
Abstract
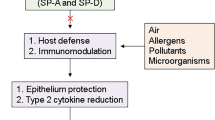
Pulmonary surfactant is a complex mixture of lipids and proteins, and is synthesized and secreted by alveolar type II epithelial cells and bronchiolar Clara cells. It acts to keep alveoli from collapsing during the expiratory phase of the respiratory cycle. After its secretion, lung surfactant forms a lattice structure on the alveolar surface, known as tubular myelin. Surfactant proteins (SP)-A, B, C and D make up to 10% of the total surfactant. SP-B and SPC are relatively small hydrophobic proteins, and are involved in the reduction of surface-tension at the air-liquid interface. SP-A and SP-D, on the other hand, are large oligomeric, hydrophilic proteins that belong to the collagenous Ca2+-dependent C-type lectin family (known as “Collectins”), and play an important role in host defense and in the recycling and transport of lung surfactant (Awasthi 2010) (Fig. 43.1). In particular, there is increasing evidence that surfactant-associated proteins A and -D (SP-A and SP-D, respectively) contribute to the host defense against inhaled microorganisms (see Chaps. 24 and 25). Based on their ability to recognize pathogens and to regulate the host defense, SP-A and SP-D have been recently categorized as “Secretory Pathogen Recognition Receptors”. While SP-A and SP-D were first identified in the lung; the expression of these proteins has also been observed at other mucosal surfaces, such as lacrimal glands, gastrointestinal mucosa, genitourinary epithelium and periodontal surfaces. SP-A is the most prominent among four proteins in the pulmonary surfactant-system. The expression of SP-A is complexly regulated on the transcriptional and the chromosomal level. SP-A is a major player in the pulmonary cytokine-network and moreover has been described to act in the pulmonary host defense. This chapter gives an overview on the understanding of role of SP-A and SP-D in for human pulmonary disorders and points out the importance for pathology-orientated research to further elucidate the role of these molecules in adult lung diseases. As an outlook, it will become an issue of pulmonary pathology which might provide promising perspectives for applications in research, diagnosis and therapy (Awasthi 2010).
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Chronic Obstructive Pulmonary Disease
- Respiratory Distress Syndrome
- Idiopathic Pulmonary Fibrosis
- Acute Respiratory Distress Syndrome
- Congenital Diaphragmatic Hernia
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Pulmonary Surfactant
Pulmonary surfactant is a complex mixture of lipids and proteins, and is synthesized and secreted by alveolar type II epithelial cells and bronchiolar Clara cells. It acts to keep alveoli from collapsing during the expiratory phase of the respiratory cycle. After its secretion, lung surfactant forms a lattice structure on the alveolar surface, known as tubular myelin. Surfactant proteins (SP)-A, B, C and D make up to 10% of the total surfactant. SP-B and SPC are relatively small hydrophobic proteins, and are involved in the reduction of surface-tension at the air-liquid interface. SP-A and SP-D, on the other hand, are large oligomeric, hydrophilic proteins that belong to the collagenous Ca2+-dependent C-type lectin family (known as “Collectins”), and play an important role in host defense and in the recycling and transport of lung surfactant (Awasthi 2010) (Fig. 43.1). In particular, there is increasing evidence that surfactant-associated proteins A and -D (SP-A and SP-D, respectively) contribute to the host defense against inhaled microorganisms (see Chaps. 24 and 25). Based on their ability to recognize pathogens and to regulate the host defense, SP-A and SP-D have been recently categorized as “Secretory Pathogen Recognition Receptors”. While SP-A and SP-D were first identified in the lung, the expression of these proteins has also been observed at other mucosal surfaces, such as lacrimal glands, gastrointestinal mucosa, genitourinary epithelium and periodontal surfaces. SP-A is the most prominent among four proteins in the pulmonary surfactant-system. The expression of both SP-A and SP-D is complexly regulated on the transcriptional and the chromosomal level. SP-A is a major player in the pulmonary cytokine-network and has been described to act in the pulmonary host defense. This chapter gives an overview on the understanding of role of SP-A and SP-D in for human pulmonary disorders and points out the importance for pathology-orientated research to further elucidate the role of these molecules in adult lung diseases. As an outlook, it will become an issue of pulmonary pathology which might provide promising perspectives for applications in research, diagnosis and therapy (Awasthi 2010).

Presence of surfactant proteins (SP) in lung surfactant, their properties and major functions of SP-A and SP-D
2 SP-A and SP-D in Interstitial Lung Disease
SP-A and SP-D appear in the circulation in specific lung diseases. Interstitial lung disease (ILD), also known as diffuse parenchymal lung disease (DPLD), refers to a group of lung diseases affecting the interstitium of lung: alveolar epithelium, pulmonary capillary endothelium, basement membrane, perivascular and perilymphatic tissues. The term ILD is used to distinguish these diseases from obstructive airways diseases. Most types of ILD involve fibrosis, but this is not essential; indeed fibrosis is often a later feature. The phrase “pulmonary fibrosis” is no longer considered a synonym, but the term is still used to denote ILD involving fibrosis. The term is commonly combined with idiopathic in “idiopathic pulmonary fibrosis”, denoting fibrotic ILD that cannot be ascribed to a distinct primary cause.
2.1 Pneumonitis
Chronic hypersensitivity pneumonitis (HP) eventually ensues to extensive lung fibrosis when exposure to causative antigen continues. Klebs von den Lungen (KL)-6, a mucin-like glycoprotein and SP-D are elevated in most cases. Correct diagnosis in the early stage is crucial, since chronic summer-type HP can result in a fatal outcome after continuous exposure to the causative antigen (Inase et al. 2007). In pulmonary tissues of collagen vascular disease-associated interstitial pneumonia (CVD-IP) and hypersensitivity pneumonitis (HP), SP-D can be a marker for maturity of regenerating epithelial cells. SP-A along with KL-6 is detected in intimate relationship to the stage of regeneration of alveolar epithelial cells and expressed before SP-D (Ohtsuki et al. 2007). Radiation pneumonitis (RP) is most common complication of radiotherapy for thoracic tumors. Both SP-A and SP-D concentrations in sera from patients with RP were significantly higher than those from patients without RP. Serum SP-A and SP-D may be of diagnostic value for detection of RP, even when radiographic change is faint (Takahashi et al. 2001). Despite the rise of SP-D and KL-6 in serum in adult patients with various types of interstitial pneumonia (IP) and collagen diseases with interstitial pneumonia, KL-6 may be superior in sensitivity of IP, where as SP-D may be more specific for IP than KL-6. Early decrease of SP-D contrasts with the transient increase of KL-6 levels after prednisolone pulse therapy (Arai et al. 2001). High serum KL-6 value is an indicator of ILD of Wilson-Mikity syndrome and better than SP-D and LDH levels (Takami et al. 2003). Thus serum SP-A and SP-D monitoring along with KL-6 is useful indicator for estimating RP (Matsuno et al. 2006).
2.2 Interstitial Pneumonia (IP)
2.2.1 SP-A and SP-D in BAL as Indicator of Pneumonia in Children
SP-A and SP-D in serum significantly increase in patients with pulmonary alveolar proteinosis (PAP), idiopathic pulmonary fibrosis (IPF) and interstitial pneumonia with collagen vascular diseases (IPCD) (Kuroki et al. 1998; Takahashi et al. 2006b). The concentrations of SP-A and SP-D in BAL fluids from patients with IPF and IPCD are rather lower than those in healthy controls; and the SP-A/phospholipid ratio may be a useful marker of survival prediction. SP-D-deficient patients have more frequently pneumonias and their long-term outcome is worse than those with detectable SP-D. Among children with recurrent bronchitis and SP-D detectable in bronchoalveolar lavage (BAL), patients with allergic asthma had threefold levels of SP-D compared with controls. In contrast, SP-D deficiency due to consumption or failure to up-regulate SP-D may be linked to pulmonary morbidity in children (Griese et al. 2008).
2.2.2 SP-A Levels can Differentiate Usual Interstitial Pneumonia with Non-Specific Interstitial Pneumonia (NSIP)
There is a need to use serum markers for differentiating usual interstitial pneumonia (UIP) from other ILD. Serum levels of SP-A and SP-D in patients with UIP and nonspecific interstitial pneumonia (NSIP) are significantly higher than in healthy volunteers. In particular, serum SP-A levels in patients with UIP are significantly higher than in patients with NSIP, where as SP-D in BAL fluid in UIP patients were significantly lower than in patients with NSIP. Thus, serum SP-A level seems useful marker to differentiate UIP from NSIP (Ishii et al. 2003).
Abnormal tracheal aspirate surfactant phospholipids and SP-A are noted in children with bacterial pneumonia, viral pneumonitis, and ARDS, but not in children on cardiopulmonary bypass (Baughman et al. 1993; LeVine et al. 1996). SP-A in pneumonia group is significantly reduced and the reduction was better indicator in the Gm+-pneumonia group than in Gm−-pneumonia group patients (Baughman et al. 1993). Fulminant early-onset neonatal pneumonia is associated with ascending intrauterine infection (IUI) and alveolar Mф showed significantly less nitric oxide synthase 2 (NOS2) isoform than in the controls. In the airway samples, the infants with fulminant pneumonia after birth had low intracellular NOS2 and significantly low IL-1β and SP-A than noninfected IUI infants (Aikio et al. 2000).
Foster et al. (2002) suggested that signaling of EGF axis and differential regulation of SPs persist during postnatal lung development, and SP-A and SP-D may modulate post-pneumonectomy (PNX) lung growth in dogs. SP-D in patients, hospitalized for community-acquired pneumonia of suspected bacterial origin, indicates significant changes during pulmonary infection (Daimon et al. 2005; Leth-Larsen et al. 2003). The SA-A and SP-D in sera are useful for identification of the clinical condition of horses with bacterial pneumonia (Hobo et al. 2007).
2.3 ILD Due to Inhaled Substances
Cigarette smoke may alter component and function of pulmonary surfactant. Alterations in serum levels of SP-A may reflect smoking habits since serum SP-A was higher in active smokers than in nonsmokers (Nomori et al. 1998). However, SP-A is not a sensitive discriminating factor to separate smokers from nonsmokers. The contents of SP-A and SP-D in BAL fluids were significantly decreased in smokers compared to those in nonsmokers, although there was no significant difference of total phospholipid content between two groups (Honda et al. 1996). SP-A may decrease due to the cumulative effects of long-term smoking and development of emphysema, while SP-D decreases due to long-term smoking (Betsuyaku et al. 2004; Shijubo et al. 1998). Emphysema can be induced in mice by chronic cigarette smoke exposure with increase of SP-D in emphysema lungs. While accumulation of foamy alveolar macrophages may play a key role in the development of smoking-induced emphysema, increased SP-D may play a protective role in the development of smoking-induced emphysema, in part by preventing alveolar cell death (Hirama et al. 2007).
Although effects of maternal smoking on fetal growth and viability are overwhelmingly negative, there is a paradoxical enhancement of lung maturation as evidenced, in part, by a lower incidence of RDS in infants of smoking mothers. Epidemiologic and experimental evidence further support the view that a tobacco smoke constituent, possibly nicotine, affects the development of the lung in utero. The murine embryonic lungs explanted at 11 days gestation showed a 32% increase in branching after 4 days in culture in presence of 1 μM nicotine and 7–15-fold increases in mRNAs encoding SP-A and SP-C after 11 days. The nicotine-induced stimulation of surfactant gene expression could, in part, account for the effect of maternal smoking on the incidence of RDS (Wuenschell et al. 1998).
Intratracheal administration of crystalline silica to rats elicits a marked increase in alveolar accumulation of surfactant lipids and SP-A. The extracellular accumulation of SP-D is markedly increased in silica-induced lipoproteinosis, and that SP-D is associated with amorphous components identified by electron microscopy. SP-D may be useful biomarkers for early diagnosis and serum SP-D concentration may associate with the pathogenesis of silicosis (Barbaro et al. 2002; Wang et al. 2007b). Alcohol consumption at high levels during pregnancy is associated with immuno-modulation and premature birth. Chronic maternal ethanol consumption during the third trimester of pregnancy alters SP-A gene expression in fetal lung. These alterations may underlie increased susceptibility of preterm infants, exposed to ethanol in utero, to RSV and other microbial agents (Lazic et al. 2007). The exposure to moderate and high occupational levels of Diesel exhaust (DE) causes an increase in lung injury and inflammation, and a decrease in host defense molecules, which could result in increased severity of infectious and allergic lung disease. Several inflammatory and immune cytokines are upregulated at various time points and concentrations, in contrast to SP-A and SP-D which were significantly decreased at protein level. (Gowdy et al. 2008).
2.4 Idiopathic Pulmonary Fibrosis
Idiopathic pulmonary fibrosis (IPF) is a progressive disease of lung characterized by an inflammatory infiltrate, alveolar type II cell hypertrophy and hyperplasia, and ultimate parenchymal scarring. The phospholipid composition of the surface-active material recovered by BAL is abnormal in this disease. The content of SP-A in lavage was reduced, even when normalized for the total amount of surface-active material (SP-A/total phospholipids (PL)) recovered. The reduction in SP-A was not specific to IPF but also occurred in other interstitial lung diseases. Despite this, SP-A/PL in BAL is a biochemical marker that predicts survival in patients with IPF (McCormack et al. 1995; Phelps et al. 2004).
The serum SP-A and SP-D levels are significantly elevated in patients with IPF and systemic sclerosis compared to sarcoidosis, beryllium disease and normal controls, and correlated with radiographic abnormalities in patients with IPF. Dohmoto et al. (2000) hypothesized that regenerated or premature bronchoepithelial cells may circulate in the blood in patients with IPF. RT-PCR for cytokeratin 19 (CK19) and pulmonary SP-A in peripheral blood in patients with IPF and pulmonary fibrosis (PF) associated with collagen vascular disorders suggests that there were some circulating bronchoepithelial cells expressing mRNA for SP-A in peripheral blood of patients associated with collagen vascular disorders. Thus, both serum SP-A and SP-D levels are highly predictive of survival in patients with IPF (Greene et al. 2002; Takahashi et al. 2006b) and the measurement of SP-D in sera can provide an easily identifiable and useful clinical marker for the diagnosis of IPF, IPCD, and PAP, and can predict the disease activity of IPF and IPCD and the disease severity of PAP (Honda et al. 1995). However, KL-6 is the best serum marker for ILD (Ohnishi et al. 2002). Serum KL-6 and SP-D were also prognostic markers in acute exacerbation of IPF after treatment with Sivelestat (Endo et al. 2006; Nakamura et al. 2007). High levels of SP-D in BAL fluids are associated in patients with PAP, but not with IPF and IPCD.
Selman et al. (2003) examined associations between IPF and genetic polymorphic variants of SP-A1, SP-A2, SP-B, SP-C, and SP-D. One SP-A1 (6A4) allele and SNPs that characterize the 6A4 allele and one SP-B (B1580_C) were found with higher in nonsmoker and smoker IPF subgroups, respectively, compared with healthy controls. To explore whether a tryptophan (in 6A4) or an arginine (in other SP-A1 alleles and in all SP-A2 alleles) at amino acid 219 alters protein behavior, two truncated proteins that varied only at amino acid 219 were oxidized by exposure to ozone. Differences in the absorption spectra (310–350 nm) between the two truncated rSP-A proteins, before and after protein oxidation, suggested allele-specific aggregation attributable to amino acid 2143. The SP-B SNP B1580_C, to be a risk factor for IPF smokers, was also shown to be a risk factor for other pulmonary diseases. The SP-C and SP-D SNPs and SP-B-linked microsatellite markers did not associate with IPF. These findings indicated that surfactant protein variants may serve as markers to identify subgroups of patients at risk. The observed alleles of SP-A and SP-D in association with various diseases are summarized in Table 43.1. Different alleles of these genes seem to predispose the individuals to various diseases. A logical explanation seems to be that different SNPs lead to different alterations in function or expression. However, common SNPs predispose Caucasians to RDS and Mexicans to TB. Similarly, common SNPs predispose the Indian population to ABPA and TB. Furthermore, Met11 SP-D allele is predisposing Mexicans to TB and Finns to RSV infection. It is also interesting to note that some of the alleles of SP-A interact with other alleles of SP-A and SP-B and thus increase the susceptibility of subjects to a disease (Kishore et al. 2005).
2.5 Cystic Fibrosis
Cystic fibrosis (CF) is an inherited disorder of CFTR gene, a chloride ion channel. The lack of this channel causes reduced water content of secretions. This affects the mucus secreted as part of the lung’s defence and creates sticky, viscous mucus. In patients with CF, neutrophils are recruited in excess to the airways yet pathogens are not cleared and the patients suffer from chronic infections. In CF, the disease-causing gene has been clearly identified as the CF transmembrane conductance regulator gene, but genetic variants of the MBP and SP-A have been associated with disease severity in CF. Allele associations and allele interaction of surfactant protein genes in relation to RDS have been discussed (Floros and Fan 2001). Studies have shown a deficiency of SP-A in airway fluids from patients with CF and other inflammatory pulmonary conditions. Findings suggest that the neutrophil serine proteases cathepsin G and/or elastase and/or proteinase-3 may contribute to degradation of SP-A and SP-D, thereby diminishing innate pulmonary antimicrobial defence (Rubio et al. 2004; von Bredow et al. 2001, 2003).
The dramatic decrease of SP-A and SP-D in the presence of normal surfactant phospholipid may be a mechanism underlying the relative ineffectiveness of cellular inflammatory response in killing invading bacteria in lungs of patients with CF. In bronchoalveolar lavage fluids (BALFs), although SP-A levels tend to decline in CF patients compared with non-CF, and the decline was only significant in presence of bacterial infection. Among CF patients, SP-A concentrations in BALF were inversely related to inflammation and age (Hull et al. 1997; Noah et al. 2003). Reports suggest that decreasing protease activity and increasing collectin activity may be beneficial in early CF (Alexis et al. 2006; Baker et al. 1999).
However, both, SP-D and TNF-α, are significantly increased in CF patients compared with patients of allergic fungal rhinosinusitis (AFRS), suggesting activation of both innate immunity and Th1-mediated inflammation and potential correlation between SPs and downstream adaptive immune responses (Skinner et al. 2007). Rat SP-D is highly resistant to degradation by a wide range of proteolytic enzymes. Patients with CF and chronic rhinosinusitis (CRS) with nasal polyposis demonstrated elevated SP-A1, -A2, and -D. While in patients with AFS, SP-A1, SP-A2, and SP-D, were not significantly different, these proteins are up-regulated in various forms of CRS, particularly in CF-CRS (Woodworth et al. 2007).
2.6 Familial Interstitial Lung Disease
Amin et al. (2001) studied the development of chronic lung injury in a familial form of ILD. An 11-year-old girl, her sister, and their mother who were diagnosed with chronic ILD were negative for SP-C and decreased levels of SP-A and SP-B in BALF. Lung biopsy from both children demonstrated a marked decrease of pro-SP-C in the alveolar epithelial cells but strong staining for pro-SP-B, SP-B, SP-A, and SP-D. The apparent absence of SP-C and a decrease in the levels of SP-A and SP-B were related to familial ILD. Several linkage and association studies have been done using SPs genes as markers to locate pulmonary disease susceptibility genes, but few have studied markers systematically in different ethnic groups.
3 Connective Tissue Disorders
3.1 Systemic Sclerosis
Significant progress is being made in terms of understanding the pathogenesis and various options for therapy of systemic sclerosis patients whose disease course is complicated by ILD. The significance of serum SP-A, SP-D and KL-6 for diagnosis and treatment of ILD in connective tissue disorders has been evaluated by different workers. Serum KL-6 and SP-D levels are more specific and useful markers for diagnosis and evaluation of ILD compared with serum LDH in connective tissue disorders (Ogawa et al. 2003; Suematsu et al. 2003). Characteristics or disease activity of early ILD has been evaluated in subjects. In abnormal group, curvilinear subpleural lines or thickened interlobular and intralobular lines were observed more frequently in lower lung fields and SP-A and SP-D were higher in true abnormalities group than in control group. True parenchymal abnormalities in posterior subpleural aspect of lung may indicate early ILD activity (Al-Salmi et al. 2005; Kashiwabara 2006). Since higher levels of SP-A and SP-D are associated with more severe lung function impairment at presentation, and better recovery over time, Janssen et al. (2005) suggested that SP-A, SP-D and KL-6 are especial markers of disease activity. Nevertheless, serum pulmonary and activation-regulated chemokine (PARC) levels may be more useful marker for active PF in systemic sclerosis (SSc) (Kodera et al. 2005) since elevated PARC values correlated more sensitively reflecting the PF activity than serum KL-6 or SP-D levels.
