major limitations. The first is its small size and the second is that eNose technology does not allow identification of the individual VOCs that drive the signal. The first of these concerns can be addressed by large well-conducted clinical trials, and the second by studies run in parallel with other techniques such as GC-MS.
Selective Ion Flow Tube Mass Spectrometry
SIFT-MS has been used to detect H2S and HCN used in ICU studies, but we are unaware of any studies designed to detect fungal infections in these patients.
Secondary Electrospray Ionization-Mass Spectrometry
We are unaware of any relevant clinical trials using this technique.
Gas Chromatography with Mass Spectrometry
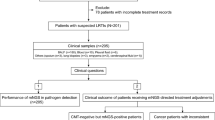
Early clinical studies suggested that 2-pentylfuran might serve as an appropriate target but environmental contamination and spontaneous production from food and inconsistent results made this an unsuitable diagnostic target. It does however illustrate the potential hazards associated with using VOC’s for diagnosis that may only become apparent during clinical trials [27, 56, 57]. The most compelling study performed thus far is reported by Koo et al. [41]. Following the studies performed to identify markers of four Aspergillus species, in the headspace of cultures, they conducted a prospective study of 64 consecutive immune-compromised oncology, transplant and infectious diseases patients who were at risk of IA. The results of breath testing were compared with those of the EORTC/MSG consensus criteria. Most of the patients had received mould active antifungal therapy (mean 2, IQR 1–13 days). The results are instructive firstly because the overall results were encouraging as a secondary metabolite signature distinguished patients with IA from patients with other IFD or other pneumonia with 94% (95% CI 81–98%) sensitivity and 93% (95% CI 79–98%) specificity against the reference standard of proven or probable IA. Secondly, a four-metabolite signature indicating the presence of IA was not predictable from the in vitro results. This consisted of the volatile sesquiterpenes β-trans-bergamotene and α-trans-bergamotene that were found in the in vitro cultures, and two closely related metabolites that were not seen in in vitro cultures—the terpenoid ketone trans-geranylacetone and a β-vatirenene-like sesquiterpene. This breath metabolite signature correctly identified all 31 of 32 classified as having IA from A. fumigatus. They also identified a novel sesquiterpene, not present in the headspace of in vitro cultures, in the breath of a patient with A. niger present in multiple respiratory samples and an elevated serum galactomannan. This is presumably the results of fungal growth in the lung environment and does not seem to be the result of some exposure to anti-mould treatment. The concentrations of the key metabolites β-trans-bergamotene and trans-geranylactone were quite high in each breath sample (> 2ppm), which should be detectable by other less sensitive techniques. Thirdly, monoterpenes that were produced in vitro by Aspergillus species were present in samples from all patients, although not in the ambient air controls. The origin of these is not clear.
Possible Role for Monitoring Therapy
There is also a potential role for using breath testing to monitoring response to antifungal therapy. Currently, the duration of treatment is reliant on clinical judgement which takes into account resolution of radiological signs and reduction in immune suppression. Both of these are difficult to quantitate and clinical caution often leads to prolonged courses of treatment with expensive agent that may cause significant drug interactions and adverse effects. A preliminary study demonstrated SIFT-MS showed changes in non-specific VOC production by A. fumigatus on incubation with benomyl and tebuconazole. Similarly, Koo et al. found that exposure of A. fumigatus hyphae to antifungal drugs in vitro, modulated VOC production, particularly sesquiterpenes [41]. Within 12 h of exposure to micafungin, β-trans-bergamotene increased 10-fold and 3-fold after amphotericin exposure. There was near-complete attenuation of all volatile metabolites by 36 h. Voriconazole reduced monoterpene and sesquiterpene production by 12 h, with attenuation of all volatile metabolites after 36-h exposure. They also reported that there was a mean exposure to active antimould treatment in 75% of subjects with mould infections for a median of 2 days (IQR 2–11 days) which did not appear to inhibit VOC production suggesting activity may be different in vivo [41]. These initial observations need to be studied further.
