
Abstract
The objective of this chapter is to review and summarize the current economic estimates of influenza and the cost-effectiveness of its vaccines. We reviewed the published assessments of the economic costs of human seasonal and pandemic influenza internationally. Seasonal influenza costs Germany, France, and the USA between $4 and $87 billion annually. Depending upon the intensity of transmission and severity of disease, pandemic influenza may cause as many as 350 million deaths and result in economic losses topping $1 trillion – an impact great enough to create a worldwide recession. We then reviewed 100 papers primarily from more than a dozen countries which studied the cost-effectiveness of influenza vaccine in children, adults, and the elderly. These studies demonstrate that influenza vaccination is quite cost-effective among children 6 months to 18 years old, in health care workers and pregnant women, and in high-risk individuals. Remarkably, compared with the other recently introduced vaccines for children, such as rotavirus and pneumococcal polysaccharide, vaccinating children and school attendees results in societal cost savings because it obviates lost productivity and wages among infected individuals and their caretakers. Vaccination for children is recommended in the USA and in Canada, but public health policy makers in Europe have undervalued this vaccine and not recommended it so widely.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Annual seasonal outbreaks of influenza result in substantial socioeconomic costs. In addition to the health care costs incurred by sick patients needing outpatient care and hospitalization, the societal costs of lost productivity and ancillary costs are substantial. When children become ill, parents take time off from work to care for them and take them for treatment. Ill employees are absent from work, and even when present in the workplace, their productivity can be substantially reduced, while increasing the risk of transmission to coworkers. Retirees suffer some of the most severe complications of influenza and may require more assistance from family members and informal caregivers resulting in societal costs that exceed the usual medical expenditures.
Pandemic influenza that occurs only once every few decades results in much greater socioeconomic costs than annual seasonal influenza. During pandemics, more cases of influenza occur, but more importantly because of widespread fear of infection, people stop working, shopping, going to social and cultural events and venues where large numbers gather. The impact on the economy can be enormous depending upon the severity of the pandemic.
An efficacious influenza vaccine can avert most of the disease, deaths, and socioeconomic consequences, if vaccination programs effect high coverage among those at risk. Among some high-risk populations such as children and elderly, the societal savings from annual vaccination can sometimes outweigh the costs of the vaccination program. However, in other populations such as young adults, the costs of annual vaccination to prevent seasonal disease may substantially exceed any cost savings in health care and societal costs. When the societal cost savings are high, then vaccination becomes a high priority for public health.
This chapter will review three main topics in economics of influenza and vaccination:
-
1.
Macroeconomic estimates of the societal costs of pandemic influenza
-
2.
Estimates of the societal costs of the annual seasonal outbreaks
-
3.
Cost-effectiveness of annual vaccination for the prevention of seasonal outbreaks. The variation in cost-effectiveness values that result from comparisons among different target groups, methods, and locations will be reviewed
2 Methods
2.1 Societal Costs of Pandemic Influenza
Initial search at http://www.pandemicflu.gov provided four references on the economic implications of pandemic flu. Further sources were identified by performing a general internet search, as well as a query of the Web of Science and PubMed databases up to September 5, 2009, utilizing the terms: (flu OR influenza) AND pandemic AND (cost* OR macroeconomic* OR economic* OR death* OR mortality OR impact* OR effect*) AND (worldwide OR global OR “united states”).
2.2 Societal Costs of Seasonal Influenza
Sources were identified by performing a general internet search, as well as a query of the Web of Science and PubMed databases up to September 5, 2009, utilizing the terms: (flu OR influenza) AND seasonal AND (cost* OR macroeconomic* OR economic* OR death* OR mortality OR impact* OR effect*) AND (worldwide OR global OR “united states”).
2.3 Cost-Effectiveness: Children
We searched Web of Science and PubMed databases up to September 5, 2009, using the following Boolean search: (flu OR influenza) AND (cost* OR economic* OR pharmacoeconomic*) AND (child* OR infant* OR toddler*). The bibliographies of retrieved studies were reviewed to identify studies that may have been missed by these search criteria. This approach produced 417 potentially relevant articles.