In lung fibrosis in patients with SSc and inflammatory myopathies, KL-6, von Willebrandt factor (vWF), soluble E-selectin (sES), SP-D are good surrogate factors of PF but cannot replace conventional diagnostic procedures. However, these markers are suitable for the assessment of progression and severity of PF in systemic autoimmune disorders once the diagnosis is established (Kumánovics et al. 2008). Takahashi et al. (2006b) indicated that elevated levels of serum SP-A and SP-D reflect the presence of ILD and the combination of SP-D and X-ray contributes to reduce the risk of clinicians overlooking ILD complicated by SSc (Highland and Silver 2005; Yanaba et al. 2004).
Maeda et al. (2001) compared serum SP-D in collagen diseases such as systemic scleroderma (SSd), scleroderma spectrum disorders (SSD), systemic lupus erythematodes (SLE), Sjogren syndrome (Sjs), dermatomyositis (DM), rheumatoid arthritis (RA), and dermatitis (DE) as a control. Patients with SSc possess higher levels of SP-D than those with other collagen diseases and dermatitis, which may correspond to severity of pulmonary fibrosis (Maeda et al. 2001). The basic and clinical studies of SSc patients with ILD are yielding promising data that may be translated in to more effective diagnostic and therapeutic strategies Although the SP-D level in sera of patients with polymyositis/dermatomyositis (PM/DM) is significantly elevated, the serum SP-D in patients with ILD was still higher than those without ILD, suggesting that serum SP-D level is a useful marker for ILD in patients with PM/DM (Ihn et al. 2002). However, there is a need to investigate whether another connective tissue disease has developed when laboratory findings cannot be explained by usual clinical course of an existing connective tissue disease (Ishiguro et al. 2007).
3.2 Sarcoidosis
Sarcoidosis also called sarcoid, Besnier-Boeck disease or Besnier-Boeck-Schaumann disease, is a disease in which abnormal collections of chronic inflammatory cells form as nodules in multiple organs. KL-6, SP-A and SP-D levels in BALF were increased in pulmonary sarcoidosis. Since these markers are specifically derived from epithelial cells, it is considered that KL-6 and SP-D levels are reflecting damage or release of these markers from epithelial cells due to the inflammatory response. Among serum Clara cell 16 (CC16), KL-6, and SP-D as markers of ILD, and their ability to reflect pulmonary disease severity and prognosis in sarcoidosis, KL-6 is the best marker in differentiating patients from healthy controls (Günther et al. 1999; Hamm et al. 1994; Janssen et al. 2003; Kunitake et al. 2001). The median amounts of SP-A in BAL fluid in control subjects was 2.82 mg/L (range, 0.92–5.17 mg/L). In comparison to control, SP-A in patients with asthma had a lower value of SP-A, which remained unchanged in patients with pulmonary sarcoidosis (van de Graaf et al. 1992). In contrast, SP-A levels in BAL fluids from patients with sarcoidosis were markedly higher than in control subjects and it was comparable with patients of hypersensitivity pneumonitis (HP). In both conditions, SP-A+ alveolar macrophages were increased (Günther et al. 1999; Hamm et al. 1994).
The serum levels of SP-A in patients with IPF (205 ± 23 ng/mL) and PAP (285 ± 23 ng/mL) were significantly higher than those in healthy controls (45 ± 3 ng/mL). In patients of sarcoidosis, pneumonia, and tuberculosis SP-A values were 52 ± 27 ng/mL, 65 ± 11 ng/mL, and 49 ± 23 ng/mL, respectively. The SP-A appears to circulate in the bloodstream as a complex with Ig in IPF and in PAP (Kuroki et al. 1993).
4 Pulmonary Alveolar Proteinosis
A diffuse lung process of unknown etiology is characterized by the presence of alveolar spaces filled with amorphous eosinophilic (but sometimes basophilic) PAS-positive material of predominantly phospholipid nature in alveolar lumina. It is generally regarded as type of response to alveolar injury and results from accumulation of surfactant apoprotein through either: increased secretion by granular pneumocytes, or abnormal uptake and handling by alveolar macrophages. The prominent increase of SP-A and SP-D in BAL fluids and sputum is diagnostic for pulmonary alveolar proteinosis (PAP) (Kuroki et al. 1998; Brasch and Müller 2004; Takahashi et al. 2006a). There are reports about polymorphisms and mutations on the surfactant protein genes, especially SP-B that may be associated with congenital alveolar proteinosis.
4.1 Idiopathic Pulmonary Alveolar Proteinosis
SP-A in BALF of PAPs patients is significantly increased in comparison to normal volunteers and hence can be used as a diagnostic tool in the clinical laboratory (Brasch et al. 2004; Honda et al. 1996). PAP is a rare lung disorder and can be caused by inactivation of either granulocyte-macrophage colony-stimulating factor (GM-CSF) or GM receptor common β-chain (βc) genes in mice [GM−/−, βc−/−], demonstrating a critical role of GM-CSF signaling in surfactant homeostasis. Studies demonstrate abnormal accumulation of SP-A and SP-D in air spaces of patients with PAP (Crouch et al. 1993) and the precursors of SP-B, SP-B and SP-C. Although lung histology in βc−/− and GM−/− mice was indistinguishable, distinct differences were observed in surfactant phospholipid and surfactant protein concentrations in lungs of βc−/− and GM−/− mice. The defect in clearance was significantly more severe in GM−/− than in βc−/− mice. GM-CSF concentrations, increased in BALF but not in serum of βc−/− mice, were consistent with a pulmonary response to the lack of GM-CSF signaling. The observed differences in surfactant metabolism suggest the presence of alternative clearance mechanisms regulating surfactant homeostasis in mice and may provide a molecular basis for the range in severity of PAP symptoms (Reed et al. 2000). In a young patient with idiopathic PAP, the enhanced serum anti-GM-CSF antibody level demonstrated a striking difference in the distribution of SP-A and SP-D in intra-alveolar substance with idiopathic PAP (Ohtsuki et al. 2008; Kobayashi et al. 2008b).
Evidence suggests that not only an impairment of surfactant clearance by alveolar macrophages, but also an abnormal secretion of transport vesicles containing precursors of SP-B (but not SP-C) and an insufficient palmitoylation of SP-C, which may lead to the formation of di- and oligomeric SP-C forms, play a role in the pathogenesis of pulmonary alveolar proteinosis.
4.2 Structural Changes in SPs in PAP
The primary structures of human pulmonary SPs isolated from lung lavage of patients with alveolar proteinosis demonstrate significant differences from lung surfactant proteins isolated from lungs of healthy individuals. In contrast to SP-A from normal lungs, PAP-SP-A was shown to contain large amounts of non-reducable cross-linked β chains, where as proteinosis SP-B showed a significantly increased molecular weight by approx. 500 Da for the unreduced protein dimer. In contrast, SP-C from proteinosis patients was modified by (1) partial or even complete removal of palmitate residues and (2) additional N-terminal proteolytic degradation (Voss et al. 1992).
Pathophysiological structural modifications in SP-A seemed to occur in the alveolar space, and may lead to a reduced surfactant function (Voss et al. 1992). Multimerized form of SP-A oligomer (alveolar proteinosis protein-I, APP-I) has been detected besides the normal-sized octadecamer (APP-II) in SP-As isolated from PAP patients. Analysis of APP revealed that it was composed of two proteins. The Mr of APP-I and APP-II were 1.65 MDa and 0.93 MDa, respectively. APP-I and APP-II showed almost identical amino acid compositions. Electron microscopy revealed that APP-II was a hexameric particle, presumably consisting mainly of octadecamers whose diameter was approximately 30 nm. In contrast, APP-I was made of multimerized larger aggregates whose diameter appeared to be about 70–90 nm. Both APP-I and APP-II retained the abilities to bind DPPC. Reconstitution experiments with porcine SP-B and phospholipids revealed that multilamellated membranes in structures formed from APP-I consisted of several layers of doubled unit membranes. APP-I failed to form tubular myelin structures. In contrast, APP-II formed well-formed lattice structures seen in tubular myelin The multimerized form of human SP-A oligomer exhibits the reduced capacity to regulate phospholipid secretion from type II cells, and lower affinity to bind to type II cells. It is to be reminded that the integrity of a flower-bouquet-like octadecameric structure of SP-A oligomer is important for the expression of full activity of this protein, indicating the importance of the oligomeric structure of mammalian lectins with collagenous domains. Thus there exists an abnormal multimerized form of SP-A oligomer in the alveoli of patients with PAP that exhibits abnormal function on phospholipid membrane organization (Hattori et al. 1996a, b).
In alveolar proteinosis, cholesterol/disaturated phospholipid ratios (CHOL/DSP) are invariably elevated, whereas the SP-A/DSP and SP-B/DSP ratios are generally elevated. Because the SP-B/SP-A ratio was normal in all cases, it was suggested that structural changes to the proteins occurred secondarily and that caution must be used in comparing functional data derived using SP-A obtained from patients with PAP (Doyle et al. 1998). The major part of SP-A from a proteinosis patient consisted of SP-A2 gene product while SP-A1 gene product was present in only a small amount. The disulfide bridges in the carbohydrate recognition domain were identified to be in the 1–4, 2–3 pattern common for collectins. Interchain disulfide bridges were discovered between two Cys-48 residues and cysteine residues in the N-terminal region. However, the exact disulfide bridge connections within the bouquet-like ultrastructure could not be established (Berg et al. 2000).
5 Respiratory-Distress Syndrome and Acute Lung Injury
5.1 ARDS and Acute Lung Injury
Acute respiratory distress syndrome (ARDS), also known as respiratory distress syndrome (RDS) or adult respiratory distress syndrome (in contrast with IRDS) is a serious reaction to various forms of injuries to lung. ARDS is caused by a variety of direct and indirect issues. It is characterized by inflammation of lung parenchyma leading to impaired gas exchange with concomitant systemic release of inflammatory mediators causing inflammation, hypoxemia and frequently resulting in multiple organ failure. A less severe form is called acute lung injury (ALI). Clinical and biochemical evidences suggest that the etiology of RDS is multifactorial with a significant genetic component. There are reports about polymorphisms and mutations on the surfactant protein genes, especially surfactant proteins-B that may be associated with RDS, ARDS, and congenital alveolar proteinosis. The measurement of SP-A and SP-D in amniotic fluids and tracheal aspirates reflects lung maturity and the production level of the lung surfactant in infants with RDS. The SP-A concentrations in BAL fluids are significantly reduced in patients with ARDS and also in patients at risk to develop ARDS (Kuroki et al. 1998; Takahashi et al. 2006a). Patients with low concentrations of SP-A and SP-B in the BAL are at risk for ARDS before onset of clinically defined lung injury, though the SP-D concentrations remain in normal range. Thus, SP abnormalities occur before and after the onset of ARDS, and the responses of SP-A, SP-B, and SP-D differ in important ways. However, plasma SP-D is a valuable biomarker in ALI/ARDS and SP-A increases during the early phase of ARDS, including some molecular alteration followed by decrease during the late phase (Endo et al. 2002; Kuroki et al. 1998; Takahashi et al. 2006b; Zhu et al. 2001).
Elevated level of SP-A has also been reported in the sera of patients with acute cardiogenic pulmonary edema (APE) and in patients with ARDS relative to healthy subjects and ventilated patients with no cardio-respiratory disease. Serum SP-A was inversely related to blood oxygenation and to static respiratory system compliance both at the time of patient’s entry into the study and during the course of admission. Since SP-B is synthesized as a precursor smaller than alveolar SP-A, Doyle et al. (1995, 1997) suggested that immunoreactive SP-B that enters more readily than SP-A, is cleared acutely, and provides a better indicator of lung trauma (Shimura et al. 1996).
Prematurely born infants can develop the neonatal RDS because of a deficiency of pulmonary surfactant. At autopsy RDS lungs lacked tubular myelin and had decreased immunoreactivity for antisera to SP-A, an important component of tubular myelin. Therefore, a role for SP-A in the conversion of lamellar bodies to tubular myelin and in the pathogenesis of RDS was proposed. It was postulated that if SP-A is indeed necessary for the conversion of lamellar bodies to tubular myelin, in RDS either there is a deficiency of adequate amounts of functional SP-A, or some other important component of surfactant is missing (deMello et al. 1993). Mechanical ventilation is the main modality of treatment of ARDS. On mechanical ventilation, there is a progressive increase in SP-A levels in patients with ARDS, and may be one of the contributors for recovery in ARDS. A significant increase within the first 4 days was found in those infants who survived, whereas no such change was found in those infants who died (Balamugesh et al. 2003; Stevens et al. 1992). Intratracheal aerosolization of LPS in rats produces typical features of human ARDS. The SP-D binds inhaled LPS-endotoxin in vivo, which may help to protect the lung from endotoxin-induced disease (van Rozendaal et al. 1999). The SP-D was reduced in lung of young rats following ALI at early stage and early administration of Dex could reverse the SP-D content (Shu et al. 2007). SP-A in sera of cord blood from infants born at gestational ages <32 weeks with RDS was 15.1 ng/mL compared to without RDS (5.8 ng/mL) and significantly related to the non-RDS outcome (Cho et al. 2000). Shimoya et al. (2000) suggested that IL-6 elevation in fetuses with chorioamnionitis promotes fetal lung maturation by inducing SP-A synthesis, thereby decreasing the incidence of RDS in the preterm neonates.
Acute Lung Injury (ALI): Plasma SP-A, but not SP-D, was higher in patients with fewer days of unassisted ventilation and in patients with an absence of intact alveolar fluid clearance. In contrast, pulmonary edema fluid SP-D, but not SP-A, was lower in patients with worse oxygenation. Reduced pulmonary edema fluid SP-D and elevated plasma SP-A concentrations at the onset of ALI may be associated with more severe disease and worse clinical outcome and may serve as valuable biochemical markers of prognosis (Cheng et al. 2003). The BALF proteome analysis showed the presence of several isoforms of SP-A, in which an N-non-glycosylierte form and several proline hydroxylations were identified (Bai et al. 2007). In the plasma and edema fluid, protein profile of ALI patients showed multiple qualitative changes. Nearly all ALI patients also had protein spots that indicated truncation or other posttranslational modifications (Bowler et al. 2004).
5.2 Bronchopulmonary Dysplasia (BPD)
The pathophysiology of bronchopulmonary dysplasia (BPD) as an inflammatory disorder, secondary to neonatal RDS represents a major complication of prematurity. Maximum SP-A and anti-SP-A antibodies (SAS) immune complex values between 2 and 4 weeks after birth correlate with subsequent development of BPD independently and may be useful in analyzing the course and outcome of neonatal RDS, in particular the likelihood of subsequent development of BPD (Strayer et al. 1995). Weber et al. (2000) investigated an association of polymorphisms of SP-A1 and SP-A2 encoding genes and the risk of BPD in Caucasian preterm infants below 32 weeks of gestation matched for immaturity and year of birth. BPD was defined as oxygen dependency or need for mechanical ventilation at day 243. A significantly increased frequency of SP-A1 polymorphism 6A6 in infants was associated with BPD compared with controls. In addition to established risk factors for BPD, 6A6 polymorphism for SP-A1 gene is an independent co-factor.
BPD_28D (O2 dependency at 28 days of life) and BPD_36W (O2 dependency at 36 week post-menstrual age) are diseases of prematurely born infants exposed to mechanical ventilation and/or oxygen supplementation. Genetic variants of SP-A, B, C, and D and SP-B-linked microsatellite markers are risk factors in BPD. Significant associations were observed for alleles of SP-B and SP-B-linked microsatellite markers, and haplotypes of SP-A, SP-D, and SP-B. Unlike SP-A, SP-D does not contribute to lowering surface tension. SP-D-deficient mice have no respiratory abnormalities at birth, but it causes development of emphysema and predisposition to specific infections. No human infant or child with respiratory distress and mutation in the SP-D gene has been identified (Yurdakök 2004). Studies in larger sample size are warranted to confirm these observations and delineate genetic background of BPD subgroups (Pavlovic et al. 2006).
5.2.1 SP-A Deficiency in Primate Model of BPD with Infection
In a baboon model of hyperoxia-induced BPD and superimposed infection, animals constituting a group- pro re nata (PRN) were delivered by hysterotomy at 140 days gestational age and ventilated on clinically appropriate oxygen for a 16-day experimental period and served as controls. Immunostaining with SP-A, SP-B, and SP-C antibodies showed variable staining patterns. The study demonstrated that a deficiency of SP-A mRNA expression persists in chronic lung injury and variable protein staining patterns are manifested depending upon the underlying pathology (Coalson et al. 1995; King et al. 1995).
Awasthi et al. (1999) measured SP-A and SP-D levels and their mRNAs in three groups of animals: (1) nonventilated premature baboon fetuses; (2) neonatal baboons delivered prematurely at 140 d gestation age (ga) and ventilated with PRN O2; (3) animals of same age ventilated with 100% O2 to induce chronic lung injury. In chronic lung injury, SP-A is significantly reduced in alveolar space. SP-D concentration in lavage was nearly equal to that in normal adults, but the total collectin pool in lavage was still significantly reduced. Because these collectins may bind and opsonize bacteria and viruses, decrements in their amounts may present additional risk to those premature infants who require prolonged periods of ventilatory support (Awasthi et al. 1999). Reduced SP-D expression in BAL fluid was associated with progression of bronchial dysplasia in heavy smokers. SP-D levels in BAL fluid may serve a potential biomarker to identify smokers who are at risk of early lung cancer (Sin et al. 2008b). Cheng et al. (2003) proved the hypothesis that reduced pulmonary edema fluid SP-D and elevated plasma SP-A concentrations at onset of ALI may be associated with more severe disease and worse clinical outcome and may serve as valuable biochemical markers of prognosis (Cheng et al. 2003).
6 Chronic Obstructive Pulmonary Disease (COPD)
6.1 COPD as a Group of Diseases
Obstructive lung disease is a category of respiratory disease characterized by airway obstruction. Chronic obstructive pulmonary disease (COPD), also known as chronic obstructive airways disease (COAD) or chronic airflow limitation (CAL) is a group of illnesses characterised by airflow limitation that is not fully reversible. The flow of air into and out of the lungs is impaired. The COPD is characterized by chronic inflammation. It is most likely the result of complex interactions of environmental and genetic factors. Term COPD includes the conditions of emphysema and chronic bronchitis although most patients with COPD have characteristics of both conditions to varying degrees. Asthma being a reversible obstruction of airways is often considered separately, but many COPD patients also have some degree of reversibility in their airways. The most common cause of COPD is cigarette smoking. COPD may also be caused by breathing in other particles and gases. Diagnosis of COPD is established through spirometry and chest X-ray although other pulmonary function tests can be helpful. Emphysema can only be seen on CT scan. COPD is generally irreversible although lung function can partially recover if the patient stops smoking. α1-antitrypsin deficiency is a rare genetic condition that results in COPD (particularly emphysema) due to lack of antitrypsin protein which protects fragile alveolar walls from protease enzymes released by inflammatory processes.
The prevalence of COPD is age-dependent, suggesting an intimate relationship between the pathogenesis of COPD and aging. Genetic polymorphism in SP-A is associated with the development of COPD in Chinese Hans. The genotypes of patients with COPD and healthy smoking subjects as controls for SP-A gene showed that in COPD group, the frequencies of +186 locus genotypes AA, AG and GG were 86.4%, 12.5% and 1.1%i respectively; compared to 66.7%, 27.6% and 5.7% in control group. The frequencies of polymorphic genotypes at +655 locus and +667 loci showed no significant difference between the COPD group and control group (Xie et al. 2005).