Conclusion
There is a need for improved diagnostics particularly for fungal infections in the neutropenic or severely immune-compromised host and breath testing for VOC’s is very promising. The basic approach of using a biologically driven investigation to identify appropriate VOC targets in vitro that can be identified by various platforms may be the most fruitful way forward. However, more clinical trials are urgently needed, and before VOC detection can be widely adopted, a diagnostic platform that can be widely available in clinical laboratories needs to be developed to take advantage of the repeatable, minimally invasive technique and highly acceptable techniques that VOC testing offers.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Hammond SP, Marty FM, Bryar JM, DeAngelo DJ, Baden LR. Invasive fungal disease in patients treated for newly diagnosed acute leukemia. Am J Hematol. 2010;85(9):695–9. doi:10.1002/ajh.21776.
Kontoyiannis DP, Marr KA, Park BJ, Alexander BD, Anaissie EJ, Walsh TJ, et al. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin Infect Dis. 2010;50(8):1091–100. doi:10.1086/651263.
Pappas PG, Alexander BD, Andes DR, Hadley S, Kauffman CA, Freifeld A, et al. Invasive fungal infections among organ transplant recipients: results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin Infect Dis. 2010;50(8):1101–11. doi:10.1086/651262.
Neofytos D, Horn D, Anaissie E, Steinbach W, Olyaei A, Fishman J, et al. Epidemiology and outcome of invasive fungal infection in adult hematopoietic stem cell transplant recipients: analysis of Multicenter Prospective Antifungal Therapy (PATH) Alliance Registry. Clin Infect Dis. 2009;48:265–73. doi:10.1086/595846. Erratum in: Clin Infect Dis. 2009;48(5):690
Segal BH. Aspergillosis. N Engl J Med. 2009;360(18):1870–84. doi:10.1056/NEJMra0808853.
Bassetti M, Garnacho-Montero J, Calandra T, Kullberg B, Dimopoulos G, Azoulay E, et al. Intensive care medicine research agenda on invasive fungal infection in critically ill patients. Intensive Care Med. 2017 Mar 2; doi:10.1007/s00134-017-4731-2.
Baddley JW, Stephens JM, Ji X, Gao X, Schlamm HT, Tarallo M. Aspergillosis in intensive care unit (ICU) patients: epidemiology and economic outcomes. BMC Infect Dis. 2013;13:29. doi:10.1186/1471-2334-13-29.
•• Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015;70(3):270–7. doi:10.1136/thoraxjnl-2014-206291. Provides an excellent overview of the epidemiology and pathogenesis of A. fumigatus infections.
Armstead J, Morris J, Denning DW. Multi-country estimate of different manifestations of aspergillosis in cystic fibrosis. PLoS One. 2014;9(6):e98502. doi:10.1371/journal.pone.0098502.
Chrdle A, Mustakim S, Bright-Thomas RJ, Baxter CG, Felton T, Denning DW. Aspergillus bronchitis without significant immunocompromise. Ann N Y Acad Sci. 2012;1272:73–85.
Guo YL, Chen YQ, Wang K, Qin SM, Wu C, Kong JL. Accuracy of BAL galactomannan in diagnosing invasive aspergillosis: a bivariate metaanalysis and systematic review. Chest. 2010 Oct;138(4):817–24. doi:10.1378/chest.10-0488.
Kourbeti IS, Ziakas PD, Mylonakis E. Biologic therapies in rheumatoid arthritis and the risk of opportunistic infections: a meta-analysis. Clin Infect Dis. 2014;58(12):1649–57. doi:10.1093/cid/ciu185.
McCarty TP, Baddley JW, Walsh TJ, Alexander BD, Kontoyiannis DP, Perl TM, et al., TRANSNET investigators. Phaeohyphomycosis in transplant recipients: results from the Transplant Associated Infection Aurveillance Network (TRANSNET). Med Mycol. 2015;53(5):440–6. doi:10.1093/mmy/myv018.
Lin SJ, Schranz J, Teutsch SM. Aspergillosis case-fatality rate: systematic review of the literature. Clin Infect Dis. 2001 Feb 1;32(3):358–66.
Harrison E, Stalhberger T, Whelan R, Sugrue M, Wingard JR, Alexander BD, et al. Aspergillus DNA contamination in blood collection tubes. Diagn Microbiol Infect Dis. 2010;67(4):392–4. doi:10.1016/j.diagmicrobio.2010.02.028.