These abstracts were assessed and only studies published within the last 15 years that contained an original, quantitative economic comparison of vaccination of children against seasonal influenza (compared with no intervention) were included. This produced a list of nine references that were then analyzed in detail. Of these, the study published by [1] was excluded for failing to include the indirect costs of influenza. Additionally, the paper published by [2] the same year was left out because the cohort study was based on a small number (N = 303) of vaccinated and nonvaccinated individuals with wide variation in average costs (e.g., $131.43 ± 1058).
To compare results of the papers, metrics were converted to the prevailing measure in the literature, which was dollars saved per child vaccinated. Schmier et al. [3] presented their results in dollars saved per family with school-age children, which was converted by assuming an average of 1.4 school-age children in families with children between 5 and 18 years. All foreign currencies were converted to US dollars according to the exchange rate during the year of the study (http://www.oanda.com/convert/fxhistory), and all dollar values were adjusted to 2009 dollars using general (as opposed to health care) inflation rates, given that the majority of the costs of influenza were found to be nonmedical.
2.4 Cost-Effectiveness: Elderly
We searched Web of Science and PubMed databases up to September 5, 2009, using the following Boolean search: (flu OR influenza) AND (cost* OR economic* OR pharmacoeconomic*) AND elderly. The bibliographies of retrieved studies were reviewed to identify studies that may have been missed by these search criteria. This approach produced 436 potentially relevant articles, which were filtered using criteria similar to those applied to the articles on influenza in children. This produced a list of 12 references which were then analyzed in greater detail. Of these, the studies published by [4, 5], were excluded as their analyses were based on a small number of people with no significant difference in incidence of influenza-like illness (ILI) and hospitalizations between those vaccinated and those not vaccinated.
For those studies reporting costs per year of life saved, foreign currencies were converted to dollars using exchange rates from the year of the study and then adjusted to 2009 dollars using general inflation rates as described above. For those reporting benefit-to-cost ratios, no such conversions were necessary.
3 Results
3.1 Macroeconomic Costs of Seasonal Influenza
The seasonal influenza epidemics that occur throughout the world each year wreak billions of dollars in economic damage, in addition to killing hundreds of thousands. Figure 1 illustrates the estimated societal costs (in 2009 dollars) for the USA (approximately $240/capita), France ($80/capita), Germany ($50/capita), Thailand ($0.50–$1/capita), and Australia [$5/capita (health care costs only)], the only countries for which such an analysis has been undertaken. Even in Thailand, a middle-income country, average costs to society total $40 million annually [6], while the toll is significantly greater in higher income countries ($4–$88 billion) [8, 9]. The differences in these per capita estimates stem from differences in health care costs in value of a day of lost productivity and absenteeism for the sick person and his/her caretaker during illness.

National estimates of direct and indirect costs of seasonal influenza (2009 US dollars)
The majority of these costs are not from increased health care expenditures (hospitalizations, ambulatory care visits, drugs, and over-the-counter treatments, etc.) but rather from lost productivity due to illness in jobholders or their dependents. Indeed, these “indirect” costs of illness to be two to seven times greater than the “direct” costs (Fig. 1). Furthermore, because these calculations do not include reduced productivity of employees who come to work despite illness, they are an underestimate.
3.2 Macroeconomic Costs of Pandemic Influenza
Figure 2 presents the predicted economic costs of a pandemic (adjusted to 2009 dollars) in the USA performed by several different international agencies. Even a mild pandemic would cost the USA nearly $100 billion and take as many as two million lives (Fig. 3). Worldwide, a pandemic could result in as many as 350 million lives (Fig. 4), with economic costs predicted to range from several hundred billion (1,000 million) dollars for mild disease to several trillion (million million) dollars for a more severe scenario (Fig. 5). Under the last estimate, the slowdown caused by the disease would be expected to precipitate a worldwide recession [10–14].

Predicted economic cost of pandemic flu to the USA under different scenarios (2009 US dollars)

Deaths from pandemic flu in the USA

Predicted worldwide deaths from pandemic flu

Predicted worldwide economic cost of pandemic flu (2009 US dollars)
Surprisingly, Fig. 6 demonstrates that 60% of the costs of a pandemic are predicted to result not from infection, but from people’s effort to avoid infection [12]. These estimates are based on observations of the SARS epidemic in Hong Kong and Canada, where many remained in their homes, avoiding places of work, markets, restaurants, and so on, until the fear of infection subsided.