6.1.1 Serum SP-A in COPD and Its Relation to Smoking
SP-A occurs physiologically in small amounts in blood. Tobacco smoke induces increased alveolo-capillary leakage of SPs into blood and its level in blood may help in the assessment of lung injury caused by smoke. SP-A is occasionally elevated in non-ILD pulmonary patients. Serum SP-A increased in current smokers than in never- or ex-smokers and in COPD and pulmonary thromboembolism than in other diseases. Serum SP-D and KL-6 were unaffected by smoking. Therefore, different baseline levels of serum SP-A need to be established for smokers and non-smokers. Serum SP-A may be a useful marker for predicting COPD in the preclinical stage (Behera et al. 2005; Kobayashi et al. 2008a). Different alleles of SP-A and SP-D associated with various diseases have been summarized by Kishore et al. (2005) and given in Table 43.2. Analysis between COPD and smokers revealed several COPD susceptibility alleles (AA62_A, B1580_C, D2S388_5), based on an odds ratio (OR > 2.5). Results indicate that surfactant protein alleles may be useful in COPD by either predicting the disease in a subgroup and/or by identifying disease subgroups that may be used for therapeutic intervention (Guo et al. 2001).
Proteome research revealed increased levels of SP-A in COPD but not in normal or fibrotic lung. Furthermore, elevated SP-A protein levels were detected from the induced sputum supernatants of COPD patients. The levels of other surfactant proteins (SP-B, SP-C, SP-D) were not altered. It is suggested that SP-A is linked to the pathogenesis of COPD and can be considered as a potential COPD biomarker (Ohlmeier et al. 2008). Toxic metals and transition elements are detectable in exhaled breath condensate (EBC) of studied subjects (Mutti et al. 2006).
6.1.2 SP-D Is an Ideal Biomarker in COPD
In COPD, SP-D is an ideal biomarker that is produced mostly in lungs and can be measured in the peripheral circulation. It changes with the clinical status of the patient and has inherent functional attributes that suggest a possible causal role in pathogenesis of disease (Sin et al. 2008b, c).
In a multivariable linear regression model, COPD was independently associated with lower SP-D levels. Given the importance of this molecule in lung, low levels may play a role in the pathogenesis and/or progression of COPD (Sims et al. 2008). Inhaled corticosteroids alone or in combination exhibited partial systemic anti-inflammatory effects, reducing significantly only SP-D serum levels. ICS in conjunction with long-acting β2-adrenergic agonist significantly reduced serum SP-D levels. These drugs reduce lung-specific but not generalized biomarkers of systemic inflammation in COPD. Hydrofluoroalkane-beclomethasone dipropionate (HFA-BDP) controls eosinophilic inflammation, including in distal airways, more effectively than fluticasone propionate (FP) Diskus (Ohbayashi and Adachi 2008; Sin et al. 2008a).
6.2 Emphysema
Emphysema is a chronic pulmonary disease marked by an abnormal increase in size of air spaces. Pulmonary emphysema, a major component of COPD, is pathologically characterized by destructive alterations in pulmonary architectures as a result of persistent inflammation. Emphysema may be a dynamic disease process in which alveolar wall cell death and proliferation are repeated. The decrease of surfactant protein secreted by the alveolar type II cell is one of the important causes of limiting air of pulmonary emphysema and the changes of SP-A may be related to emphysematous changes in the lung. Cigarette smoke and LPS alter lung SP-A gene activity and protein homeostasis (Hu et al. 2008). Mice deficient in SP-D−/− develop progressive emphysema with age. SP-D gene-targeted mice develop severe pulmonary lipidosis, and foamy macrophage infiltrations. By lowering surface tension at the air-water interface in the surfactant deficient premature lung, exogenous surfactant replacement therapy for neonatal RDS has been highly successful in decreasing mortality after preterm birth. It has emerged that SP-A and SP-D have additional roles in host defence distinct from the surface tension lowering effects of surfactant. Recombinant forms of SP-D could be useful therapeutically in attenuating inflammatory processes in neonatal chronic lung disease, cystic fibrosis, and emphysema (Clark and Reid 2003).
6.3 Allergic Disorders
6.3.1 Allergic Inflammation in Asthma
Asthma is an obstructive lung disease where the bronchial tubes (airways) are extra sensitive (hyperresponsive). The airways become inflamed and produce excess mucus and muscles around the airways tighten making the airways narrower. Asthma is usually triggered by breathing in things present in air such as dust or pollen that produces an allergic reaction. It may be triggered by other things such as an upper respiratory tract infection, cold air, exercise or smoke. Asthma is diagnosed by the characteristic pattern of symptoms. A peak flow meter can record variations in the severity of asthma over time. Spirometry can provide an assessment of the severity, reversibility, and variability of airflow limitation, and help confirm the diagnosis of asthma. Significant changes occur in levels of SP-A and SP-D during the asthmatic response in animal models as well as in asthmatic patients. The impact of the SP-A and SP-D on asthmatic allergic inflammation and vice versa has been reviewed (Hohlfeld et al. 2002). Serum SP-D concentrations are affected in allergic patients and correlate with changes in allergic airway inflammation. Serum SP-D levels may give additional information, beside bronchial hyper-responsiveness (BHR) and sputum eosinophils, about the degree of bronchial inflammation in allergic patients (Koopmans et al. 2004).
6.3.1.1 Immunoregulatory Roles of SP-A and SP-D
Studies on allergen-sensitized murine models and asthmatic patients show that SP-A and SP-D can: specifically bind to aero-allergens; inhibit mast cell degranulation and histamine release; and modulate the activation of alveolar macrophages and DCs during the acute hypersensitive phase of allergic response (Erpenbeck et al. 2005; Wang et al. 1998). They also can alleviate chronic allergic inflammation by inhibiting T-lymphocyte proliferation as well as increasing phagocytosis of DNA fragments and clearance of apoptotic cell debris. Furthermore, it has emerged, from the studies on SP-D-deficient mice, that, when these mice are challenged with allergen, they develop increased eosinophil infiltration, and abnormal activation of lymphocytes, leading to the production of Th2 cytokines. Intranasal administration of SP-D significantly attenuated the asthmatic-like symptoms seen in allergen-sensitized wild-type, and SP-D-deficient, mice. These findings provide a new insight of role that surfactant proteins play in handling environmental stimuli and in their immunoregulation of airway inflammatory disease (Wang and Reid 2007).
Both SP-A and SP-D can inhibit histamine release in the early phase of allergen provocation and suppress lymphocyte proliferation in the late phase of bronchial inflammation, the two essential steps in the development of asthmatic symptoms (Wang et al. 1998). Studies suggest that the increased levels of SP-A and D may play a protective role in an allergic inflammation in the pathogenesis of bronchial asthma. Structural remodelling of airways in asthma that follows inflammation may be affected by SP-D-mediated effects on immune response. SP-D accumulation is increased in this model of allergen-induced eosinophilia, both in upper and lower airways (Cheng et al. 2000; Kasper et al. 2002). SP-D gene-deficient mice (Sftpd −/−) have an impaired systemic Th-2 response at baseline and reduced inflammation and airway responses after allergen exposure. Translational studies revealed that a polymorphism in SFTPD gene was associated with lower atopy and possibly asthma susceptibility. Thus, SP-D-dependent innate immunity influences atopy and asthma (Brandt et al. 2008). Dex significantly down-regulates SP-D in allergic airways and lavage fluid. In addition, Dex promoted airway expression of vitamin D-binding protein, heptoglobin and α1-antitrypsin (Zhao et al. 2007).
Serum SP-D is increased in acute and chronic inflammation in mice. Profiles of SP-A and SP-D in acute and chronic inflammation indicated that serum SP-D can serve as a biomarker of lung inflammation in both acute and chronic lung injury in mice (Fujita et al. 2005). Because of their capability to directly inhibit T-cell activation and T-cell-dependent allergic inflammatory events, SP-A and SP-D may be significant contributors to the local control of Th-2 type inflammation in the airways. SP-D is able to reduce the immediate allergen-induced mediator release and the early bronchial obstruction in addition to its effects on airway inflammation and bronchial hyperresponsiveness in an A. fumigatus mouse asthma model. Thus, SP-D not only reduces allergen-induced eosinophilic inflammation and airway hyper-responsiveness but also provides protection against early airway obstruction by inhibition of early mediator release (Erpenbeck et al. 2006; Takeda et al. 2003). However, mice sensitized and challenged with either A. fumigatus or OVA increased SP-D levels in their lung. Allergen exposure induced elevation in SP-D protein levels in an IL-4/IL-13-dependent manner, which in turn, prevents further activation of sensitized T cells. This negative feedback regulatory circuit could be essential in protecting the airways from inflammatory damage after allergen inhalation (Haczku et al. 2006). Haczku (2006) support the hypothesis that SP-A and SP-D have a role in regulation of allergic airway sensitization.
6.3.1.2 Murine Model of Asthma
Dust mite allergens can directly activate alveolar macrophages (AΦs), induce inflammatory cytokines, and enhance T-helper type 2 cytokine production. The SP-D is able to bind mite allergens and alleviates allergen-induced airway inflammation and may be an important modulator of allergen-induced pulmonary inflammation (Liu et al. 2005a). There is marked reduction in SP-A and SP-D levels in the BALF of dust mite (Dermatophagoides pteronyssinus, Der p)-sensitized BALB/c mice after allergen challenge. Both SP-A and SP-D were able to suppress Der p-stimulated intrapulmonary lymphocyte proliferation of naïve mice with saline or allergen challenge, or of Der p-sensitized mice with saline challenge. On the contrary, this suppressive effect was mild on lymphocytes from sensitized mice after allergen challenge. These results indicated the involvement of pulmonary surfactant proteins in the allergic bronchial inflammation of sensitized mice (Wang et al. 1996, 2001). Both SP-A and SP-D down-regulate the eosinophilic inflammation in murine asthma models and shift the cytokine profile towards a T helper cell type 1 response. In addition, they are effective at alleviating bronchial hyperresponsiveness. There is evidence of activation of innate immune system in asthma which results in the production of pro-inflammatory cytokines and may contribute to the pathogenesis of neutrophilic asthma (Simpson et al. 2007).
6.3.2 Chronic Sialadenitis and Chronic Rhinosinusitis
SP-A and mRNA and protein were detected in glands of patients with chronic sialadenitis. The expression in salivary glands of patients with chronic sialadenitis was significantly higher than from healthy salivary glands. SP-A immunoreactivity, localized in the epithelial cells and submucosal glands of paranasal sinus mucosa in normal and chronic sinusitis patients, was enhanced in chronic rhinosinusitis mucosa as compared with normal paranasal sinus mucosa (Lee et al. 2004, 2006). SP-A expression in human nasal tissue was correlated with symptoms suggestive of allergic rhinitis. (Wootten et al. 2006).
6.4 Interactions of SP-A and SP-D with Pathogens and Infectious Diseases
Microbial targets for SP-D include both Gram-positive and Gram-negative respiratory pathogens, influenza, and respiratory syncytial viruses, Cryptococcus neoformans, Pneumocystis carinii, and Aspergillus fumigatus. Both monocytes/macrophages and neutrophils express surface receptors that can interact with SP-D. The interactions between SP-D and microorganisms and in many instances immune cells promote both microbial aggregation and enhanced phagocytosis. SP-D has been shown to bind to a variety of bacteria, including rough strains of Salmonella Minnesota and E. coli as well as Klebsiella pneumoniae and Pseudomonas aeruginosa (Lim et al. 1994). SP-D also stimulates the phagocytosis of Pseudomonas aeruginosa (Restrepo et al. 1999). The interaction of SP-D with bacteria often results in CRD-dependent bacterial aggregation or agglutination. Unlike SP-A (van Iwaarden et al. 1994), SP-D does not bind to lipid A. It interacts with E. coli through the core polysaccharides and/or the O-specific antigens. The core region of the LPS of other gram-negative bacteria is broadly recognized by SP-D as well (Kuan et al. 1992). SP-D can be used as a biomarker for chronic periodontitis. As no significant associations of SFTPD gene polymorphisms could be detected, other mechanisms influencing SP-D serum/plasma expression might exist (Glas et al. 2008).
SP-D has been shown to bind to the influenza A virus, resulting in aggregation of the target (Hartshorn et al. 1996a). The binding and inhibition of hemagglutination was inhibited by chelation of calcium and by carbohydrates, suggesting that the interaction of SP-D with the virus was mediated via the CRD. SP-D also enhances the neutrophil uptake of the virus in a calcium-dependent manner (Hartshorn et al. 1997). Further enhanced antiviral and opsonic activity for influenza A virus was obtained by making a human MBP and SP-D chimera (White et al. 2000) (Table 43.1). The degree of multimerization of SP-D also appears to be important for its interactions with viruses (Brown-Augsburger et al. 1996; Hartshorn et al. 1996b). SP-D induces massive aggregation of influenza A virus particles (Hartshorn et al. 1996a). This massive agglutination of organisms could contribute to lung host defence by promoting airway mucociliary clearance, but it could also promote internalization by phagocytic cells. Recombinant SP-D inhibited RSV infectivity both in vitro and in vivo (Hickling et al. 1999; Le Vine et al. 2004), and reduced SP-D protein levels have been detected in RSV infection (Kerr and Paton 1999). A direct interaction between the yeast Candida albicans and SP-D confirms the importance of SP-D in innate immunity (van Rozendaal et al. 2000).
6.4.1 Distinct Effects of SP-A or -D Deficiency During Bacterial Infection
Surfactant proteins A and D expressed in respiratory tract bind bacterial, fungal and viral pathogens, enhancing their opsonization and killing by phagocytic cells. Clearance of bacterial pathogens including group B streptococci, Haemophilus influenza, Pseudomonas aeruginosa and viral pathogens, respiratory syncytial virus, adenovirus and influenza A virus, was deficient in SP-A−/− mice (Table 43.1). Mice lacking SP-A (SP-A−/−) or SP-D (SP-D−/−) and wild-type mice, infected with group B streptococcus or Haemophilus influenzae, are associated with increased inflammation and inflammatory cell recruitment in lung after infection. Although, decreased killing of group B streptococcus and H. influenzae was observed only in SP-A−/− mice but not in SP-D−/− mice, bacterial uptake by alveolar macrophages was reduced in both SP-A- and SP-D-deficient mice. Isolated alveolar macrophages from SP-A−/− mice generated significantly less, whereas those from SP-D−/− mice generated significantly greater superoxide and H2O2 compared with wild-type alveolar macrophages.
In SP-D−/− mice, bacterial killing was associated with increased lung inflammation and increased oxidant production. Where as, bacterial killing was decreased and associated with increased lung inflammation and decreased oxidant production in SP-A−/−, macrophage phagocytosis was decreased in both SP-A and SP-D deficient mice. SP-A deficiency was associated with enhanced inflammation and synthesis of pro-inflammatory cytokines. SP-D−/− mice cleared these bacteria as efficiently as wild-type mice; however, clearance of viral pathogens was deficient in SP-D−/− mice and associated with increased inflammation. Study suggests that SP-A and SP-D play distinct roles during bacterial infection of lung (LeVine et al. 2000, 2001).
Alloiococcus otitidis has been found to be associated with otitis media with effusion. SP-A and MBL interact with A. otitidis in Ca2+-dependent manner. Results demonstrate that A. otitidis is a ligand for SP-A and TLR2, and that the collectins enhance the phagocytosis of A. otitidis by macrophages, suggesting important roles of collectins and TLR2 in the innate immunity of the middle ear against A. otitidis infection (Konishi et al. 2006). Meningococcal disease occurs after colonization of nasopharynx with Neisseria meningitidis. Variation in genes of surfactant proteins affects the expression and function of SPs. Gene polymorphism resulting in substitution of glutamine with lysine at residue 223 in the CRD of SP-A2 increases susceptibility to meningococcal disease, as well as the risk of death (Jack et al. 2006). In contrast to defensive function, SP-D in BALF binds β-glucan onB. Dermatitidis and, blocks BAM access to β-glucan, thereby inhibiting TNF-α production. Thus, whereas BALF constituents commonly mediate antimicrobial activity,莔B. dermatitidis may utilize BALF constituents, such as SP-D, to blunt the host defensive reaction; this effect could reduce inflammation and tissue destruction but could also promote disease (Lekkala et al. 2006)
7 Pulmonary Tuberculosis
7.1 Enhanced Phagocytosis of M. tuberculosis by SP-A
During initial infection with M. tuberculosis, bacteria that reach the distal airspaces of lung are phagocytosed by AMΦs in presence of pulmonary surfactant. Studies indicated a direct interaction between SP-A and macrophage in mediating enhanced adherence of M. tuberculosis (Gaynor et al. 1995). Since, SP-A binds mannose, it was hypothesized that SP-A attaches to M. tuberculosis and serves as a ligand between M. tuberculosis and AΦs. Stokes et al. (1998) demonstrated that explanted alveolar AΦs do not efficiently bind M. tuberculosis in a serum-free system, although a small subpopulation of these AΦs could bind mycobacteria. In contrast, almost 100% of peritoneal AΦs bind mycobacteria under similar conditions. Evidence suggests that opsonic binding of M. tuberculosis by differentiated alveolar Mфs is mediated by complement and CR3, and that the poor binding by resident alveolar AΦs is due to their poor expression of CR3. Thus, attachment of M. tuberculosis to AΦs is an essential early event in primary pulmonary tuberculosis and SP-A helps in early capture and phagocytosis of M. tuberculosis by AΦs. Ferguson et al. (2002) provided evidence for specific binding of SP-D to M. tuberculosis and indicated that SP-D and SP-A serve different roles in the innate host response to this pathogen in lung.
7.1.1 Lipomannan and ManLAM are Major Mycobacterial Lipoglycans as Potential Ligands
The SP-A binds to M. bovis Bacillus Calmette-Guerin (BCG), the vaccinating strain of pathogenic mycobacteria, and also to a lesser extent to M. smegmatis, which indicates that SP-A does not discriminate virulent from nonpathogenic strains. Lipomannan and mannosylated lipoarabinomannan (ManLAM) are two major mycobacterial cell-wall lipoglycans, which act as potential ligands for binding of SP-A. Both the terminal mannose residues and the fatty acids are critical for binding. It appears that recognition of carbohydrate epitopes on lipoglycans by SP-A is dependent on the presence of fatty acids (Sidobre et al. 2000, 2002).
Rivière et al, (2004) claim that the hydrophobic aglycon part of ManLAM is associated to a supra-molecular organization of these complex molecules. Furthermore, the deacylated ManLAMs or the lipid-free mannosylated arabinomannans, which do not exhibit characteristic ManLAM activities, do not display this supra-molecularorganization. These observations suggest that the ManLAMs immunomodulatory activities might be associated to their particular organization. The critical micellar concentration of ManLAMs obviously supports the notion that this supra-molecularorganization may be responsible for the specific biological activities of these complex molecules (Rivière et al. 2004).
As indicated, the molecular recognition of ManLAM terminal mannose units by CRDs of SP-A depends on the presence of lipid moiety of ManLAMs associated to a characteristic supra-molecular organization of ManLAM complex. On the other hand, the deacylated ManLAM or the lipid-free mannosylated arabinomannans, which do not exhibit characteristic ManLAM activities, do not display this supra-molecular organization. Therefore the ManLAM immunomodulatory activities might be associated to their particular organization. The critical micellar concentration of ManLAM supports the notion that this supra-molecular organization is responsible for specific biological activities of these complex molecules.