Mengoli C, Cruciani M, Barnes RA, Loeffler J, Donnelly JP. Use of PCR for diagnosis of invasive aspergillosis: systematic review and meta-analysis. Lancet Infect Dis. 2009 Feb;9(2):89–96. doi:10.1016/S1473-3099(09)70019-2.
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig LM, et al. Standards for reporting of diagnostic accuracy. The STARD statement for reporting studies of diagnostic accuracy: explanation and elaboration. Ann Intern Med. 2003 Jan 7;138(1):W1–12.
Morath S, Hung R, Bennet J. Fungal volatile organic compounds: a review with emphasis on their biotechnological potential. Fungal Biol Rev. 2012;26:73–83.
Schmidt R, Cordovez V, de Boer W, Raaijmakers J, Garbeva P. Volatile affairs in microbial interactions. ISME J. 2015;9(11):2329–35. doi:10.1038/ismej.2015.42.
Piechulla B, Degenhardt J. The emerging importance of microbial volatile organic compounds. Plant Cell Environ. 2014;37(4):811–2. doi:10.1111/pce.12254.
Siddiquee S, Al Azad S, Bakar FA, Naher L, Kumar SV. Separation and identification of hydrocarbons and other volatile compounds from cultures of Aspergillus niger by GC–MS using two different capillary columns and solvents. J Saudi Chem Soc. 2015;19(3):243–56.
•• Heddergott C, Calvo AM, Latgé JP. The volatome of Aspergillus fumigatus. Eukaryot Cell. 2014;13(8):1014–25. doi:10.1128/EC.00074-14. This is an interesting review of the VOCs produced by A. fumigatus.
• Neerincx AH, Geurts BP, Habets MF, Booij JA, van Loon J, Jansen JJ, et al. Identification of Pseudomonas aeruginosa and Aspergillus fumigatus mono- and co-cultures based on volatile biomarker combinations. J Breath Res. 2016;10(1):016002. doi:10.1088/1752-7155/10/1/016002. This paper provides data on VOCs in co cultures that may occur in cystic fibrosis or bronchiectasis or ventilator-associated pneumonia.
Matysik S, Herbarth O, Mueller A. Determination of volatile metabolites originating from mould growth on wall paper and synthetic media. J Microbiol Methods. 2008;75(2):182–7. doi:10.1016/j.mimet.2008.05.027.
Fischer G, Schwalbe R, Möller M, Ostrowski R, Dott W. Species-specific production of microbial volatile organic compounds (MVOC) by airborne fungi from a compost facility. Chemosphere. 1999;39(5):795–810.
Syhre M, Scotter JM, Chambers ST. Investigation into the production of 2-pentylfuran by Aspergillus fumigatus and other respiratory pathogens in vitro and human breath samples. Med Mycol. 2008;46(3):209–15. doi:10.1080/13693780701753800.
Bazemore RA, Feng J, Cseke L, Podila GK. Biomedically important pathogenic fungi detection with volatile biomarkers. J Breath Res. 2012;6(1):016002. doi:10.1088/1752-7155/6/1/016002.
Beck JJ, Mahoney NE, Cook D, Gee WS. Generation of the volatile spiroketals conophthorin and chalcogran by fungal spores on polyunsaturated fatty acids common to almonds and pistachios. J Agric Food Chem. 2012;60(48):11869–76. doi:10.1021/jf304157q.
Stotzky G, Schenck S. Volatile organic compounds and microorganisms. CRC Crit Rev Microbiol. 1976;4(4):333–82.
Kaminski E, Stawicki S, Wasowicz E. Volatile flavor compounds produced by molds of Aspergillus, Penicillium, and Fungi imperfecti. Appl Microbiol. 1974;27(6):1001–4.
Meruva NK, Penn JM, Farthing DE. Rapid identification of microbial VOCs from tobacco molds using closed-loop stripping and gas chromatography/time-of-flight mass spectrometry. J Ind Microbiol Biotechnol. 2004;31(10):482–8.