Distribution of estimated societal costs during a pandemic
3.3 Cost-Effectiveness of Vaccination
Given the high societal costs of seasonal influenza and the catastrophic potential of pandemic flu, strategies for mitigating the flow of this disease through populations are of crucial human and economic importance. Although there are several strategies to address the spread of influenza, the low cost and relatively good efficacy (25–85%) of vaccination mean that it is still preferred over other measures such as targeted antiretroviral therapy and, in more extreme cases, quarantine of those who are ill and their susceptible associates through closure of schools and workplaces [15]. This review focuses on vaccination against influenza in the main target groups: children, elderly, and adults.
The studies were conducted in the USA and more than a dozen other countries, and most take the societal perspective for costs and include indirect costs of lost productivity from absenteeism and time off from work.
The societal cost of a vaccination program ideally be calculated as a net cost using the following simplified formula:
-
Net Cost of Vaccination Program =
-
Cost of the Vaccination Program + Cost of Side Effects from the Vaccine
-
− Cost of Healthcare Averted Resulting from Illnesses Prevented
-
− Cost of Lost Productivity Averted Resulting from Illnesses Prevented
When estimating cost-effectiveness, the net cost of the program is compared with the illness and disability prevented usually in terms of years of life saved (YOLS), quality adjusted life years (QALYs), or disability adjusted life years (DALYs). When the net costs are less than zero, as is the case in most of the studies of children vaccination, then the program saves society money.
Influenza vaccine has extremely few, rare, and usually mild side effects when they occur so that many of the studies do not include any estimates of costs of side effects. Unfortunately, many of the published cost-effectiveness assessments use different methods to estimate costs of health care and lost productivity so that the results are difficult to compare.
3.3.1 Children
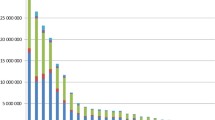
Figure 7 reports estimates from nine studies for the cost-effectiveness of annual influenza vaccination in children to prevent seasonal influenza. Nearly all of the analyses demonstrate cost savings to society from vaccination. When health care costs are considered alone, there are no net savings (i.e., the cost of vaccination exceeds the cost of averted health care expenditures in most cases) [2,16–23]. Net savings result only when societal costs of lost productivity are included. Important parameters that affect the results from each of these papers are outlined in Table 1. The inconsistencies in the assumptions and methods are substantial and explain the wide range in results.

Economic benefits of influenza immunization in children (cost savings)
Nonetheless, cost savings from childhood vaccination remains robust across a wide range of model input values and assumptions. These include vaccine effectiveness estimates from 25% to 85% (higher efficacy improves cost-effectiveness), attack rates from 13% to 40% (higher attack rates improve cost-effectiveness), and vaccine coverage from 20% to 100% (variable results on cost-effectiveness), and vaccination program costs of $0–$60 (higher vaccine costs decrease cost-effectiveness). The target age group for vaccination varied from day care center attendees, school children, and all children 6 months to 18 years. Some of the studies included only illness in those children in the target age group receiving the vaccine; others included secondary cases in families and general population averted resulting from childhood vaccination. In all studies, indirect benefits such as fewer days off from work for parents to care for sick children greatly exceeded the direct savings from the obviated medical expenses.
3.3.2 Elderly
Summarized in Fig. 8 are the findings from ten studies of the cost-effectiveness of vaccinating the elderly against seasonal influenza, measured in dollars per year of life saved. Only one study (Scuffham and West, England and Wales) demonstrated cost savings [22]. Others showed that vaccination of the elderly costs $700 to $15,500 per year of life saved (YOLS) [24–31]. Most of the studies only include the direct health care costs as lost economic productivity is assumed to be minimal among the elderly.

Cost-effectiveness of influenza immunization in the elderly in terms of years of life saved (YOLS)
A selection of important assumptions included in each of these investigations is presented in Table 2. These models apply varying assumptions, including vaccine efficacies from 18% to 60%, attack rates from 1% to 15%, and vaccination coverages from 37% to 100%. Despite these variations, all studies found the cost/YOLS to be less than $50,000. Interventions less than this threshold are usually considered cost-effective and of societal value for resource allocation.
3.3.3 Working Adults
A number of articles have assessed cost–benefit and cost-effectiveness of influenza vaccination in healthy adults [35–40]. Similar to the analyses of influenza vaccination in children and in the elderly, the studies have involved a variety of population groups (adults 50–64, 18–50, 25–64 years; health care workers, pregnant women, etc.). Similarly, the studies applied a variety of methods, including simulation models, observational models, and randomized double-blind placebo-controlled trials with varied assumptions for some of the key factors.