Apa Glycoprotein on M. tuberculosis: A Potential Adhesion to SP-A: Although lipoglycan ManLAM is considered as the major C-type lectin target on mycobacterial surface, Ragas et al. (2007) identified Apa (alanine- and proline-rich antigenic) glycoprotein as new potential target for SP-A, which binds to purified Apa. Apa is associated to the cell wall for a long time to aid in the attachment of SP-A. Because, Apa seems to be restricted to the M. tuberculosis complex strains, it was proposed that it may account for selective recognition of complex strains by SP-A containing homologous functional domains.
SP-A Enhances M. avium Ingestion by Macrophages: Tuberculosis leads to immune activation and increased HIV-1 replication in lung. SP-A promotes attachment of M. tuberculosis to AΦs during infection with HIV. SP-A levels and attachment of M. tuberculosis to AΦs inversely correlate with peripheral blood CD4 lymphocyte counts (Downing et al. 1995). M. avium complex (MAC) is a significant cause of opportunistic infection in patients with AIDS. Once in lung, MAC can interact with SP-A. Work on pulmonary pathogens including M. bovis BCG suggests that SP-A participates in promoting efficient clearance of these organisms by AMs. Lopez et al. (2003) reported that SP-A can bind to and enhance the uptake of MAC by AΦs, similar to BCG and M. tuberculosis. However, unlike BCG and other pulmonary pathogens that are cleared in presence of SP-A via a NO-dependent pathway, macrophage-mediated clearance of MAC is not enhanced by SP-A.
Suppression of Reactive Nitrogen Intermediates by SP-A in AMs in Response to M. tuberculosis: Reactive nitrogen intermediates (RNIs) play a significant role in the killing of mycobacteria. RNI levels generated by AΦs were significantly increased when IFNγ-primed AΦs were incubated with M. tuberculosis. However, the RNI levels were significantly suppressed in presence of SP-A. Furthermore, incubation of deglycosylated SP-A with M. tuberculosis failed to suppress RNI by AΦs, suggesting that the oligosaccharide of SP-A, which binds to M. tuberculosis, is necessary for this effect. Pasula et al. (1999) showed that SP-A-mediated binding of M. tuberculosis to AΦs and decreased RNI levels may be one mechanism by which M. tuberculosis diminishes the cytotoxic response of activated AΦs.
7.2 SP-A Modulates Inflammatory Response in AΦs During Tuberculosis
There is a severe reduction in SP-A levels in BAL during tuberculosis only in the radiographically involved lung segments, and the levels returned to normal after 1 month of treatment. The SP-A levels were inversely correlated with the percentage of neutrophils in BAL fluid, suggesting that low SP-A levels were associated with increased inflammation in the lung. SP-A has pleiotropic effects even at low concentrations found in tuberculosis patients. This protein augments inflammation in presence of infection and inhibits inflammation in uninfected macrophages, protecting uninvolved lung segments from the deleterious effects of inflammation (Gold et al. 2004).
SP-A modulates phenotypic and functional properties of cells of adaptive immune response such as DCs and lymphocytes. Bone marrow-derived DCs generated in presence of SP-A fail to increase LPS-induced up-regulation of MHC class II and CD86 co-stimulatory molecule on DCs surface and behaves like “tolerogenic DCs”. SP-A may also induce tolerance by suppressing the proliferation of activated T lymphocytes (Hussain 2004). SP-A suppresses lymphocyte proliferation and IL-2 secretion, in part, by binding to its receptor, SP-R210. However, the mechanisms underlying this effect are not well understood. The effects of antibodies against the SP-A-binding (neck) domain (α-SP-R210n) or nonbinding C-terminal domain (α-SP-R210ct) of SP-R210 on human peripheral blood T cell immune responses against M. tuberculosis support the hypothesis that SP-A, via SP-R210, suppresses cell-mediated immunity against M. tuberculosis via a mechanism that up-regulates secretion of IL-10 and TGF-β1 (Samten et al. 2008). Role of SP-A and SP-D in linking innate and adaptive immunity to regulate host defense has been suggested by Wright (2005). Although both SP-A and SP-D can bind to T cells and directly inhibit proliferation, SP-A can also indirectly inhibit T-cell proliferation via suppression of dendritic cell (DC) maturation. SP-D has been shown to enhance antigen uptake and presentation. Taken together, these in vitro results suggest that the combined role of SP-A and SP-D is to modulate the immunologic environment of the lung so as to protect the host, yet thwart an overzealous inflammatory response that could potentially damage the lung and impair gas exchange (Wright 2005)
7.3 Marker Alleles in M. tuberculosis
Regression analyses of tuberculosis and tuberculin-skin test positive groups, on the basis of odds ratios, revealed tuberculosis susceptibility (DA11_C and GATA_3) and protective (AAGG_2) marker alleles. Similarly, between tuberculosis patients and general population control subjects, susceptibility 1A3, 6A4, and B1013_A and protective AAGG_1, and AAGG_7 marker alleles were observed. Moreover, interactions were seen between alleles 6A2 and 1A3 and between 1A3 and B1013_A. Studies indicate a possible involvement of SP alleles in tuberculosis pathogenesis (Floros et al. 2000). Malik et al. (2006) investigated polymorphisms in the SFTPA1 and SFTPA2 genes for association with tuberculosis in 181 Ethiopian families comprising 226 tuberculosis cases. Four polymorphisms, SFTPA1 307A, SFTPA1 776T, SFTPA2 355C, and SFTPA2 751C, were associated with tuberculosis. Additional subgroup analysis in male, female and more severely affected patients provided evidence for SFTPA1/2-covariate interaction. Among five intragenic haplotypes identified in SFTPA1 gene and nine identified in SFTPA2 gene, 1A3 was most significantly associated with tuberculosis susceptibility (Table 43.2).
SNPs in Collagen Region of SP-A2 as a Contributing Factor: Relation exists between polymorphisms in the collagen regions of SP-A2 genes and pulmonary tuberculosis. Seven SNPs (4 exonic and 3 intronic) were identified in collagen regions of SP-A1 and SP-A2 genes in Indian population. Two intronic polymorphisms, SP-A1C1416T and SP-A2C1382G showed significant association with pulmonary tuberculosis. A redundant SNPA1660G of SP-A2 gene showed significant association with pulmonary tuberculosis. This polymorphism, when existing along with a non-redundant polymorphism, SP-A2G1649C (Ala91Pro) resulted in a stronger association with pulmonary tuberculosis. The SNPs in collagen region of SP-A2 may be one of the contributing factors to the genetic predisposition to pulmonary tuberculosis (Madan et al. 2002).
7.4 Interaction of SP-D with M. tuberculosis
Since many mycobacteria are facultative intracellular pathogens, their ability to cause disease involves entry, survival and replication within host cells. Although much progress has been made in our understanding of entry by mycobacteria, we anticipate that clarification of role of entry in pathogenesis will require further application of newly developed molecular tools to dissect each of the proposed mechanisms.
SP-D is known to bind M. tuberculosis. Binding of SP-D to M. tuberculosis is calcium dependent, and carbohydrate inhibitable. The binding of SP-D to Erdman lipoarabinomannan is mediated by terminal mannosyl oligosaccharides of this lipoglycan. Incubation of M. tuberculosis with sub-agglutinating concentrations of SP-D leads to reduced adherence of bacteria to macrophages, whereas incubation of bacteria with SP-A leads to significantly increased adherence to monocyte-derived macrophages. Ferguson et al. (2002) provided evidence for specific binding of SP-D to M. tuberculosis and indicated that SP-D and SP-A serve different roles in the innate host response to this pathogen in lung. Further studies provide direct evidence that inhibition of phagocytosis of M. tuberculosis affected by SP-D occurs independently of aggregation process. SP-D limits the intracellular growth of bacilli in macrophages by increasing phagosome-lysosome fusion but not by generating a respiratory burst (Ferguson et al. 2006). Results also provide evidence that SP-A and SP-D enhance mannose receptor-mediated phagocytosis of M. avium by macrophages (Kudo et al. 2004). Virulent and attenuated M. tuberculosis strains bind best to immobilized SP-A (Hall-Stoodley et al. 2006). Mycobacterium avium has developed numerous mechanisms for entering mononuclear phagocytes. The SP-A, and SP-D, exhibit a concentration-dependent binding to M. avium. Studies provide evidence that SP-A and SP-D enhance mannose receptor-mediated phagocytosis of M. avium by macrophages (Kudo et al. 2004).
7.5 Association of SPs with Diabetes
Insulin decreased SP-A gene transcription in human lung epithelial cells (Miakotina et al. 2002). Alveolar type II cells and nonciliated bronchiolar epithelial (Clara) cells in lungs of rats with diabetes have decreased SP-A, but increased mRNA. This is on account of differential expression in the level of SP-A, SP-B, and SP-C mRNAs in both alveolar and bronchiolar epithelial cells from diabetic lungs in comparison to control lungs (Sugahara et al. 1994). Nonetheless, Fernández-Real et al. (2008) reported circulating SP-A significantly higher among patients with glucose intolerance and type 2 diabetes than in subjects with normal glucose tolerance, even after adjustment for BMI, age, and smoking status. In amniotic fluid from diabetic women, SP-A levels were significantly less than in nondiabetic pregnancies. Hypertension did not modify SP-A in diabetic women. Although Snyder et al. (1988) suggested that the concentration of amniotic fluid SP-A is decreased in diabetic pregnancies, McMahan et al. (1987) concluded that in well controlled diabetic pregnancies fetal lung maturation is not adversely affected. SP-A and SP-B were significantly elevated in amniotic fluid from black mothers and in amniotic fluid from mothers who smoked during pregnancy (Pryhuber et al. 1991).
8 Expression of SPs in Lung Cancer
8.1 Non-Small-Cell Lung Carcinoma (NSCLC)
Molecular mechanisms underlying carcinogenesis of non-small cell lung cancer(NSCLC) may provide gene targets in critical pathways valuable for improving the efficacy of therapy and survival of patients with NSCLC (Chong et al. 2006). SP-A is described for a portion of NSCLC facilitating a diagnostic marker for these carcinomas (Goldmann et al. 2009). Studies in human lung carcinoma reported positive staining of tumor cells for SP-A, especially in peripheral airway cell carcinoma, which include bronchioloalveolar carcinoma and in some reports also papillary subtypes. The SP-A gene is expressed at higher levels in hyperplastic cells; the expression occurs predominantly, but not exclusively, in adenocarcinomas (Broers et al. 1992; Linnoila et al. 1992). The determination of SP-A in malignant effusions may help in distinguishing primary lung adenocarcinoma from adenocarcinomas of miscellaneous origin. Analysis of SP-A gene transcript in pleural effusion is useful for diagnosis of primary lung adenocarcinoma (Saitoh et al. 1997; Shijubo et al. 1992). Gene expression of SP-A and SP-C was restricted to metastatic pulmonary adenocarcinomas (Betz et al. 1995). Camilo et al. (2006) suggested that all adenocarcinomas were negative for p63 where as 4 (26.6%) of 15 were positive for SP-A.
Uzaslan et al. (2005) studied 169 primary adenocarcinomas of lung (109 acinar, 32 solid with mucin, 24 papillary and 4 mucinous) for SP-A expression. Twenty-five percent of acinar, 38% of papillary and 3% of solid adenocarcinoma with mucin showed a positive intracytoplasmic SP-A reaction of the tumor cells. Results support the theory that SP-A-producing cells may generate not only bronchioloalveolar and papillary carcinoma, but also other subtypes of lung adenocarcinoma (Stoffers et al. 2004; Uzaslan et al. 2005). Tsutsumida et al. (2007) advocate that high MUC1 expression on the surface is an important characteristic of a micropapillary pattern, where as reduced surfactant apoprotein A expression in the micropapillary pattern may be an excellent indicator for poor prognosis in small-size lung adenocarcinoma.
8.1.1 Genetic Factors as Lung Cancer Risk
Deletions of the SP-A gene are specific genomic aberrations in bronchial epithelial cells adjacent to and within NSCLC, and are associated with tumor progression and a history of smoking. SP-A deletions might be a useful biomarker to identify poor prognoses in patients with NSCLC who might therefore benefit from adjuvant treatment (Jiang et al. 2005). Seifart et al. (2005) genotyped for SP-A1, -A2, -B, and -D marker alleles in lung cancer subgroups, which included 99 patients with small cell lung carcinoma (SCLC), or non-SCLC (NSCLC, n = 68) consisting of squamous cell carcinoma (SCC), and adenocarcinoma (AC); controls and healthy individuals (population control). Seifart et al. (2005) found (a) no significant marker associations with SCLC, (b) rare SP-A2 (1A9) and SP-A1 (6A11) alleles associate with NSCLC risk when compared with population control, (c) the same alleles (1A9, 6A11) associate with risk for AC when compared with population (6A11) or clinical control (1A9), and (d) the SP-A1-6A4 allele (found in ~10% of the population) associates with SCC, when compared with control. A correlation between SP-A variants and lung cancer susceptibility appears to exist, indicating that SP-A alleles may be useful markers of lung cancer risk.
The SP mRNAs with SP-A, B, and C were coexpressed in 10/12 (83%) of adenomas and 4/5 (80%) of carcinomas in both solid and tubulopapillary areas. SP-D mRNA signals were not noted in normal or neoplastic lung. ISH for SP A, B, or C mRNA was a helpful aid in the diagnosis of proliferative lesions of the murine lung (Pilling et al. 1999). In ovine pulmonary adenocarcinoma, caused by jaagsiekte sheep retrovirus, SP-A and C were expressed in 70% and 80% of tumor cells, respectively, whereas Clara cell 10-kDa protein was expressed in 17% of tumor cells (Platt et al. 2002).
8.1.2 TTF-1 and SP-A in Differential Diagnosis
Results suggest that TTF-1 can play an important role for the maintenance and/or differentiation process in bronchiolar and alveolar cells (Nakamura et al. 2002). TTF-1 is frequently expressed in human lung cancer, especially in adenocarcinoma and small cell lung cancer, and TTF-1 expression is closely related to the expression of surfactant protein. Zamecnik and Kodet (2002) described positive results for TTF-1 and SP-A in 75% and 46% of pulmonary adenocarcinomas and in 50% and 25% of pulmonary non-neuroendocrine large cell carcinomas (LCCs), respectively. Small cell lung carcinomas were TTF-1 positive in 89% of cases and completely negative for SP-A. Squamous cell carcinomas and carcinoid tumors were negative for both proteins. The frequency of TTF-1 expression in the nucleus was very low in human lung cancer cell lines; however, their cytoplasmic positivities should be further investigated (Fujita et al. 2003. Rossi et al. (2003) (1) support the metaplastic histogenetic theory for pulmonary carcinomas group of tumors; (2) show that cytokeratin 7 and TTF-1, but not SP-A, are useful immunohistochemical markers in this setting, and (3) suggest that this group of tumors has a worse prognosis than conventional NSCL carcinoma at surgically curable stages I, justifying their segregation as an independent histologic type. Lu et al. (2006) suggested that nuclear inclusions positive for SP-A antibody staining in adenocarcinomas of lung were derived from accumulated content in the perinuclear cistern resembling pseudoinclusion processes and composed of proteins antigenically cross-reactive with SP-A. Because of its diagnostic utility TTF-1 should be added to a panel of antibodies used for assessing tumors of unknown origin. The combination of anti-TTF-1 with anti-SP-A does not increase the diagnostic usefulness of TTF-1 alone (Lu et al. 2006). Suzuki et al. (2005) and Ueno et al. (2003) reported that Napsin is better marker than SP-A for diagnosis of lung adenocarcinoma. Napsin A is an aspartic proteinase expressed in lung and kidney. Napsin A is expressed in type II pneumocytes and in adenocarcinomas of lung.
8.1.3 SPs as a Tool for Diagnosis of Lung Tumors
Most bronchioloalveolar carcinomas of lung react positively for SP-A. Positive SP-A staining of large cell carcinoma of the lung could indicate that at least part of these tumors have the same cellular origin or differentiation as bronchioloalveolar carcinoma. Twenty of 63 (32%) tumors stained positive for SP-A. This may imply that about one third of large cell carcinomas of lung have a similar cellular origin or differentiation as bronchioloalveolar carcinoma (Uzaslan et al. 2006).
SP-A, a marker for lung adenocarcinomas, can be used to differentiate lung adenocarcinomas from other types and metastatic cancers of other origins (Kuroki et al. 1998; Takahashi et al. 2006b). RT-PCR and primers specific for SP-A, SP-B, SP-C and SP-D genes were used to detect nodal metastases and occult tumor spread of pulmonary adenocarcinomas. A combination of SP-A and SP-D may help to establish a differential prognosis in patients with gefitinib-induced ILD (Kitajima et al. 2006). ILD is a serious adverse event in lung cancer patients treated with gefitinib, an epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI). Pretreatment with gefitinib exacerbated LPS-induced lung EGFR-TKI by reducing SP-A expression in lung. EGFR- TKI may reduce SP-A expression in lungs of lung cancer patients and thus patients treated with EGFR tyrosine kinase inhibitor may be susceptible to pathogens (Inoue et al. 2008).
SP mRNAs were present in all lung tumors, with SPs A, B, and C being co-expressed in 83% of adenomas and 80% of carcinomas in both solid and tubulopapillary areas. No signals for SP D mRNA were noted in normal or neoplastic lung. Additionally, no staining for any SP transcript was observed in the hepatocellular carcinoma metastases. In situ hybridization for SP A, B, or C mRNA was helpful in diagnosis of proliferative lesions of the murine lung, enabling differentiation from hepatocellular metastases (Pilling et al. 1999; Qi et al. 2002).
9 Other Inflammatory Disorders
9.1 Airway Inflammation in Children with Tracheostomy
The long-term tracheostomy in infants and children may perpetuate chronic airway inflammation and airway remodeling due to easier access to the lungs for microorganisms. The SP-A and SP-D may directly interact with invading microorganisms and also modulate the activity of local immune cells. Children with tracheostomy had an increased total number of cells, increased neutrophils, and more frequently bacteria, but no viruses were recovered. SP-D concentration was reduced to half, though SP-A, SP-B, and SP-C were not different from controls. SP-D was inversely correlated to neutrophils, and high numbers of bacteria were associated with lower SP-D concentrations. It was suggested that bacteria and low SP-D support neutrophilic inflammation in the lower respiratory tract of nonsymptomatic with children with tracheostomy (Griese et al. 2004). BAL fluids from patients carrying a chronic tracheostoma agglutinated P. aeruginosa, which was completely inhibited by maltose. The agglutination of P. aeruginosa by BAL fluid was related in part to the concentration of SP-D. Additional factors, such as the multimeric organization of SP-D, are likely to contribute to the agglutination of microorganisms by BAL or other body fluids (Griese and Starosta 2005).
Pulmonary Alveolar Microlithiasis (PAM): Pulmonary alveolar microlithiasis (PAM) is an uncommon chronic disease characterized by calcifications within the alveoli and a paucity of symptoms in contrast to image findings. PAM occurs in the absence of any known disorder of calcium metabolism. Takahashi et al. (2006a) reported two cases of PAM, with markedly elevated sera concentrations of SP-A and SP-D, which showed a tendency to increase as the disease progressed. Therefore, SP-A and SP-D may function as serum markers to monitor the disease activity and progression of PAM.
Gastroesophageal Reflux Disease: Children with gastroesophageal reflux often suffer from chronic, severe lung damage and recurrent infections. The mechanisms may involve reflux induced lung injury with alterations of the SP-A and SP-D, which bind specifically to various microbes and increase their elimination by granular leukocytes and macrophages. In children with gastroesophageal reflux disease (GERD), the macromolecular organization of SP-A and SP-D were significantly reduced. The more active SP-A and especially those of SP-D were diminished, whereas the smaller sized forms of SP-D were markedly increased. Reduced amounts of SP-A and SP-D and an altered structural organization of the surfactant proteins may contribute to pathogenesis of chronic lung disease commonly observed in these children (Griese et al. 2002).