Bitas V, McCartney N, Li N, Demers J, Kim JE, Kim HS, et al. Fusarium oxysporum volatiles enhance plant growth via affecting auxin transport and signaling. Front Microbiol. 2015;6:1248. doi:10.3389/fmicb.2015.01248.
Freire ES, Campos VP, Pinho RS, Oliveira DF, Faria MR, Pohlit AM. Volatile substances produced by Fusarium oxysporum from coffee rhizosphere and other microbes affect Meloidogyne incognita and Arthrobotrys conoides. J Nematol. 2012;44(4):321–8.
Park S, Lee K. Inverted race tube assay for circadian clock studies of the Neurospora accessions. Fungal Genet Rep. 2004;51(1):12–4.
Pastore GM, Park YK, Min DB. Production of fruity aroma by Neurospora from beiju. Mycol Res. 1994 Nov 1;98(11):1300–2.
Fiedler K, Schütz E, Geh S. Detection of microbial volatile organic compounds (MVOCs) produced by moulds on various materials. Int J Hyg Environ Health. 2001;204(2–3):111–21.
Gao P, Korley F, Martin J, Chen BT. Determination of unique microbial volatile organic compounds produced by five Aspergillus species commonly found in problem buildings. AIHA J (Fairfax, Va). 2002;63(2):135–40.
Keller NP, Turner G, Bennett JW. Fungal secondary metabolism—from biochemistry to genomics. Nat Rev Microbiol. 2005;3(12):937–47.
Kontoyiannis DP, Lewis RE, Lortholary O, Spellberg B, Petrikkos G, Roilides E, et al. Future directions in mucormycosis research. Clin Infect Dis. 2012;54(Suppl 1):S79–85. doi:10.1093/cid/cir886. Erratum in: Clin Infect Dis. 2012 Apr;54(8):1220
Koo S, Thomas HR, Daniels SD, Lynch RC, Fortier SM, Shea MM, et al. A breath fungal secondary metabolite signature to diagnose invasive aspergillosis. Clin Infect Dis. 2014;59(12):1733–40. doi:10.1093/cid/ciu725.
Moens M, Smet A, Naudts B, Verhoeven J, Ieven M, Jorens P, et al. Fast identification of ten clinically important micro-organisms using an electronic nose. Lett Appl Microbiol. 2006;42(2):121–6.
Schnabel RM, Boumans ML, Smolinska A, Stobberingh EE, Kaufmann R, Roekaerts PM, et al. Electronic nose analysis of exhaled breath to diagnose ventilator-associated pneumonia. Respir Med. 2015;109(11):1454–9. doi:10.1016/j.rmed.2015.09.014.
Chambers ST, Syhre M, Murdoch DR, McCartin F, Epton MJ. Detection of 2-pentylfuran in the breath of patients with Aspergillus fumigatus. Med Mycol. 2009;47(5):468–76. doi:10.1080/13693780802475212.
Wilson AD. Advances in electronic-nose technologies for the detection of volatile biomarker metabolites in the human breath. Meta. 2015;5(1):140–63. doi:10.3390/metabo5010140.
Gardner JW. Detection of vapours and odours from a multisensor array using pattern recognition part 1. Principal component and cluster analysis. Sensors Actuators B Chem. 1991;4(1–2):109–15.
Brattoli M, De Gennaro G, De Pinto V, Demarinis Loiotile A, Lovascio S, Penza M. Odour detection methods: olfactometry and chemical sensors. Sensors. 2011;11(5):5290–322.
Kalita P, Saikia M, Singh N. Electronic-nose technology and its application—a systematic survey. Internation J Innov Res Electr Electron Instrum Control Eng. 2015;3(1):123–8.
Spaněl P, Smith D. Progress in SIFT-MS: breath analysis and other applications. Mass Spectrom Rev. 2011;30(2):236–67. doi:10.1002/mas.20303.
Bean HD, Zhu J, Hill JE. Characterizing bacterial volatiles using secondary electrospray ionization mass spectrometry (SESI-MS). J Vis Exp. 2011;(52).pii: 2664. doi: 10.3791/2664.