Despite these differences, the majority of the studies demonstrate that vaccination of high-risk individuals, health care workers, and pregnant women is likely to be cost-effective.
4 Discussion
4.1 Cost-Effectiveness and Cost–Benefit Analysis: Methodological Issues
Although the data, when viewed as a whole, clearly demonstrate influenza vaccination to be quite cost-effective, there were several methodological inconsistencies noted during our review.
First, several studies estimating cost-effectiveness for country #1 applied disease incidence rates from country #2 but cost data from country #1. It is probable that this was done because incidence rates were not available for country #1. However, the authors may draw conclusions based on data that were not necessarily representative of the country for which they were doing the analysis. Several studies did not include one-way, two-way, or multi-way sensitivity analyses to test the robustness of the results to the lack of confidence in the assumptions.
Second, there were several studies that directly compared health outcomes for people who chose to be immunized with those who chose not to be immunized. It is common knowledge among epidemiological researchers that the groups of individuals who seek medical care are different in many ways from the groups of individuals who do not. Although not every study can be a randomized controlled trial, for those that are not, care should be taken to eliminate confounding by controlling for the differences between intervention and control groups that are unrelated to vaccination. In many of these studies, no such precautions were taken.
Finally, a few studies made an attempt to include the effects of herd immunity. In order to do this, authors must model the spread of infection through the population or make assumptions about transmission rates from infected to susceptibles. Influenza is one of the most transmissible human infections. When herd immunity is included, the estimates of benefits of vaccination rise.
This review includes results from studies using live-attenuated intranasal vaccine and the inactivated injectable vaccine. The estimated vaccine efficacy and community effectiveness of these vaccines overlapped and cost-effectiveness/benefit results were similar; therefore we reviewed them together.
4.2 Policy Implications
Despite these methodological problems, the consistency of findings across a wide range of methods and study populations demonstrates that among most population groups influenza vaccination is highly cost-effective.
Table 3 lists estimates for the cost-effectiveness of several other recently introduced vaccines that are widely recommended for children and preteens. Influenza vaccination in these age groups is generally cost saving compared with the societal costs of several thousand dollars for saving only one quality adjusted life year (QALY) for human papilloma virus (HPV) vaccine and more than one hundred thousand for only one year of life saved (YOLS) for pneumococcal vaccine. The US Advisory Committee on Immunization Practices recommends that all children (or preteens in the case of HPV) receive the vaccines listed in Table 3 plus an annual influenza vaccination. Canada recommends vaccination of the entire population annually. A few European countries recommend annual vaccination of children, despite the benefits demonstrated in this review, and only recommend vaccination for the elderly and those with chronic illness. Public health policymakers and health providers have undervalued influenza vaccination despite clear benefits.
References
Prosser LA, Bridges CB, Uyeki TM, Hinrichsen VL, Meltzer MI, Molinari NA, Schwartz B, Thompson WW, Fukuda K, Lieu TA (2006) Health benefits, risks, and cost-effectiveness of influenza vaccination of children. Emerg Infect Dis 12(10):1548–1558
Schmier J, Li S, King JC Jr, Nichol K, Mahadevia PJ (2008) Benefits and costs of immunizing children against influenza at school: an economic analysis based on a large-cluster controlled clinical trial. Health Aff (Millwood) 27(2):w96–104