9.2 Surfactant Proteins in Non-ILD Pulmonary Conditions
Infants with increased pulmonary blood flow secondary to congenital heart disease suffer from tachypnea, dyspnea, and recurrent pulmonary infections. In congenital heart disease with pulmonary hypertension secondary to increased pulmonary blood flow, there is a decrease in SP-A gene expression as well as a decrease in SP-A and SP-B protein contents (Gutierrez et al. 2001). In an experiment involving 4-week-old lambs with pulmonary hypertension secondary to increased pulmonary blood flow following an in utero placement of an aortopulmonary vascular graft, Lee et al. (2004) found a decrease in SP-A gene expression as well as a decrease in SP-A and SP-B protein contents. But in a lamb model of congenital heart disease with pulmonary hypertension and increased pulmonary blood flow, the effect of the shunt on SP gene expression and protein content was not apparent within first week of life (Lee et al. 2004). No significant association between the common genetic variants of SP-A and SP-D and victims of sudden infant death syndrome (SIDS) was disclosed by Stray-Pedersen et al. (2009). However, low SP-A protein expression may possibly be determined by the 6A2/1A0 SP-A haplotype, which should be a subject for further investigation.
The SP-A level decreases significantly in acute pulmonary embolism, which may play an important role in hypoxemia in pulmonary embolism (Xie et al. 2005). Although an immunohistochemical investigation of pulmonary SP-A suggested a characteristic increase in fatal asphyxiation, no particular change was observed in the total amount of SP-A mRNA. The analysis of the SP-A1/A2 ratio may assist interpretation of the molecular alterations of SP-A related to acute asphyxial death (Ishida et al. 2002).
In hyperpnea there is a significant increase in lamellar bodies (LB) SP-A, lysozyme, and phospholipid (PL) but no change in the protein-to-prolonged hyperpnea ratios. It was suggested that (1) surfactant-associated lysozyme is secreted with LB, (2) the majority of SP-A is linked to lipid secretion but not necessarily with LB, and (3) the majority of SP-B secretion is independent of PL secretion. (4) Hyperpnea did not alter the mRNA expression of SP-A, SP-B, SP-C, or lysozyme in alveolar type II cells, but expression of SP-A and SP-B mRNA was significantly increased in lung tissue (Yogalingam et al. 1996).
10 DNA Polymorphisms in SPs and Pulmonary Diseases
Though the genes underlying susceptibility to RDS are insufficiently known, genes coding for SP-A and B have been assigned as the most likely genes in the etiology of RDS. Acute-RDS (ARDS) develops in association with many serious medical disorders. Mortality is at least 40%, and there is no specific therapy. The deficiency in SP-A level has been implicated in the pathophysiology of ARDS. Associations between single nucleotide polymorphisms (SNPs) of human gene coding SFTPA1, SFTPA2, and SFTPD and infectious pulmonary diseases have been established by several groups.
10.1 Association Between SP-A Gene Polymorphisms and RDS
Evidences suggest that the etiology of RDS is multifactorial with a significant genetic component. There are reports about polymorphisms and mutations on the surfactant protein genes, especially surfactant proteins-B, that may be associated with RDS, ARDS, and congenital alveolar proteinosis. The human SP-A gene locus includes two functional genes, SFTPA1 and SFTPA2 which are expressed independently, and a pseudo gene. SP-A polymorphisms play a role in respiratory distress syndrome, allergic bronchopulmonary aspergillosis and idiopathic pulmonary fibrosis. The levels of SP-A are decreased in lungs of patients with CF, RDS and chronic lung diseases (Heinrich et al. 2006).
Both low levels of SP-A and SP-A alleles have been associated with RDS. Floros et al. characterized four allelic variants of SP-A1 gene (6A, 6A2, 6A3, and 6A4) and five allelic variants of the SP-A2 gene (1A, 1A0, 1A1, 1A2, and 1A3) and hypothesized that specific SP-A alleles/genotypes are associated with increased risk of RDS. Because race, gestational age (GA), and sex are risk factors for RDS, Kala et al. (1998) studied the distribution and frequencies of SP-A alleles/genotypes while adjusting for these factors as confounders or effect modifiers in control and RDS populations with GAs ranging from 24 week to term. Although the odds ratios of several alleles and genotypes were in opposite directions for black and white subjects, the homogeneity of odds ratio reached statistical significance only in case of 6A3/6A3. Although differences were observed in subgroups with different GAs of RDS white population, definitive conclusions could not be made regarding the effect of modification by GA or as a function of sex. Study suggested that (1) the genetic analyses of RDS and SP-A locus should be performed separately for black and white populations and (2) SP-A alleles/genotypes and SP-B variant may contribute to the etiology of RDS and/or may serve as markers for disease subgroups. In a genetically homogeneous Finnish population, Rämet et al. (2000) showed that certain SP-A1 alleles (6A2 and 6A3) and an SP-A1/SP-A2 haplotype (6A2/1A0) were associated with RDS. The 6A2 allele was over-represented and the 6A3 allele was under-represented in infants with RDS. According to results, diseases associated with premature birth did not explain the association between the odds of a particular homozygous SP-A1 genotype (6A2/6A2 and 6A3/6A3) and RDS. In the population evaluated, SP-B intron 4 variant frequencies were low and had no association with RDS. Thus, SP-A gene locus is an important determinant for predisposition to RDS in premature infants.
Floros et al. (2001b), in family-based linkage studies to discern linkage of SP-A to RDS, showed a link between SP-A and RDS; certain SP-A alleles/haplotypes are susceptibil (1A0, 6A2, 1A0/6A2) or protective (1A5, 6A4, 1A5/6A4) for RDS. Some differences between blacks and whites with regard to SP-A alleles may exist. In a 107 father-mother-offspring trios, divided into two sets according to proband’s phenotype, Haataja et al. (2001) evaluated familial segregation of candidate gene polymorphisms by the transmission disequilibrium test. A set of 76 trios were analyzed for transmission disequilibrium from parents to affected offspring. Another set of 31 trios were studied for allele transmission from parents to hypernormal offspring born very prematurely before GA of 32 weeks. SP-A1-A2 haplotype 6A2-1A0 showed significant excess transmission to affected infants and SP-A1 allele 6A2 decreased transmission to the hypernormals. Study provides a support for a role of SP-A alleles as genetic predisposers to RDS in premature infants.
10.2 SP-A and SP-B as Interactive Genetic Determinants of Neonatal RDS
Haataja et al. (2000) investigated if SP-B gene or interaction between SP-A and SP-B genes has a role in genetic susceptibility to RDS. Of the two SP-B polymorphisms genotyped, the Ile131Thr variation, a putative N-terminal N:-linked glycosylation site of proSP-B and length variation of intron 4 have been suggested to associate with RDS. Neither of the two SP-B polymorphisms associated directly with RDS or with prematurity. Instead, results showed that known association between SP-A alleles and RDS was dependent on the SP-B Ile131Thr genotype. Hence, the SP-B Ile131Thr polymorphism is a determinant for certain SP-A alleles as factors causing genetic susceptibility to RDS (6A2, 1A0) or protection against it (6A3, 1A2).
Floros et al. (2001a) studied genotypes for SP-B intron 4 size variants and for four SNPs [−18 (A/C), 1013 (A/C), 1580 (C/T), 9306 (A/G)] in SP-B in black and white subjects. Based on odds ratio: (1) the SP-B intron 4 deletion variant in white subjects is more of an RDS risk factor for males and for subjects of 28 weeks < gestational age (GA) <33 weeks; (2) the SP-B intron 4 insertion variant in black subjects is more of an RDS risk factor in females; (3) in white subjects, SP-A1 (6A2/6A2) or SP-A2 (1A0/1A0 or 1A0/*) genotypes in subjects of certain GA and with a specific SP-B genotype (9306 (A/G) or deletion/*) are associated with an enhanced risk for RDS; (4) in black subjects, SP-A1 (6A3/6A3 or 6A3/*) genotypes in subjects of 31 weeks < or = GA < or = 35 weeks and with the SP-B (1580 (T/T)) genotype are associated with a reduced risk for RDS. The SP-B polymorphisms are important determinants for RDS. These may identify differences between black and white subjects, as well as, between males and females regarding the risk for RDS. Moreover, SP-A susceptibility or protective alleles, in specific SP-B background, are associated with an increased or reduced risk for RDS.
10.3 RDS in Premature Infants
DNA samples from 441 premature singleton infants and 480 twin or multiple infants were genotyped for SP-A1, SP-A2, and SP-B exon 4 polymorphisms and intron 4 size variants in a homogeneous white population. Distribution of SP-A and SP-B gene variants between RDS and no-RDS infants were determined alone and in combination. The SP-A1 allele 6A2 and homozygous genotype 6A2/6A2 are over-represented in RDS of singletons when SP-B exon 4 genotype was Thr/Thr, and under represented in RDS of multiples when the SP-B genotype was Ile/Thr. The SP-A 6A2 allele in SP-B Thr131 background predisposed the smallest singleton infants to RDS, whereas near-term multiples were protected from RDS. There was a continuous association between fetal mass and risk of RDS, defined by SP-A and SP-B variants. Labeled lung explants with the Thr/Thr genotype showed proSP-B amino-terminal glycosylation, which was absent in Ile/Ile samples. Hence, Genetic and environmental variation may influence intracellular processing of surfactant complex and the susceptibility to RDS (Marttila et al. 2003b). However, the association between SP-A polymorphisms and RDS may not be applicable to entire population of premature infants. In twins, the association between SP-A polymorphism and RDS is different from that seen in premature singleton infants. The factor associated with SP-A genotype-specific susceptibility to RDS appears to be related to the size of uterus and length of gestation at birth (Marttila et al. 2003a). Zhai et al. (2008) reported that the frequency of SP-A1 allele 6A2 and 6A3 expression of SP-A in Chinese premature infants was low in neonatal RDS. In contrast, the frequency of SP-A2 allele 1A0 and 1A1 was high in normal Chinese premature infants. It supports that SP-A1 allele 6A2 may be a susceptible gene for RDS.
10.4 Gene Polymorphism in Patients of High-altitude Pulmonary Edema
A pathogenetic cofactor for development of high-altitude pulmonary edema (HAPE) is an increase in capillary permeability, which could occur as a result of an inflammatory reaction and/or free-radical-mediated injury to lung. Pulmonary SP-A has potent antioxidant properties and protects unsaturated phospholipids and growing cells from oxidative injury (Swenson et al. 2002). In view of protective role of SP-A against oxidative damage, Saxena et al. (2005) examined the association of constitutional susceptibility to HAPE with polymorphisms in SP-A1 and SP-A2. Allele frequencies of three loci in SP-A1 and one in SP-A2 were significantly different between low-altitude native (LAN) HAPE patients and LAN control subjects. Heterozygous individuals, with respect to SP-A1 C1101T and SP-A2 A3265C, showed less severity in oxidative damage in comparison with homozygous subjects (SP-A1 T1101 and SP-A2 C3265). The polymorphisms in SP-A1 might be one of the genetic factors contributing to susceptibility to HAPE (Saxena et al. 2005).
10.5 SNPs in Pulmonary Diseases
Four validated SNPs were genotyped with sequence-specific probes (TaqMan 7000) in 284 newborn infants below 32 weeks of GA. The finding of an association of a variant of the Sftpd gene, that has previously been shown to be associated with increased SP-D serum levels in adult patients with RDS in preterm infants, may provide a basis for the initial risk assessment of RDS and modification of surfactant treatment strategies. A role for SP-D in neonatal pulmonary adaptation has to be postulated. Genotyping for three SNP altering amino acids in the mature protein in codon 11 (Met11Thr), 160 (Ala160Thr), and 270 (Ser270Thr) of the SP-D gene was performed and related to the SP-D levels in serum. Individuals with Thr/Thr-11-encoding genotype had significantly lower SP-D serum levels than individuals with Met/Met (11) genotype. Polymorphic variation in the N-terminal domain of the SP-D molecule influences oligomerization, function, and the concentration of the molecule in serum (Hilgendorff et al. 2009; Leth-Larsen et al. 2005; Sorensen et al. 2007).
Studies on twins indicated very strong genetic dependence for serum levels of SP-D. Sequencing of 5′ untranslated region (5′UTR), the coding region and the 3′ region of Sftpd gene of 32 randomly selected blood donors indicated one single Sftpd haplotype (allele frequency 13.53%) that showed a negative association with serum SP-D levels. The discovery of a frequent negative variant of Sftpd gene provides a basis for genetic analysis of function of SP-D in resistance against pulmonary infections and inflammatory disorders in humans (Heidinger et al. 2005). The presence of SP-D in non-pulmonary tissues, such as gastrointestinal tract and genital organs, suggest additional functions located to other mucosal surfaces. Sorensen et al. (2007) summarized studies on genetic polymorphisms, structural variants, and serum levels of human SP-A and SP-D and their associations with human pulmonary disease.
Polymorphisms of genes are transmitted together in haplotypes, which can be used in study of development of complex diseases such as RDS. Genetic haplotypes of these SP genes are associated with the development of RDS. Studies identify protective haplotypes against RDS and support findings related to SP genetic differences in children who develop RDS. An allele association study of 19 polymorphisms in SP-A1, SP-A2, SP-B, and SP-D genes in ARDS was carried out. Analysis revealed differences in frequency of alleles for some of the microsatellite markers flanking SP-B, and for one polymorphism (C/T) at nucleotide 1580 [C/T (1580)], within codon 131 (Thr131Ile) of the SP-B gene. The latter determines the presence or absence of a potential N-linked glycosylation site. Based on the odds ratio, the C allele may be viewed as a susceptibility factor for ARDS. These data suggest that SP-B or a linked gene contributes to susceptibility to ARDS (Lin et al. 2000; Thomas et al. 2007).
Amino Acid Variants in SP-D Are Not Associated with Bronchial Asthma: As SP-D binds and neutralizes common allergens like house dust mites it is especially important in allergic asthma. Levels of SP-D are elevated in serum and alveolar lavage of asthmatic patients. Three common amino acid variants have been identified in SP-D and association of first variant has been described to severe infection with respiratory syncytial virus. The three polymorphisms leading to amino acid exchanges (Met11Thr, Ala160Thr, and Ser270Thr) were typed in 322 asthmatic children and none of these polymorphisms was associated with bronchial asthma. Haplotype analyses revealed four major haplotypes all of which were evenly distributed between the populations. Functional amino acid variants in SP-D do not seem to play a major role in the genetic pre-disposition to bronchial asthma in children (Krueger et al. 2006).
Following allergen exposure in vivo, SP-D−/− mice expressed higher bronchoalveolar lavage (BAL) eosinophils and IL-13 and lower FN-γ expression at early time points compared with wild mice. IL-10 expression was increased at early time points in SP-D−/− compared with wild mice. SP-D may be critical for the modulation of early stages of allergic inflammation in vivo (Schaub et al. 2004).
Pettigrew et al. (2006, 2007) evaluated gene polymorphisms in loci encoding SP-A and risk of otitis media during first year of life among a cohort of infants at risk for developing asthma in white infants. Polymorphisms at codons 19, 62, and 133 in SP-A1, and 223 in SP-A2 were associated with race/ethnicity. In regression models incorporating estimates of uncertainty in haplotype assignment, the 6A4/1A5 haplotype was protective for otitis media among white infants. On similar line, analyses suggested that polymorphisms within SFTPA loci may be associated with wheeze and persistent cough in white infants at risk for asthma. These associations require replication and exploration in other ethnic/racial groups.
10.6 Allergic Bronchopulmonary Aspergillosis and Chronic Cavitary Pulmonary Aspergillosis (CCPA)
Individuals with any structural or functional defects in SP-A and SP-D due to genetic variations might be susceptible to aspergillosis. Single nucleotide polymorphism in genes of collagen region of SP-A1 and SP-A2 has been associated with allergic bronchopulmonary aspergillosis (ABPA) and its clinical markers. SP-A2 G1649C and SP-A2 A1660G, polymorphisms in the collagen region of SP-A2, might be one of the contributing factors to genetic predisposition and severity of clinical markers of ABPA. SNPs in SP-A2 and MBL genes showed significant associations with patients of ABPA in an Indian population. Patients carrying either one or both of GCT and AGG alleles of SP-A2 and patients with A allele at position 1011 of MBL had markedly higher eosinophilia, total IgE antibodies and lower FEV1. Therapeutic administration of SP-D and MBL proteins in a murine model of pulmonary invasive aspergillosis rescued mice from death. In mice mimicking human ABPA, SP-A and SP-D suppressed IgE levels, eosinophilia, pulmonary cellular infiltration and cause a marked shift from a pathogenic Th2 to a protective Th1 cytokine profile. Thus, collectins play an important role in Aspergillus mediated allergies and infections (Madan et al. 2005; Saxena et al. 2003).
Patients with CCPA or ABPA of Caucasian origin were screened for SNPs in collagen region of SP-A1 and SP-A2 and MBL. The T allele at T1492C and G allele at G1649C of SP-A2 were observed at slightly higher frequencies in ABPA patients (86% and 93%) than in controls (63% and 83%), and the C alleles at position 1492 and 1649 were found in higher frequencies in CCPA patients (33% and 25%) than in ABPA patients (14% and 7%). However, the CC genotype at position 1649 of SP-A2 was significantly associated with CCPA. Similarly, ABPA patients showed a higher frequency of TT genotype (71%) at 1492 of SP-A2 than controls (43%) and CCPA patients (41%). In case of MBL, the T allele and CT genotype at position 868 (codon 52) were significantly associated with CCPA, but not with ABPA. Further analysis of genotype combinations at position 1649 of SP-A2 and at 868 of MBL between patient groups showed that both CC/CC and CC/CT SP-A2/MBL were found only in CCPA patients, while GG/CT SP-A2/MBL was significantly higher in CCPA patients in comparison to ABPA patients. SNPs in SP-A1 did not differ between patients and controls. Distinct alleles, genotypes and genotype combinations of SP-A2 and MBL may contribute to differential susceptibility of the host to CCPA or ABPA (Vaid et al. 2007).
Allergic Airway Inflammation: The SP-A has potent immunomodulatory activities. SP-A protein levels in the BAL fluid showed a rapid, transient decline that reached the lowest values (25% of controls) 12 h after intranasal Af provocation of sensitized mice. It was speculated that a transient lack of SP-A following allergen exposure of airways may significantly contribute to the development of a T-cell dependent allergic immune response (Scanlon et al. 2005). After acute ovalbumin-induced allergic airway inflammation (1) alveolar epithelial type II cells (AEII) but not Clara cells show a significantly higher expression of SP-A and SP-D in rats leading also to higher amounts of both SPs in BALF and (2) macrophages gather predominantly SP-A (Schmiedl et al. 2008).
10.7 Autoreactivity Against SP-A and Rheumatoid Arthritis
Circulating SP-D is decreased in early rheumatoid arthritis and SP-A and SP-D levels in synovial fluid from patients correlated with rheumatoid factor, CRP, IgA, IgM, and IgG, and total lipid content. SP-A and SP-D seem to participate in initiation of immune system and joint inflammation within the joint (Kankavi 2006) and may be an additional RA disease modifier like MBL. The Met11Thr polymorphism in the N-terminal part of SP-D is important determinant in serum SP-D. But this polymorphism is also essential to the function and assembly into oligomers. SP-D levels did not correlate with traditional disease activity measures. The Thr11/Thr11 genotype and the Thr11 allele tended to be more frequent in RA patients. Therefore, the low serum level of SP-D and the lack of correlation with traditional disease activity measures indicate that SP-D reflects a distinctive aspect in the RA pathogenesis (Hoegh et al. 2008; Miyata et al. 2002). Trinder et al. (2000) were able to show autoreactivity to SP-A, as expressed by IgG and IgM autoantibodies, and present in synovial fluid (SF) from patients with RA. There was no cross-reactivity between autoantibodies reactive with type II collagen (CII) and those reactive with SP-A or C1q; However, autoantibodies reacted with polymeric (dimers and larger) SP-A, but not with monomeric SP-A subunits, indicating that a degree of quaternary structure is required for antibody binding.