Zhu J, Bean HD, Kuo YM, Hill JE. Fast detection of volatile organic compounds from bacterial cultures by secondary electrospray ionization-mass spectrometry. J Clin Microbiol. 2010;48(12):4426–31. doi:10.1128/JCM.00392-10.
Smith D, Španěl P. SIFT-MS and FA-MS methods for ambient gas phase analysis: developments and applications in the UK. Analyst. 2015;140(8):2573–91. doi:10.1039/c4an02049a.
Scotter JM, Langford VS, Wilson PF, McEwan MJ, Chambers ST. Real-time detection of common microbial volatile organic compounds from medically important fungi by selected ion flow tube-mass spectrometry (SIFT-MS). J Microbiol Methods. 2005;63(2):127–34. PubMed
Chippendale TW, Gilchrist FJ, Španěl P, Alcock A, Lenney W, Smith D. Quantification by SIFT-MS of volatile compounds emitted by Aspergillus fumigatus cultures and in co-culture with Pseudomonas aeruginosa, Staphylococcus aureus and Streptococcus pneumoniae. Anal Methods. 2014;6(20):8154–64.
Lough F, Perry JD, Stanforth SP, Dean JR. Detection of exogenous VOCs as a novel in vitro diagnostic technique for the detection of pathogenic bacteria. TrAC Trends Anal Chem. 2017;87:71–81.
Chambers ST, Bhandari S, Scott-Thomas A, Syhre M. Novel diagnostics: progress toward a breath test for invasive aspergillus fumigatus. Med Mycol. 2011;49(Suppl 1):S54–61. doi:10.3109/13693786.2010.508187.
Syhre M, Scotter JM, Chambers ST. Investigation into the production of 2-pentylfuran by Aspergillus fumigatus and other respiratory pathogens in vitro and human breath samples. Med Mycol. 2008;46(3):209–15. doi:10.1080/13693780701753800. PubMed
Sudfeld CR, Dasenbrook EC, Merz WG, Carroll KC, Boyle MP. Prevalence and risk factors for recovery of filamentous fungi in individuals with cystic fibrosis. J Cyst Fibros. 2010 Mar;9(2):110–6. doi:10.1016/j.jcf.2009.11.010.
Lin HC, Chooi YH, Dhingra S, Xu W, Calvo AM, Tang Y. The fumagillin biosynthetic gene cluster in aspergillus fumigatus encodes a cryptic terpene cyclase involved in the formation of β-trans-bergamotene. J Am Chem Soc. 2013;135(12):461.
Frisvad JC, Rank C, Nielsen KF, Larsen TO. Metabolomics of aspergillus fumigatus. Med Mycol. 2009;47(Suppl 1):S53–71. doi:10.1080/13693780802307720.
Nozoe S, Kobayashi H, Morisaki N. Isolation of β-trans-bergamotene from aspergillus fumigatus, a fumagillin producing fungi. Tetrahedron Lett. 1976;17(50):4625–6.
•• de Heer K, Kok MG, Fens N, Weersink EJ, Zwinderman AH, van der Schee MP, et al. Detection of airway colonization by Aspergillus fumigatus by use of electronic nose technology in patients with cystic fibrosis. J Clin Microbiol. 2016;54(3):569–75. doi:10.1128/JCM.02214-15. This is the first clinical study of the eNose in cystic fibrosis will provide a stimulus for further studies.
•• de Heer K, van der Schee MP, Zwinderman K, van den Berk IA, Visser CE, van Oers R, et al. Electronic nose technology for detection of invasive pulmonary aspergillosis in prolonged chemotherapy-induced neutropenia: a proof-of-principle study. J Clin Microbiol. 2013 May;51(5):1490–5. doi:10.1128/JCM.02838-12. This initial clinical study of the eNose in neutropenic sepsis provides a basis for further studies.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Advances in Diagnosis of Invasive Fungal Infections
Rights and permissions
About this article

Cite this article
Scott-Thomas, A., Chambers, S.T. Volatile Organic Compounds: Upcoming Role in Diagnosis of Invasive Mould Infections. Curr Fungal Infect Rep 11, 117–123 (2017). https://doi.org/10.1007/s12281-017-0284-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12281-017-0284-7