Esposito S, Marchisio P, Bosis S, Lambertini L, Claut L, Faelli N, Bianchi C, Colombo GL, Principi N (2006) Clinical and economic impact of influenza vaccination on healthy children aged 2-5 years. Vaccine 24(5):629–635
Allsup S, Gosney M, Haycox A, Regan M (2003) Cost-benefit evaluation of routine influenza immunisation in people 65–74 years of age. Health Technol Assess 7(24):iii-x, 1–65. PMID: 14499051
Allsup S, Haycox A, Regan M, Gosney M (2004) Is influenza vaccination cost effective for healthy people between ages 65 and 74 years? A randomised controlled trial. Vaccine 16;23(5):639–645
Simmerman JM, Lertiendumrong J, Dowell SF, Uyeki T, Olsen SJ, Chittaganpitch M et al (2006) The cost of influenza in Thailand. Vaccine 24(20):4417–4426
Newall AT, Scuffham PA (2008) Influenza-related disease: the cost to the Australian healthcare system. Vaccine. Dec 9;26(52):6818–6823
Molinari N, Ortega-Sanchez I, Massonnier M, Thompson W, Wortley P, Weintraub E et al (2007) The annual impact of seasonal influenza in the US: measuring disease burden and costs. Vaccine 25:5086–5096
Szucs T (1999) The socio-economic burden of influenza. J Antimicrob Chemother 44:11–15
Congressional Budget Office (2006) A potential influenza pandemic: an update on possible macroeconomic effects and policy issues. Congressional Budget Office, Washington
Meltzer M, Cox N, Fukuda K (1999) The economic impacts of pandemic influenza in the united states: priorities for intervention. Emerg Infect Dis 5(5):659–671
Burns A, van der Mensbrugghe D, Timmer H (2008) Evaluating the economic consequences of avian influenza. The World Bank, Washington
McKibbin W, Sidorenko A (2006) Global macroeconomic consequences of pandemic influenza. Lowy Institute for International Policy, Sydney
Bloom E, deWit V, Carangal-San Jose MJ (2005) Potential Economic Impact of an Avian Flu Pandemic on Asia. Washington, DC: Asian Development Bank. Economics and Research Department. ERD Policy Brief Series #42
Sander B, Nizam A, Garrison LP (2009) Economic evaluation of influenza pandemic mitigation strategies in the united states using a stochastic microsimulation transmission model. Value Health 12(2):226–233
Weycker D, Edelsberg J, Halloran ME, Longini IMJ, Nizam A, Ciuryla V et al (2005) Population-wide benefits of routine vaccination of children against influenza. Vaccine 23(10):1284–1293
Meltzer MI, Neuzil KM, Griffin MR, Fukuda K (2005) An economic analysis of annual influenza vaccination of children. Vaccine 23(8):1004–1014
Hibbert CL, Piedra PA, McLaurin KK, Vesikari T, Mauskopf J, Mahadevia PJ (2007) Cost-effectiveness of live-attenuated influenza vaccine, trivalent in preventing influenza in young children attending day-care centres. Vaccine 25(47):8010–8020
Marchetti M, Kuhnel UM, Colombo GL, Esposito S, Principi N (2007) Cost-effectiveness of adjuvanted influenza vaccination of healthy children 6 to 60 months of age. Hum Vaccin 3(1):14–22
Dayan GH, Nguyen VH, Debbag R, Gomez R, Wood SC (2001) Cost-effectiveness of influenza vaccination in high-risk children in argentina. Vaccine 19(30):4204–4213
Navas E, Salleras L, Dominguez A, Ibanez D, Prat A, Sentis J et al (2007) Cost-effectiveness analysis of inactivated virosomal subunit influenza vaccination in children aged 3–14 years from the provider and societal perspectives. Vaccine 25(16):3233–3239
Salleras L, Navas E, Dominguez A, Ibanez D, Prat A, Garrido P et al (2009) Economic benefits for the family of inactivated subunit virosomal influenza vaccination of healthy children aged 3–14 years during the annual health examination in private paediatric offices. Vaccine 27(25–26):3454–3458
Skowronski DM, Woolcott JC, Tweed SA, Brunham RC, Marra F (2006) Potential cost-effectiveness of annual influenza immunization for infants and toddlers: experience from Canada. Vaccine 24(19):4222–4232
Cai L, Uchiyama H, Yanagisawa S, Kamae I (2006) Cost-effectiveness analysis of influenza and pneumococcal vaccinations among elderly people in Japan. Kobe J Med Sci 52(3–4):97–109
Hoshi SL, Kondo M, Honda Y, Okubo I (2007) Cost-effectiveness analysis of influenza vaccination for people aged 65 and over in Japan. Vaccine 25(35):6511–6521