11 Inhibition of SP-A Function by Oxidation Intermediates of Nitrite
11.1 Protein Oxidation by Chronic Pulmonary Diseases
The oxidation of proteins may play an important role in the pathogenesis of chronic inflammatory lung diseases, and may contribute to lung damage. Higher levels of protein oxidation than in healthy controls were observed in patients with interstitial lung disease, gastro-esophageal reflux disease, and PAP. The proteins most sensitive to oxidation were serum albumin, SP-A, and α1-antitrypsin. Abundance of reactive oxygen species produced during neutrophilic inflammation may be a deleterious factor that leads to pulmonary damage in these patients (Starosta and Griese 2006). Primary chain and quaternary structure of SP-D in BALFs showed significant changes under oxidative conditions in vitro and in vivo and functional capacity to agglutinate bacteria was impaired by oxidation. Free radicals generated in lungs resulting in oxidation of SP-D may impair host defense and may contribute to the suppurative lung diseases like cystic fibrosis (Starosta and Griese 2006).
11.2 Oxidation Intermediates of Nitrite
Nitration of protein tyrosine residues by peroxynitrite (ONOO−) has been implicated in a variety of inflammatory diseases such as ARDS. A mixture of hypochlorous acid (HOCl) and nitrite (NO −2 ) induces nitration, oxidation, and chlorination of tyrosine residues in human SP-A, and inhibits SP-A’s ability to aggregate lipids and bind mannose. Nitration and oxidation of SP-A was not altered by the presence of lipids, suggesting that proteins are preferred targets in lipid-rich mixtures such as pulmonary surfactant. Moreover, both horseradish peroxidase and myeloperoxidase (MPO) can utilize NO −2 and H2O2 as substrates to catalyze tyrosine nitration in SP-A, and inhibit its lipid aggregation function. SP-A nitration and oxidation by MPO is markedly enhanced in presence of Cl− and the lipid aggregation function of SP-A is completely abolished. Studies suggest that MPO released by activated neutrophils during inflammation utilizes physiological or pathological levels of NO −2 to nitrate proteins, and may provide an additional mechanism in addition to ONOO – formation, for tissue injury in ARDS and other inflammatory diseases associated with upregulated NO* and oxidant production. The oxidant-mediated tissue injury is likely to be important in the pathogenesis of ARDS/ALI (Davis et al. 2002; Lang et al. 2002; Narasaraju et al. 2003).
In vitro and in vivo data suggest that NO alters surfactant protein gene expression. The role of NO in ALI remains controversial. Although inhaled NO increases oxygenation in clinical trials, inhibiting NOS can be protective. However, inhalation of NO may not be indicated in sepsis because of excessive NO production. Aikio et al. (2003) indicated that inhaled NO is effective in a select group of small premature infants and that the responsiveness to NO is associated with low NOS2 enzyme. Very low birth-weight infants (birthweight <1,500 g), infants with progressive respiratory failure and infection at birth have deficient pulmonary NOS2 and cytokine response. After surfactant therapy, these infants responded strikingly to inhaled NO. An acute pulmonary inflammatory response may contribute to respiratory adaptation in early-onset pneumonia. In intact lambs inhaled NO increased SP-A and SP-B mRNA and protein content with no change in DNA content. The mechanisms and physiological effects of these findings warrant further investigation (Stuart et al. 2003; Hu et al. 2007). Exposure of rats to NO2 showed impairment of SP-A and a higher alveolar pool size after in vivo exposure. The NO2-induced alterations of SP-A may contribute to the pulmonary toxicity of this oxidant (Müller et al. 1992). NO production from NOS2 expressed in lung parenchymal cells in a murine model of ARDS correlates with abnormal surfactant function and reduced SP-B expression. NOS2−/− null mice exhibit significantly less physiologic lung dysfunction and loss of SP-B expression. Study indicated that the expression of NOS2 in lung epithelial cells is critical for the development of lung injury and mediates surfactant dysfunction independent of NOS2 inflammatory cell expression and cytokine production (Baron et al. 2004).
11.3 BPD Treatment with Inhaled NO
Inhaled NO is used to treat a number of disease processes. BPD is characterized by arrested alveolar and vascular development of immature lung. The increased expression of SP-A mRNA under hyperoxia can be attributed, at least in part, to an induction of mRNA and protein expression in bronchial Clara cells. The expanded role of Clara cells in the defence against hyperoxic injury suggests that they support alveolar type 2 cell function and may play an important role in the supply of surfactant proteins to the lower airways (ter Horst et al. 2006). The inhaled nitric oxide treatment of premature infants at risk for bronchopulmonary dysplasia does not adversely affect endogenous surfactant function or composition and may improve surfactant function transiently (Ballard et al. 2007). Chorioamnionitis is a risk factor for the development of bronchopulmonary dysplasia. Endotoxin-induced oxidative stress to the fetus in the uniquely hypoxic intrauterine environment has been reported. SP-A and B mRNAs were highest at Day 2, suggesting that oxidative stress did not contribute to the lung maturation response. A modest lung oxidative stress in chorioamnionitis could contribute to bronchopulmonary dysplasia (Cheah et al. 2008).
12 Congenital Diaphragmatic Hernia
Pulmonary hypoplasia is one of the main causes for high mortality rate in patients with congenital diaphragmatic hernia (CDH). The expression of SP-A in hypoplastic CDH lung is reduced, and its concentration is decreased in amniotic fluid of pregnancies complicated by CDH. In animal models, surfactant deficiency contributes to the pathophysiology of the disease. In humans surfactant disaturated phosphatidylcholine (DSPC) synthesis and SP-A were significantly lower in infants with CDH than in control subjects (Cogo et al. 2002).
SP-A is altered in developing lungs from rat fetuses with CDH induced by maternal ingestion of Nitrofen on Day 9 of gestation. There is decreased expression of SP-A in rat fetuses with CDH secondary to Nitrofen exposure (Mysore et al. 1998). In rat CDH model, induced in pregnant rats following administration of nitrofen, SP-A, SP-B, and SP-D mRNA expression in CDH lung were significantly decreased compared to controls at birth and 6 h after ventilation. The inability of O2 to increase SP mRNA expression in hypoplastic CDH lung suggests that the hypoplastic lung is not responsive to increased oxygenation for synthesis of SP (Shima et al. 2000). Though, SP’s deficiency appears to be a common feature among various CDH models, TTF-1 expression was not altered in surgical model in contrast to nitrofen model, indicating different molecular mechanisms in two models (Benachi et al. 2002).
13 Protective Effects of SP-A and SP-D on Transplants
Surfactant treatment has been shown to improve lung transplant function, but the effect is variable. Erasmus et al. (2002) indicated that SP-A enrichment of surfactant improves the efficacy of surfactant in lung transplantation. After instillation of SP-A-enriched surfactant, PO2 values were reached to control values, whereas after SP-A-deficient surfactant treatment, the PO2 values did not improve (Erasmus et al. 2002). The impairment of surfactant adsorption from transplanted lungs may be correlated with decreased levels of SP-A, and increased levels of serum acute-phase protein C-reactive protein (CRP). The elevated levels of CRP in BAL can be a very sensitive marker of lung injury (Casals et al. 1998).
Bronchiolitis obliterans syndrome (BOS) affects long-term survival of lung transplant recipients (LTRs). Among 11 differentially expressed proteins in BALF, peroxiredoxin 2 (Prdx2) exclusively expressed in BOS; and SP-A expressed consistently less in BOS patients than in stable LTRs. The reduction of SP-A in BALF was detectable early after lung transplant, preceding BOS onset in four of five patients and indicated that SP-A levels in BALF could predict LTR patients who are at higher risk of BOS development (Meloni et al. 2007) BOS and IPS cause high mortality and impaired survival after allogeneic hematopoietic stem-cell transplantation (allo-HSCT). The pretransplant serum SP-D levels but not SP-A, KL-6 in BOS/IPS patients were lower than those in non-BOS/IPS patients. However, the patients with lower pretransplant serum SP-D level had a trend toward frequent development of BOS/IPS. Constitutive serum SP-D level before allo-HSCT may be a useful, noninvasive predictor for the development of BOS/IPS (Nakane et al. 2008).
Keratinocyte growth factor (KGF) given before bone marrow transplantation (BMT) can prevent allogeneic T cell-dependent lung inflammation, but the antiinflammatory effects of KGF were impaired in mice injected with both T cells and conditioning regimen of cyclophosphamide. Yang et al. (2000, 2002) demonstrated that addition of cyclophosphamide interferes with the ability of KGF to enhance SP-A production. The systemic pre-BMT injection of KGF in recipients of allogeneic T cells up-regulates SP-A, which may contribute to the early antiinflammatory effects of KGF. Exogenous and basal endogenous SP-A can suppress donor T-cell-dependent inflammation that occurs during the generation of idiopathic pneumonia syndrome after BMT. Wild-type and SP-A-deficient mice, given allogeneic donor bone marrow plus inflammation-inducing spleen T cells, showed that basal endogenous SP-A, and enhanced alveolar SP-A level modulate donor T-cell-dependent immune responses and prolong survival after allogeneic BMT.
14 Therapeutic Effects of SP-A, SP-D and Their Chimeras
14.1 SP-A Effects on Inflammation of Mite-sensitized Mice
SP-A and SP-D interact with a wide range of inhaled allergens, competing for their binding to cell-sequestered IgE resulting in inhibition of mast cell degranulation. SP-D interacts with glycoprotein allergens of house dust mite (Dermatophagoides pteronyssinus, Derp) via its CRDs and thus inhibits specific IgE, isolated from mite-sensitive asthmatic patients, from binding these allergens, and blocking subsequent histamine release from sensitized basophils. Exogenous administration of SP-A and SP-D diminishes allergic hypersensitivity in vivo. A fragment of recombinant human SP-D (rfh SP-D) has a therapeutic effect on allergen-induced bronchial inflammation through its inhibitory effect on NO and TNF-α production by AΦs, and thus preventing the development of Th-2 type cytokine response (Liu et al. 2005b; Singh et al. 2003). The rfhSP-D that is effective in diminishing allergic hypersensitivity in mouse models of dust mite allergy was more susceptible to degradation than the native full-length protein. The degradation and consequent inactivation of SP-A and SP-D may be a mechanism to account for the potent allergenicity of these common dust mite allergens (Deb et al. 2007). Evidence suggests for an antiinflammatory role for SP-D in response to noninfectious, subacute lung injury via modulation of oxidative-nitrative stress (Casey et al. 2005).
14.2 SP-D Increases Apoptosis in Eosinophils of Asthmatics
The effect of exogenous rfhSP-D on protection of adult mouse lung from LPS-induced and lipoteichoic acid (LTA)-induced injury was assessed in Sftpd +/+ and Sftpd −/− mice. Intratracheal rhSP-D inhibited inflammation induced by intratracheal LPS and LTA instillation in lung. The antiinflammatory effects of rhSP-D were enhanced by addition of pulmonary surfactant, providing a potential therapy for the treatment of lung inflammation (Ikegami et al. 2007). In view of therapeutic effects of exogenous SP-D or rfhSP-D (composed of eight Gly-X-Y collagen repeat sequences, homotrimeric neck and lectin domains) in murine models of lung allergy and hypereosinophilic SP-D gene-deficient mice, Mahajan et al. (2008) suggested that rfhSP-D mediated preferential increase of apoptosis of primed eosinophils while not affecting the normal eosinophils. The increased phagocytosis of apoptotic eosinophils may be important mechanisms of rfhSP-D and SP-D-mediated resolution of allergic eosinophilic inflammation in vivo.
14.3 Targeting of Pathogens to Neutrophils Via Chimeric SP-D/Anti-CD89 Protein
Intratracheal rfhSP-D prevents shock caused by endotoxin released from the lung during ventilation in the premature newborn (Ikegami et al. 2006). In lambs, preterm infants experience enhanced susceptibility and severity to respiratory syncytial virus (RSV) infection. This was observed when SP-A, -D and TLR4 mRNA expression increased from late gestation to term birth, where as in preterm lungs, studies showed reduced SP-A, -D, and TLR4 expression and enhanced RSV susceptibility (Meyerholz et al. 2006).
A chimeric protein, consisting of a recombinant fragment of human SP-D coupled to a Fab’ fragment directed against human Fc α receptor (CD89) (chimeric rfSP-D/anti-Fc), effectively targets pathogens recognized by SP-D to human neutrophils. A recombinant trimeric fragment of SP-D (rfSP-D), consisting of CRD and neck domain of human SP-D, cross-linked to the Fab’ of an Ab directed against the human Fc α RI (CD89) (chimeric rfSP-D/anti-CD89 protein) enhanced uptake of E. coli, C. albicans, and influenza A virus by human neutrophils (Tacken et al. 2004). Both chimeric rfSP-D/anti-Fc receptor proteins increased internalization of E. coli by human promonocytic cell line U937, but only after induction of monocytic differentiation. Both CD64 and CD89 on U937 cells proved suitable for targeting by rfSP-D/anti-Fc receptor proteins (Tacken and Batenburg 2006). Collectin-based chimeric proteins may thus offer promise for therapy of infectious disease.
14.4 Anti-IAV and Opsonic Activity of Multimerized Chimeras of rSP-D
A recombinant human SP-D, consisting of a short collagen region (two repeats of Gly-Xaa-Yaa amino acid sequences), the neck domain and CRD can form a trimeric structure owing to neck domain and exhibits sugar-binding activity and specificity similar to those of native human SP-D. Though the truncated SP-D could bind to IAV, like native SP-D, but the truncated human SP-D was less effective in agglutinating bacteria than the native structure and failed to inhibit haemagglutination by IAV (Eda et al. 1997). On the other hand, chimeric collectin containing N-terminus and collagen domain of human SP-D and CRD of MBL showed greater anti-IAV activity than similarly multimerized preparations of SP-D or incompletely oligomerized preparations of the chimera. Highly multimerized preparations of chimera also caused greater increases in uptake of IAV by neutrophils. These studies may be useful for development of collectins as therapeutic agents against IAV infection (Hartshorn et al. 2000b; White et al. 2000).
Bovine serum conglutinin has greater ability to inhibit IAV infectivity than other collectins. Altering the carbohydrate binding properties of SP-D [e.g., by replacing its CRD with that of either MBL or conglutinin] can increase its activity against IAV. Hence, recombinant conglutinin and a chimeric protein containing NH2 terminus and collagen domain of rat SP-D (rSP-D) fused to neck region and CRD of conglutinin (termed SP-D/Cong(neck + CRD)) have markedly greater ability to inhibit infectivity of IAV than wild-type recombinant rSP-D, confirming that potent IAV-neutralizing activity of conglutinin resides in its neck region and CRD. Furthermore, SP-D/Cong(neck + CRD) also caused substantially greater enhancement of neutrophil binding and H2O2 responses to IAV than r-conglutinin or rSP-D. Hence, chimeric SP-D/Cong(neck + CRD) protein showed favorable antiviral and opsonic properties of conglutinin and SP-D (Hartshorn et al. 2000a). Thus, the SP-D N-terminal and/or collagen domains contribute to the enhanced bacterial binding and aggregating activities of SP-D. Although replacement of neck recognition domains and CRDs of SP-D with those of MBL and conglutinin confer increased viral binding activity, it does not favorably affect bacterial binding activity, suggesting that requirements for optimal collectin binding to influenza virus and bacteria differ (Hartshorn et al. 2007).
Chimera of Trimeric Neck + CRDs of Human SP-D: The recombinant trimeric neck + CRDs of human SP-D (NCRD) retains binding activity for some ligands and mediates some functional activities. In comparison to strong neutralizing activity of lung SP-D for IAVs in vitro and in vivo, the NCRD derived from SP-D has weak viral-binding ability and lacks neutralizing activity. Using a panel of mAbs against NCRD, Tecle et al. (2008) showed that antiviral activities of SP-D can be reproduced without the N-terminal and collagen domains and that cross-linking of NCRDs is essential for antiviral activity of SP-D with respect to IAV (Tecle et al. 2008).
Incubation of native SP-D or NCRDs with peroxynitrite results into nitration and nondisulfide cross-linking. Modifications could be blocked by peroxynitrite scavengers or pH inactivation of peroxynitrite. Abnormal cross-linking leads to defective aggregation. Thus, modification of SP-D by reactive oxygen-nitrogen species could contribute to alterations in the structure and function of SP-D at sites of inflammation in vivo (Matalon et al. 2009). In contrast, a trimeric neck and CRD construct of bovine serum collectin CL-46 induces aggregation of IAV and potently increases IAV uptake by neutrophils. CL-46-NCRD showed calcium-dependent and sugar-sensitive binding to both neutrophils and IAV. Results indicate that collectins can act as opsonins for IAV even in the absence of the collagen domain or higher order multimerization. This may involve increased affinity of individual CRDs for glycoconjugates displayed on host cells or the viral envelope (Hartshorn et al. 2010).
Insertion of Arg-Ala-Lys in NCRD Increases Inhibitory Activity: Arg-Ala-Lys (RAK) (immediately N-terminal to the first motif) in CL-43 contributes to differences in saccharide selectivity and host defense function. Insertion of CL-43 RAK sequence or a control Ala-Ala-Ala sequence (AAA) into corresponding position in NCRD increased the efficiency of binding to mannan and changed the inhibitory potencies of competing saccharides to more closely resemble those of CL-43. In addition, RAK resembled CL-43 in its greater capacity to inhibit infectivity of IAV and to increase uptake of IAV by neutrophils (Crouch et al. 2005).
15 Lessons from SP-A and SP-D Deficient Mice
SP-D deficient (SP-D−/−) mice exhibit an increase in the number and size of airway macrophages, peribronchiolar inflammation, increases in metalloproteinase activity, and development of emphysema. Mice deficient in SP-D−/− develop progressive emphysema with age, associated with loss of parenchymal tissue, subpleural fibrosis, and accumulation of abnormal elastin fibers. The changes in lung structure in SP-D−/− mice are reflected in the mechanical properties of both airway and lung parenchyma measured in vivo (Yoshida and Whitsett 2006).
Gene-targeted mice deficient in SP-D develop abnormalities in surfactant homeostasis, hyperplasia of alveolar epithelial type II cells, and emphysema-like pathology. Alveolar and tissue phosphatidylcholine pool sizes are markedly increased in SP-D−/− mice. The pulmonary lipoidosis in SP-D−/− mice was not associated with accumulation of SP-B or C, or their mRNAs, distinguishing the disorder from alveolar proteinosis syndromes. Surfactant protein A mRNA was reduced and, SP-A protein appeared to be reduced in SP-D−/− compared with wild type mice. Targeting of mouse SP-D gene caused accumulation of surfactant lipid and altered phospholipid structures, demonstrating a unsuspected role for SP-D in surfactant lipid homeostasis in vivo (Botas et al. 1998; Korfhagen et al. 1998; Ikegami et al. 2005). HDL cholesterol was significantly elevated in SP-D−/− mice while treatment of SP-D−/− mice with rhSP-D resulted in decreases of HDL-cholesterol as well as total cholesterol, and LDL cholesterol along with reduced plasma TNF-α in SP-D−/− mice. It shows that SP-D regulates atherogenesis in mouse model (Sorensen et al. 2006). SP-D plays a critical role in the suppression of alveolar macrophage activation, which may contribute to the pathogenesis of chronic inflammation and emphysema (Wert et al. 2000). Oxidant production and reactive oxygen species were increased in lungs of SP-D−/− mice, in turn activate NF-kB and MMP expression. SP-D plays an unexpected inhibitory role in the regulation of NF-kB in AΦs (Yoshida et al. 2001).
Studies indicate that GM-CSF-dependent macrophage activity is not necessary for emphysema development in SP-D-deficient mice, but that type II cell metabolism and proliferation are, either directly or indirectly, regulated by GM-CSF in this model (Hawgood et al. 2001; Ochs et al. 2004). SP-D and GM-CSF play distinct roles in the regulation of surfactant homeostasis and lung structure (Ikegami et al. 2001).