Wang ST, Lee LT, Chen LS, Chen TH (2005) Economic evaluation of vaccination against influenza in the elderly: an experience from a population- based influenza vaccination program in Taiwan. Vaccine 23(16):1973–1980
Scuffham PA, West PA (2002) Economic evaluation of strategies for the control and management of influenza in Europe. Vaccine 20(19–20):2562–2578
Postma MJ, Bos JM, van Gennep M, Jager JC, Baltussen R, Sprenger MJ (1999) Economic evaluation of influenza vaccination. Assessment for the Netherlands. Pharmacoeconomics 16(Suppl 1):33–40
Gutierrez JP, Bertozzi SM (2005) Influenza vaccination in the elderly population in Mexico: economic considerations. Salud Pública Méx 47(3):234–239
Nichol KL, Goodman M (1999) The health and economic benefits of influenza vaccination for healthy and at-risk persons aged 65 to 74 years. Pharmacoeconomics 16(Suppl 1):63–71
Maciosek MV, Solberg LI, Coffield AB, Edwards NM, Goodman MJ (2006) Influenza vaccination health impact and cost effectiveness among adults aged 50 to 64 and 65 and older. Am J Prev Med 31(1):72–79
Ohkusa Y (2005) Policy evaluation for the subsidy for influenza vaccination in elderly. Vaccine 23(17–18):2256–2260
Gasparini R, Lucioni C, Lai P, Maggioni P, Sticchi L, Durando P et al (2002) Cost–benefit evaluation of influenza vaccination in the elderly in the Italian region of Liguria. Vaccine 20(Suppl 5):B50–B54
Fitzner KA, Shortridge KF, McGhee SM, Hedley AJ (2001) Cost-effectiveness study on influenza prevention in Hong Kong. Health Policy 56(3):215–234
Lee PY, Matchar DB, Clements DA, Huber J, Hamilton JD, Peterson ED (2002) Economic analysis of influenza vaccination and antiviral treatment for healthy working adults. Ann Intern Med 137(4):225–231
Burls A, Jordan R, Barton P, Olowokure B, Wake B, Albon E et al (2006) Vaccinating healthcare workers against influenza to protect the vulnerable – is it a good use of healthcare resources? A systematic review of the evidence and an economic evaluation. Vaccine 24(19):4212–4221
Bridges CB, Thompson WW, Meltzer MI, Reeve GR, Talamonti WJ, Cox NJ et al (2000) Effectiveness and cost-benefit of influenza vaccination of healthy working adults: a randomized controlled trial. JAMA 284(13):1655–1663
Turner D, Wailoo A, Nicholson K, Cooper N, Sutton A, Abrams K (2003) Systematic review and economic decision modeling for the prevention and treatment of influenza A and B. Health Technol Assess 7(35):iii–iv, xi–xiii, 1–170
Postma MJ, Jansema P, van Genugten ML, Heijnen ML, Jager JC, de Jong-van den Berg LT (2002) Pharmacoeconomics of influenza vaccination for healthy working adults: reviewing the available evidence. Drugs 62(7):1013–1024
Rothberg MB, Rose DN (2005) Vaccination versus treatment of influenza in working adults: a cost-effectiveness analysis. Am J Med 118(1):68–77
Lieu TA, Ray GT, Black SB, Butler JC, Klein JO, Breiman RF, Miller MA, Shinefield HR (2000) Projected cost-effectiveness of pneumococcal conjugate vaccination of healthy infants and young children. JAMA 283(11):1460–1468
Shepard CW, Ortega-Sanchez IR, Scott RD 2nd, Rosenstein NE (2005) Cost-effectiveness of conjugate meningococcal vaccination strategies in the United States. Pediatrics 115(5):1220–1232
Widdowson MA, Meltzer MI, Zhang X, Bresee JS, Parashar UD, Glass RI (2007) Cost-effectiveness and potential impact of rotavirus vaccination in the United States. Pediatrics 119(4):684–697
Kim JJ, Goldie SJ (2008) Health and economic implications of HPV vaccination in the United States. N Engl J Med 359(8):821–832
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Birkhäuser Basel
About this chapter
Cite this chapter
Walsh, J.A., Maher, C. (2011). Economic Implications of Influenza and Influenza Vaccine. In: Rappuoli, R., Del Giudice, G. (eds) Influenza Vaccines for the Future. Birkhäuser Advances in Infectious Diseases. Springer, Basel. https://doi.org/10.1007/978-3-0346-0279-2_19
Download citation
DOI: https://doi.org/10.1007/978-3-0346-0279-2_19
Published:
Publisher Name: Springer, Basel
Print ISBN: 978-3-0346-0278-5
Online ISBN: 978-3-0346-0279-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)