SP-A and SP-D Double Deficient Mice SP-A and SP-D proteins have overlapping as well as distinct functions. Mice singly deficient in SP-A and SP-D have distinct phenotypes and produce altered inflammatory responses to microbial challenges. Adult mice deficient in both SP-A and SP-D (A−D−) show fewer and larger alveoli, an increase in the number and size of type II cells, as well as more numerous and larger alveolar macrophages. Chronic deficiency of SP-A and SP-D in mice leads to parenchymal remodeling, type II cell hyperplasia and hypertrophy, and disturbed intracellular surfactant metabolism (Jung et al. 2005) In double deficient mice, there is a progressive increase in bronchoalveolar lavage phospholipid, protein, and macrophage content through 24 week of age. The macrophages from doubly deficient mice express high levels of the MMP-12 and develop intense but patchy lung inflammation. Qualitative changes resemble the lung pathology seen in SP-D-deficient mice (Hawgood et al. 2002).
Treatment of SP-D deficient mice with a truncated recombinant fragment of human SP-D (rfhSP-D) decreased lipidosis and alveolar macrophage accumulation as well as production of proinflammatory chemokines. The rfhSP-D treatment reduced the structural abnormalities in parenchymal architecture and type II cells characteristic of SP-D deficiency and reduced degree of emphysema and a corrected type II cell hyperplasia and hypertrophy. This suggests that rfhSP-D might become a therapeutic option in diseases that are characterized by decreased SP-D levels in the lung (Knudsen et al. 2007; Zhang et al. 2002).
Treatment with a recombinant fragment of human SP-D consisting of a short collagen-like stalk (but not the entire collagen-like domain of native SP-D), neck, and CRD inhibited development of emphysema-like pathology in SP-D deficient mice. On the other hand, the entire collagen-like domain was necessary for preventing SP-D knockout mice from pulmonary emphysema development. The fragment of SP-D lacking the short collagen-like stalk failed to correct pulmonary emphysematous alterations demonstrating the importance of the short collagen-like stalk for the biological activity of the recombinant fragment of human SP-D (Knudsen et al. 2009; Breij and Batenburg 2008).
NO Production and S-Nitrosylation of SP-D Controls Inflammatory Function SP-D−/− mice exhibit an increase in the number and size of airway macrophages, peribronchiolar inflammation, increases in metalloproteinase activity, and development of emphysema. SP-A inhibited production of NO and inducible nitric oxide synthase (iNOS) in rat AΦ stimulated with smooth LPS. In contrast, SP-A enhanced production of NO and iNOS in cells stimulated with IFN-γ or IFN-γ plus LPS. SP-A contributes to the lung inflammatory response by exerting differential effects on the responses of immune cells, depending on their state and mechanism of activation (Stamme et al. 2000). NO is involved in a variety of signaling processes, and because altered NO metabolism has been observed in inflammation, it is predicted that alterations in its metabolism would underlie the proinflammatory state observed in SP-D deficiency (Atochina et al. 2004a, c). Treatment with the iNOS inhibitor 1,400 W can inhibit inflammatory phenotype and can attenuate inflammatory processes within SP-D deficiency. Mice treated with 1,400 W reduced total lung NO synthase activity (Atochina-Vasserman et al. 2007). Guo et al. (2008) suggest that NO controls the dichotomous nature of SP-D and that posttranslational modification by S-nitrosylation causes quaternary structural alterations in SP-D causing it to switch its inflammatory signaling role. This represents new insight into both the regulation of protein function by S-nitrosylation and NO’s role in innate immunity (Guo et al. 2008). Thus, inflammation that occurs in SP-D deficiency is due to an increase in NO production and a shift in the chemistry and targets of NO from a disruption of NO-mediated signaling within the innate immune system. However, purified preparations of SPs often contain endotoxin and the functions of SP-A and SP-D are affected by endotoxin. Therefore, the monitoring of SP preparations for endotoxin contamination is important (Wright et al. 1999).
References
Aikio O, Vuopala K, Pokela ML, Hallman M (2000) Diminished inducible nitric oxide synthase expression in fulminant early-onset neonatal pneumonia. Pediatrics 105:1013–1019
Aikio O, Saarela T, Pokela ML et al (2003) Nitric oxide treatment and acute pulmonary inflammatory response in very premature infants with intractable respiratory failure shortly after birth. Acta Paediatr 92:65–69
Alexis NE, Muhlebach MS, Peden DB, Noah TL (2006) Attenuation of host defense function of lung phagocytes in young cystic fibrosis patients. J Cyst Fibros 5:17–25
Allen MJ, Harbeck R, Smith B et al (1999) Binding of rat and human surfactant proteins A and D to Aspergillus fumigatus conidia. Infect Immun 67:4563–4569
Al-Salmi QA, Walter JN, Colasurdo GN et al (2005) Serum KL-6 and surfactant proteins A and D in pediatric interstitial lung disease. Chest 127:403–407
Amin RS, Wert SE, Baughman RP et al (2001) Surfactant protein deficiency in familial interstitial lung disease. J Pediatr 139:85–92
Appelmelk BJ, Eggleton P, Reid KB et al (2005) Variations in Helicobacter pylori lipopolysaccharide to evade the innate immune component surfactant protein D. Infect Immun 73:7677–7686
Arai Y, Obinata K, Sato Y, Hisata K et al (2001) Clinical significance of the serum surfactant protein D and KL-6 levels in patients with measles complicated by interstitial pneumonia. Eur J Pediatr 160:425–429
Atochina EN, Beck JM, Preston AM et al (2004a) Enhanced lung injury and delayed clearance of Pneumocystis carinii in surfactant protein A-deficient mice: attenuation of cytokine responses and reactive oxygen-nitrogen species. Infect Immun 72:6002–6011
Atochina EN, Beers MF, Hawgood S et al (2004b) Surfactant protein-D, a mediator of innate lung immunity, alters the products of nitric oxide metabolism. Am J Respir Cell Mol Biol 30:271–279
Atochina EN, Gow AJ, Beck JM et al (2004c) Delayed clearance of Pneumocystis carinii infection, increased inflammation, and altered nitric oxide metabolism in lungs of surfactant protein-D knockout mice. J Infect Dis 189:1528–1539
Atochina-Vasserman EN, Beers MF et al (2007) Selective inhibition of inducible NO synthase activity in vivo reverses inflammatory abnormalities in surfactant protein D-deficient mice. J Immunol 179:8090–8097
Awasthi S (2010) Surfactant protein (SP)-A and SP-D as antimicrobial and immunotherapeutic agents. Recent Pat Antiinfect Drug Discov 5:115–123
Awasthi S, Coalson JJ, Crouch E, Yang F, King RJ (1999) Surfactant proteins A and D in premature baboons with chronic lung injury (Bronchopulmonary dysplasia). Evidence for an inhibition of secretion. Am J Respir Crit Care Med 160:942–949
Awasthi S, Magee DM, Coalson JJ (2004) Coccidioides posadasii infection alters the expression of pulmonary surfactant proteins (SP)-A and SP-D. Respir Res 5:28
Bai Y, Galetskiy D, Damoc E et al (2007) Lung alveolar proteomics of bronchoalveolar lavage from a pulmonary alveolar proteinosis patient using high-resolution FTICR mass spectrometry. Anal Bioanal Chem 389:1075–1085
Baker CS, Evans TW, Randle BJ et al (1999) Damage to surfactant-specific protein in acute respiratory distress syndrome. Lancet 353(9160):1232–1237
Balamugesh T, Kaur S, Majumdar S, Behera D (2003) Surfactant protein-A levels in patients with acute respiratory distress syndrome. Indian J Med Res 117:129–133
Ballard PL, Merrill JD, Truog WE et al (2007) Surfactant function and composition in premature infants treated with inhaled nitric oxide. Pediatrics 120:346–353
Barbaro M, Cutroneo G, Costa C, Sciorio S, et al (2002) Early events of experimental exposure to amorphous and crystalline silica in the rat: time course of surfactant protein D. Ital J Anat Embryol 107:243–256
Baron RM, Carvajal IM, Fredenburgh LE et al (2004) Nitric oxide synthase-2 down-regulates surfactant protein-B expression and enhances endotoxin-induced lung injury in mice. FASEB J 18:1276–1279
Baughman RP, Sternberg RI, Hull W et al (1993) Decreased surfactant protein A in patients with bacterial pneumonia. Am Rev Respir Dis 147:653–657
Behera D, Balamugesh T, Venkateswarlu D et al (2005) Serum surfactant protein-A levels in chronic bronchitis and its relation to smoking. Indian J Chest Dis Allied Sci 47:13–17
Benachi A, Chailley-Heu B, Barlier-Mur AM et al (2002) Expression of surfactant proteins and thyroid transcription factor 1 in an ovine model of congenital diaphragmatic hernia. J Pediatr Surg 37:1393–1399
Berg T, Leth-Larsen R, Holmskov U et al (2000) Structural characterisation of human proteinosis surfactant protein A. Biochim Biophys Acta 1543:159–173
Betsuyaku T, Kuroki Y, Nagai K, Nasuhara Y, Nishimura M (2004) Effects of ageing and smoking on SP-A and SP-D levels in bronchoalveolar lavage fluid. Eur Respir J 24:964–70
Betz C, Papadopoulos T, Buchwald J et al (1995) Surfactant protein gene expression in metastatic and micrometastatic pulmonary adenocarcinomas and other non-small cell lung carcinomas: detection by reverse transcriptase-polymerase chain reaction. Cancer Res 55:4283–4286
Botas C, Poulain F, Akiyama J et al (1998) Altered surfactant homeostasis and alveolar type II cell morphology in mice lacking surfactant protein D. Proc Natl Acad Sci USA 95:11869–11874
Bowler RP, Duda B, Chan ED et al (2004) Proteomic analysis of pulmonary edema fluid and plasma in patients with acute lung injury. Am J Physiol Lung Cell Mol Physiol 286:L1095–L1104
Brandt EB, Mingler MK, Stevenson MD et al (2008) Surfactant protein D alters allergic lung responses in mice and human subjects. J Allergy Clin Immunol 121:1140–1147, e2
Brasch F, Müller KM (2004) Classification of pulmonary alveolar proteinosis in newborns, infants, and children. Pathologe 25:299–309
Brasch F, Birzele J, Ochs M et al (2004) Surfactant proteins in pulmonary alveolar proteinosis in adults. Eur Respir J 24:426–435
Breij EC, Batenburg JJ (2008) Surfactant protein D/anti-Fc receptor bifunctional proteins as a tool to enhance host defence. Expert Opin Biol Ther 8:409–419
Broers JL, Jensen SM, Travis WD et al (1992) Expression of surfactant associated protein-A and Clara cell 10 kilodalton mRNA in neoplastic and non-neoplastic human lung tissue as detected by in situ hybridization. Lab Invest 66:337–346
Brown-Augsburger P, Hartshorn K, Chang D et al (1996) Site-directed mutagenesis of Cys-15 and Cys-20 of pulmonary surfactant protein D. Expression of a trimeric protein with altered anti-viral properties. J Biol Chem 271:13724–13730
Bufler P, Schikor D, Schmidt B, Griese M (2004) Cytokine stimulation by Pseudomonas aeruginosa – strain variation and modulation by pulmonary surfactant. Exp Lung Res 30:163–179
Camilo R, Capelozzi VL, Siqueira SA et al (2006) Expression of p63, keratin 5/6, keratin 7, and surfactant-A in non-small cell lung carcinomas. Hum Pathol 37:542–546
Casals C, Varela A, Ruano ML et al (1998) Increase of C-reactive protein and decrease of surfactant protein A in surfactant after lung transplantation. Am J Respir Crit Care Med 157:43–49
Casey J, Kaplan J, Atochina-Vasserman EN, Gow AJ (2005) Alveolar Surfactant Protein D Content Modulates Bleomycin-induced Lung Injury. Am J Respir Crit Care Med 172: 869–877
Cheah FC, Jobe AH, Moss TJ et al (2008) Oxidative stress in fetal lambs exposed to intra-amniotic endotoxin in a chorioamnionitis model. Pediatr Res 63:274–279
Cheng G, Ueda T, Numao T et al (2000) Increased levels of surfactant protein A and D in bronchoalveolar lavage fluids in patients with bronchial asthma. Eur Respir J 16:831–835
Cheng IW, Ware LB, Greene KE et al (2003) Prognostic value of surfactant proteins A and D in patients with acute lung injury. Crit Care Med 31:20–27
Chiba H, Pattanajitvilai S, Evans AJ et al (2002) Human surfactant protein D (SP-D) binds Mycoplasma pneumoniae by high affinity interactions with lipids. J Biol Chem 277:20379–20385
Cho K, Matsuda T, Okajima S et al (2000) Prediction of respiratory distress syndrome by the level of pulmonary surfactant protein A in cord blood sera. Biol Neonate 77:83–87
Chong IW, Chang MY, Chang HC et al (2006) Great potential of a panel of multiple hMTH1, SPD, ITGA11 and COL11A1 markers for diagnosis of patients with non-small cell lung cancer. Oncol Rep 16:981–988
Clark H, Reid K (2003) The potential of recombinant surfactant protein D therapy to reduce inflammation in neonatal chronic lung disease, cystic fibrosis, and emphysema. Arch Dis Child 88:981–984
Coalson JJ, King RJ, Yang F et al (1995) SP-A deficiency in primate model of bronchopulmonary dysplasia with infection. In situ mRNA and immunostains. Am J Respir Crit Care Med 151:854–866
Cogo PE, Zimmermann LJ, Rosso F et al (2002) Surfactant synthesis and kinetics in infants with congenital diaphragmatic hernia. Am J Respir Crit Care Med 166:154–159
Crouch E, Persson A, Chang D (1993) Accumulation of surfactant protein D in human pulmonary alveolar proteinosis. Am J Pathol 142:241–248
Crouch E, Tu Y, Briner D et al (2005) Ligand specificity of human surfactant protein D: expression of a mutant trimeric collectin that shows enhanced interactions with influenza A virus. J Biol Chem 280:17046–17056
Daimon T, Tajima S, Oshikawa K et al (2005) KL-6 and surfactant proteins A and D in serum and bronchoalveolar lavage fluid in patients with acute eosinophilic pneumonia. Intern Med 44:811–817
Davis IC, Zhu S, Sampson JB et al (2002) Inhibition of human surfactant protein A function by oxidation intermediates of nitrite. Free Radic Biol Med 33:1703–1713
Deb R, Shakib F, Reid K, Clark H (2007) Major house dust mite allergens Dermatophagoides pteronyssinus 1 and Dermatophagoides farinae 1 degrade and inactivate lung surfactant proteins A and D. J Biol Chem 282:36808–19
deMello DE, Heyman S, Phelps DS, Floros J (1993) Immunogold localization of SP-A in lungs of infants dying from respiratory distress syndrome. Am J Pathol 142:1631–1640
Dohmoto K, Hojo S, Fujita J et al (2000) Circulating bronchoepithelial cells expressing mRNA for surfactant protein A in patients with pulmonary fibrosis. Respir Med 94:475–481
Downing JF, Pasula R, Wright JR et al (1995) Surfactant protein A promotes attachment of Mycobacterium tuberculosis to alveolar macrophages during infection with human immunodeficiency virus. Proc Natl Acad Sci USA 92:4848–4852
Doyle IR, Nicholas TE, Bersten AD (1995) Serum surfactant protein-A levels in patients with acute cardiogenic pulmonary edema and adult respiratory distress syndrome. Am J Respir Crit Care Med 152:307–317
Doyle IR, Bersten AD, Nicholas TE (1997) Surfactant proteins-A and -B are elevated in plasma of patients with acute respiratory failure. Am J Respir Crit Care Med 156:1217–1229
Doyle IR, Davidson KG, Barr HA et al (1998) Quantity and structure of surfactant proteins vary among patients with alveolar proteinosis. Am J Respir Crit Care Med 157:658–664
Eda S, Suzuki Y, Kawai T et al (1997) Structure of a truncated human surfactant protein D is less effective in agglutinating bacteria than the native structure and fails to inhibit haemagglutination by influenza A virus. Biochem J 323:393–399
Endo S, Sato N, Nakae H, Yamada Y et al (2002) Surfactant protein A and D (SP-A, AP-D) levels in patients with septic ARDS. Res Commun Mol Pathol Pharmacol 111:245–251
Endo S, Sato N, Yaegashi Y et al (2006) Sivelestat sodium hydrate improves septic acute lung injury by reducing alveolar dysfunction. Res Commun Mol Pathol Pharmacol 119:53–65
Erasmus ME, Hofstede GJ, Petersen AH et al (2002) SP-A-enriched surfactant for treatment of rat lung transplants with SP-A deficiency after storage and reperfusion. Transplantation 73:348–352
Ernst JD (1998) Macrophage receptors for Mycobacterium tuberculosis. Infect Immun 66:1277–1281
Erpenbeck VJ, Malherbe DC, Sommer S et al (2005) Surfactant protein D increases phagocytosis and aggregation of pollen-allergen starch granules. Am J Physiol Lung Cell Mol Physiol 288:L692–L698
Erpenbeck VJ, Ziegert M, Cavalet-Blanco D et al (2006) Surfactant protein D inhibits early airway response in Aspergillus fumigatus-sensitized mice. Clin Exp Allergy 36:930–940
Ferguson JS, Voelker DR, McCormack FX, Schlesinger LS (1999) Surfactant protein D binds to Mycobacterium tuberculosis bacilli and lipoarabinomannan via carbohydrate-lectin interactions resulting in reduced phagocytosis of the bacteria by macrophages. J Immunol 163:312–321
Ferguson JS, Voelker DR, Ufnar JA et al (2002) Surfactant protein D inhibition of human macrophage uptake of Mycobacterium tuberculosis is independent of bacterial agglutination. J Immunol 168:1309–1314
Ferguson JS, Martin JL, Azad AK et al (2006) Surfactant protein D increases fusion of Mycobacterium tuberculosis-containing phagosomes with lysosomes in human macrophages. Infect Immun 74:7005–7009
Fernández-Real JM, Chico B, Shiratori M et al (2008) Circulating surfactant protein A (SP-A), a marker of lung injury, is associated with insulin resistance. Diabetes Care 31:958–963
Floros J, Fan R (2001) Surfactant protein A and B genetic variants and respiratory distress syndrome: allele interactions. Biol Neonate 80(Suppl 1):22–25
Floros J, Lin HM, García A et al (2000) Surfactant protein genetic marker alleles identify a subgroup of tuberculosis in a Mexican population. J Infect Dis 182:1473–1479
Floros J, Fan R, Diangelo S et al (2001a) Surfactant protein (SP) B associations and interactions with SP-A in white and black subjects with respiratory distress syndrome. Pediatr Int 43:567–576
Floros J, Fan R, Matthews A et al (2001b) Family-based transmission disequilibrium test (TDT) and case–control association studies reveal surfactant protein A (SP-A) susceptibility alleles for respiratory distress syndrome (RDS) and possible race differences. Clin Genet 60:178–187
Foster DJ, Yan X, Bellotto DJ et al (2002) Expression of epidermal growth factor and surfactant proteins during postnatal and compensatory lung growth. Am J Physiol Lung Cell Mol Physiol 283:L981–L990
Fujita J, Ohtsuki Y, Bandoh S et al (2003) Expression of thyroid transcription factor-1 in 16 human lung cancer cell lines. Lung Cancer 39:31–36
Fujita M, Shannon JM, Ouchi H et al (2005) Serum surfactant protein D is increased in acute and chronic inflammation in mice. Cytokine 31:25–33
Gaynor CD, McCormack FX, Voelker DR et al (1995) Pulmonary surfactant protein A mediates enhanced phagocytosis of Mycobacterium tuberculosis by a direct interaction with human macrophages. J Immunol 155:5343–5351
Ghildyal R, Hartley C, Varrasso A et al (1999) Surfactant protein A binds to the fusion glycoprotein of respiratory syncytial virus and neutralizes virion infectivity. J Infect Dis 180:2009–2013
Giannoni E, Sawa T, Allen L et al (2006) Surfactant proteins A and D enhance pulmonary clearance of Pseudomonas aeruginosa. Am J Respir Cell Mol Biol 34:704–710
Glas J, Beynon V, Bachstein B et al (2008) Increased plasma concentration of surfactant protein D in chronic periodontitis independent of SFTPD genotype: potential role as a biomarker. Tissue Antigens 72:21–28
Gold JA, Hoshino Y, Tanaka N et al (2004) Surfactant protein A modulates the inflammatory response in macrophages during tuberculosis. Infect Immun 72:645–650
Goldmann T, Kähler D, Schultz H et al (2009) On the significance of surfactant protein-A within the human lungs. Diagn Pathol 4:9
Gowdy K, Krantz QT, Daniels M, et al (2008) Modulation of pulmonary inflammatory responses and antimicrobial defenses in mice exposed to diesel exhaust. Toxicol Appl Pharmacol 229:310–9
Greene KE, King TE Jr, Kuroki Y et al (2002) Serum surfactant proteins-A and -D as biomarkers in idiopathic pulmonary fibrosis. Eur Respir J 19:439–446
Griese M (2002) Respiratory syncytial virus and pulmonary surfactant. Viral Immunol 15:357–363
Griese M, Starosta V (2005) Agglutination of Pseudomonas aeruginosa by surfactant protein D. Pediatr Pulmonol 40:378–384
Griese M, Maderlechner N, Ahrens P, Kitz R (2002) Surfactant proteins A and D in children with pulmonary disease due to gastroesophageal reflux. Am J Respir Crit Care Med 165:1546–1550
Griese M, Felber J, Reiter K, Strong P et al (2004) Airway inflammation in children with tracheostomy. Pediatr Pulmonol 37:356–361
Griese M, Steinecker M, Schumacher S et al (2008) Children with absent surfactant protein D in bronchoalveolar lavage have more frequently pneumonia. Pediatr Allergy Immunol 19:639–647
Grubor B, Gallup JM, Meyerholz DK et al (2004) Enhanced surfactant protein and defensin mRNA levels and reduced viral replication during parainfluenza virus type 3 pneumonia in neonatal lambs. Clin Diagn Lab Immunol 11:599–607
Günther A, Schmidt R, Nix F et al (1999) Surfactant abnormalities in idiopathic pulmonary fibrosis, hypersensitivity pneumonitis and sarcoidosis. Eur Respir J 14:565–573
Guo X, Lin HM, Lin Z et al (2001) Surfactant protein gene A, B, and D marker alleles in chronic obstructive pulmonary disease of a Mexican population. Eur Respir J 18:482–490
Guo CJ, Atochina-Vasserman EN, Abramova E et al (2008) S-nitrosylation of surfactant protein-D controls inflammatory function. PLoS Biol 6:e266
Gutierrez JA, Parry AJ, McMullan DM et al (2001) Decreased surfactant proteins in lambs with pulmonary hypertension secondary to increased blood flow. Am J Physiol Lung Cell Mol Physiol 281:L1264–L1270
Haataja R, Rämet M, Marttila R et al (2000) Surfactant proteins A and B as interactive genetic determinants of neonatal respiratory distress syndrome. Hum Mol Genet 9:2751–2760
Haataja R, Marttila R, Uimari P et al (2001) Respiratory distress syndrome: evaluation of genetic susceptibility and protection by transmission disequilibrium test. Hum Genet 109:351–355
Haczku A (2006) Role and regulation of lung collectins in allergic airway sensitization. Pharmacol Ther 110:14–34
Haczku A, Cao Y, Vass G et al (2006) IL-4 and IL-13 form a negative feedback circuit with surfactant protein-D in the allergic airway response. J Immunol 176:3557–3565
Hall-Stoodley L, Watts G, Crowther JE et al (2006) Mycobacterium tuberculosis binding to human surfactant proteins A and D, fibronectin, and small airway epithelial cells under shear conditions. Infect Immun 74:3587–3596
Hamm H, Lührs J, Guzman Y, Rotaeche J et al (1994) Elevated surfactant protein A in bronchoalveolar lavage fluids from sarcoidosis and hypersensitivity pneumonitis patients. Chest 106:1766–1770
Hartshorn KL, Crouch EC, White MR et al (1994) Evidence for a protective role of pulmonary surfactant protein D (SP-D) against influenza A viruses. J Clin Invest 94:311–319
Hartshorn K, Chang D, Rust K et al (1996a) Interactions of recombinant human pulmonary surfactant protein D and SP-D multimers with influenza A. Am J Physiol 271:L753–L762
Hartshorn KL, Reid KB, White MR et al (1996b) Neutrophil deactivation by influenza A viruses: mechanisms of protection after viral opsonization with collectins and hemagglutination-inhibiting antibodies. Blood 87:3450–3461
Hartshorn KL, White MR, Shepherd V et al (1997) Mechanisms of anti-influenza activity of surfactant proteins A and D: comparison with serum collectins. Am J Physiol 273:L1156–L1166
Hartshorn KL, Sastry KN, Chang D et al (2000a) Enhanced anti-influenza activity of a surfactant protein D and serum conglutinin fusion protein. Am J Physiol Lung Cell Mol Physiol 278:L90–L98
Hartshorn KL, White MR, Voelker DR et al (2000b) Mechanism of binding of surfactant protein D to influenza A viruses: importance of binding to haemagglutinin to antiviral activity. Biochem J 351:449–458
Hartshorn KL, White MR, Tecle T et al (2007) Reduced influenza viral neutralizing activity of natural human trimers of surfactant protein D. Respir Res 8:9
Hartshorn KL, White MR, Tecle T et al (2010) Viral aggregating and opsonizing activity in collectin trimers. Am J Physiol Lung Cell Mol Physiol 298:L79–L88
Hattori A, Kuroki Y, Katoh T et al (1996a) Surfactant protein A accumulating in the alveoli of patients with pulmonary alveolar proteinosis: oligomeric structure and interaction with lipids. Am J Respir Cell Mol Biol 14:608–619
Hattori A, Kuroki Y, Sohma H et al (1996b) Human surfactant protein A with two distinct oligomeric structures which exhibit different capacities to interact with alveolar type II cells. Biochem J 317:939–944
Hawgood S, Akiyama J, Brown C et al (2001) GM-CSF mediates alveolar macrophage proliferation and type II cell hypertrophy in SP-D gene-targeted mice. Am J Physiol Lung Cell Mol Physiol 280:L1148–L1156
Hawgood S, Ochs M, Jung A et al (2002) Sequential targeted deficiency of SP-A and -D leads to progressive alveolar lipoproteinosis and emphysema. Am J Physiol Lung Cell Mol Physiol 283:L1002–L1010
Heidinger K, König IR, Bohnert A et al (2005) Polymorphisms in the human surfactant protein-D (SFTPD) gene: strong evidence that serum levels of surfactant protein-D (SP-D) are genetically influenced. Immunogenetics 57:1–7
Heinrich S, Hartl D, Griese M (2006) Surfactant protein A – from genes to human lung diseases. Curr Med Chem 13:3239–3252
Hickling TP, Bright H, Wing K et al (1999) A recombinant trimeric surfactant protein D carbohydrate recognition domain inhibits respiratory syncytial virus infection in vitro and in vivo. Eur J Immunol 29:3478–3484
Highland KB, Silver RM (2005) New developments in scleroderma interstitial lung disease. Curr Opin Rheumatol 17:737–745
Hilgendorff A, Heidinger K, Bohnert A et al (2009) Association of polymorphisms in the human surfactant protein-D (SFTPD) gene and postnatal pulmonary adaptation in the preterm infant. Acta Paediatr 98:112–117
Hirama N, Shibata Y, Otake K, et al (2007) Increased surfactant protein-D and foamy macrophages in smoking-induced mouse emphysema. Respirology 12:191–201
Hobo S, Niwa H, Anzai T (2007) Evaluation of serum amyloid A and surfactant protein D in sera for identification of the clinical condition of horses with bacterial pneumonia. J Vet Med Sci 69:827–830
Hoegh SV, Lindegaard HM, Sorensen GL et al (2008) Circulating surfactant protein D is decreased in early rheumatoid arthritis: a 1-year prospective study. Scand J Immunol 67:71–76
Hohlfeld JM, Erpenbeck VJ, Krug N (2002) Surfactant proteins SP-A and SP-D as modulators of the allergic inflammation in asthma. Pathobiology 70:287–292
Honda Y, Kuroki Y, Matsuura E et al (1995) Pulmonary surfactant protein D in sera and bronchoalveolar lavage fluids. Am J Respir Crit Care Med 152:1860–1866
Honda Y, Takahashi H, Kuroki Y et al (1996) Decreased contents of surfactant proteins A and D in BAL fluids of healthy smokers. Chest 109:1006–1009
Hu X, Guo C, Sun B (2007) Inhaled nitric oxide attenuates hyperoxic and inflammatory injury without alteration of phosphatidylcholine synthesis in rat lungs. Pulm Pharmacol Ther 20:75–84
Hu QJ, Xiong SD, Zhang HL et al (2008) Altered surfactant protein A gene expression and protein homeostasis in rats with emphysematous changes. Chin Med J (Engl) 121:1177–1182
Hull J, South M, Phelan P, Grimwood K (1997) Surfactant composition in infants and young children with cystic fibrosis. Am J Respir Crit Care Med 156:161–165
Hussain S (2004) Role of surfactant protein a in the innate host defense and autoimmunity. Autoimmunity 37:125–130
Ihn H, Asano Y, Kubo M et al (2002) Clinical significance of serum surfactant protein D (SP-D) in patients with polymyositis/dermatomyositis: correlation with interstitial lung disease. Rheumatology (Oxford) 41:1268–1272
Ikegami M, Hull WM, Yoshida M et al (2001) SP-D and GM-CSF regulate surfactant homeostasis via distinct mechanisms. Am J Physiol Lung Cell Mol Physiol 281:L697–L703
Ikegami M, Na CL, Korfhagen TR, Whitsett JA (2005) Surfactant protein D influences surfactant ultrastructure and uptake by alveolar type II cells. Am J Physiol Lung Cell Mol Physiol 288:L552–L561
Ikegami M, Carter K, Bishop K et al (2006) Intratracheal recombinant surfactant protein d prevents endotoxin shock in the newborn preterm lamb. Am J Respir Crit Care Med 173:1342–1347
Ikegami M, Scoville EA, Grant S et al (2007) Surfactant protein-D and surfactant inhibit endotoxin-induced pulmonary inflammation. Chest 132:1447–1454
Inase N, Ohtani Y, Usui Y et al (2007) Chronic summer-type hypersensitivity pneumonitis: clinical similarities to idiopathic pulmonary fibrosis. Sarcoidosis Vasc Diffuse Lung Dis 24:141–147
Inoue A, Xin H, Suzuki T et al (2008) Suppression of surfactant protein A by an epidermal growth factor receptor tyrosine kinase inhibitor exacerbates lung inflammation. Cancer Sci 99:1679–1684
Ishida K, Zhu BL, Maeda H (2002) A quantitative RT-PCR assay of surfactant-associated protein A1 and A2 mRNA transcripts as a diagnostic tool for acute asphyxial death. Leg Med (Tokyo) 4:7–12
Ishiguro T, Yasui M, Takato H et al (2007) Progression of interstitial lung disease upon overlapping of systemic sclerosis with polymyositis. Intern Med 46:1237–1241
Ishii H, Mukae H, Kadota J et al (2003) High serum concentrations of surfactant protein A in usual interstitial pneumonia compared with non-specific interstitial pneumonia. Thorax 58:52–57
Jack DL, Cole J, Naylor SC et al (2006) Genetic polymorphism of the binding domain of surfactant protein-A2 increases susceptibility to meningococcal disease. Clin Infect Dis 43:1426–1433
Janssen R, Sato H, Grutters JC et al (2003) Study of Clara cell 16, KL-6, and surfactant protein-D in serum as disease markers in pulmonary sarcoidosis. Chest 124:2119–2125
Janssen R, Grutters JC, Sato H et al (2005) Analysis of KL-6 and SP-D as disease markers in bird fancier’s lung. Sarcoidosis Vasc Diffuse Lung Dis 22:51–57
Jiang F, Caraway NP, Nebiyou Bekele B et al (2005) Surfactant protein A gene deletion and prognostics for patients with stage I non-small cell lung cancer. Clin Cancer Res 11:5417–5424
Jounblat R, Kadioglu A, Iannelli F et al (2004) Binding and agglutination of Streptococcus pneumoniae by human surfactant protein D (SP-D) vary between strains, but SP-D fails to enhance killing by neutrophils. Infect Immun 72:709–716
Jung A, Allen L, Nyengaard JR et al (2005) Design-based stereological analysis of the lung parenchymal architecture and alveolar type II cells in surfactant protein A and D double deficient mice. Anat Rec A Discov Mol Cell Evol Biol 286:885–890
Kala P, Ten Have T, Nielsen H et al (1998) Association of pulmonary surfactant protein A (SP-A) gene and respiratory distress syndrome: interaction with SP-B. Pediatr Res 43:169–177
Kankavi O (2006) Increased expression of surfactant protein A and D in rheumatoid arthritic synovial fluid (RASF). Croat Med J 47:155–161
Kashiwabara K (2006) Characteristics and disease activity of early interstitial lung disease in subjects with true parenchymal abnormalities in the posterior subpleural aspect of the lung. Chest 129:402–406
Kasper M, Sims G, Koslowski R et al (2002) Increased surfactant protein D in rat airway goblet and Clara cells during ovalbumin-induced allergic airway inflammation. Clin Exp Allergy 32:1251–1258
Kerr MH, Paton JY (1999) Surfactant protein levels in severe respiratory syncytial virus infection. Am J Respir Crit Care Med 159:1115–1118
Keisari Y, Wang H, Mesika A et al (2001) Surfactant protein D-coated Klebsiella pneumoniae stimulates cytokine production in mononuclear phagocytes. J Leukoc Biol 70:135–141
King RJ, Coalson JJ, deLemos RA et al (1995) Surfactant protein-A deficiency in a primate model of bronchopulmonary dysplasia. Am J Respir Crit Care Med 151:1989–1997
Kishore U, Bernal AL, Kamran MF et al (2005) Surfactant proteins SP-A and SP-D in human health and disease. Arch Immunol Ther Exp 53:399–417
Kitajima H, Takahashi H, Harada K et al (2006) Gefitinib-induced interstitial lung disease showing improvement after cessation: disassociation of serum markers. Respirology 11:217–220
Knudsen L, Ochs M, Mackay R et al (2007) Truncated recombinant human SP-D attenuates emphysema and type II cell changes in SP-D deficient mice. Respir Res 8:70
Knudsen L, Wucherpfennig K, MackaY R-M et al (2009) A recombinant fragment of human surfactant protein D lacking the short collagen-like stalk fails to correct morphological alterations in lungs of SP-D deficient mice. Anat Rec 292:183–189
Kobayashi H, Kanoh S, Motoyoshi K (2008a) Serum surfactant protein-A, but not surfactant protein-D or KL-6, can predict preclinical lung damage induced by smoking. Biomarkers 13:385–392
Kobayashi M, Takeuchi T, Ohtsuki Y (2008b) Differences in the immunolocalization of surfactant protein (SP)-A, SP-D, and KL-6 in pulmonary alveolar proteinosis. Pathol Int 58:203–207
Kodera M, Hasegawa M, Komura K et al (2005) Serum pulmonary and activation-regulated chemokine/CCL18 levels in patients with systemic sclerosis: a sensitive indicator of active pulmonary fibrosis. Arthritis Rheum 52:2889–2896
Konishi M, Nishitani C, Mitsuzawa H et al (2006) Alloiococcus otitidis is a ligand for collectins and Toll-like receptor 2, and its phagocytosis is enhanced by collectins. Eur J Immunol 36:1527–1536
Koopmans JG, van der Zee JS, Krop EJ et al (2004) Serum surfactant protein D is elevated in allergic patients. Clin Exp Allergy 34:1827–1833
Korfhagen TR, Sheftelyevich V, Burhans MS et al (1998) Surfactant protein-D regulates surfactant phospholipid homeostasis in vivo. J Biol Chem 273:28438–28443
Krueger M, Puthothu B, Gropp E et al (2006) Amino acid variants in surfactant protein D are not associated with bronchial asthma. Pediatr Allergy Immunol 17:77–81
Kuan SF, Rust K, Crouch E (1992) Interactions of surfactant protein D with bacterial lipopolysaccharides. Surfactant protein D is an Escherichia coli- binding protein in bronchoalveolar lavage. J Clin Invest 90:97–106
Kudo K, Sano H, Takahashi H et al (2004) Pulmonary collectins enhance phagocytosis of Mycobacterium avium through increased activity of mannose receptor. J Immunol 172:7592–7602
Kumánovics G, Minier T, Radics J et al (2008) Comprehensive investigation of novel serum markers of pulmonary fibrosis associated with systemic sclerosis and dermato/polymyositis. Clin Exp Rheumatol 26:414–420
Kunitake R, Kuwano K, Yoshida K et al (2001) KL-6, surfactant protein A and D in bronchoalveolar lavage fluid from patients with pulmonary sarcoidosis. Respiration 68:488–495
Kuroki Y, Tsutahara S, Shijubo N et al (1993) Elevated levels of lung surfactant protein A in sera from patients with idiopathic pulmonary fibrosis and pulmonary alveolar proteinosis. Am Rev Respir Dis 147:723–729
Kuroki Y, Takahashi H, Chiba H, Akino T (1998) Surfactant proteins A and D: disease markers. Biochim Biophys Acta 1408:334–345
Kuronuma K, Sano H, Kato K et al (2004) Pulmonary surfactant protein A augments the phagocytosis of Streptococcus pneumoniae by alveolar macrophages through a casein kinase 2-dependent increase of cell surface localization of scavenger receptor A. J Biol Chem 279:21421–21430
Lang JD, McArdle PJ, O’Reilly PJ et al (2002) Oxidant-antioxidant balance in acute lung injury. Chest 122(6 Suppl):314S–320S
Lazic T, Wyatt TA, Matic M, Meyerholz DK et al (2007) Maternal alcohol ingestion reduces surfactant protein A expression by preterm fetal lung epithelia. Alcohol 41:347–55
Lee JW, Ovadia B, Azakie A et al (2004) Increased pulmonary blood flow does not alter surfactant protein gene expression in lambs within the first week of life. Am J Physiol Lung Cell Mol Physiol 286:L1237–L1243
Lee HM, Kang HJ, Woo JS et al (2006) Upregulation of surfactant protein A in chronic rhinosinusitis. Laryngoscope 116:328–330
Lekkala M, LeVine AM, Linke MJ et al (2006) Effect of lung surfactant collectins on bronchoalveolar macrophage interaction with Blastomyces dermatitidis: inhibition of tumor necrosis factor alpha production by surfactant protein D. Infect Immun 74:4549–4556
Leth-Larsen R, Nordenbaek C, Tornoe I et al (2003) Surfactant protein D (SP-D) serum levels in patients with community-acquired pneumonia small star, filled. Clin Immunol 108:29–37
Leth-Larsen R, Garred P, Jensenius H et al (2005) A common polymorphism in the SFTPD gene influences assembly, function, and concentration of surfactant protein D. J Immunol 174:1532–1538
LeVine AM, Lotze A, Stanley S et al (1996) Surfactant content in children with inflammatory lung disease. Crit Care Med 246:1062–1067
LeVine AM, Whitsett JA, Gwozdz JA et al (2000) Distinct effects of surfactant protein A or D deficiency during bacterial infection on the lung. J Immunol 165:3934–3940
LeVine AM, Whitsett JA, Hartshorn KL et al (2001) Surfactant protein D enhances clearance of influenza A virus from the lung in vivo. J Immunol 167:5868–5873
LeVine AM, Elliott J, Whitsett JA et al (2004) Surfactant protein-D enhances phagocytosis and pulmonary clearance of respiratory syncytial virus. Am J Respir Cell Mol Biol 31:193–199
Lim BL, Wang JY, Holmskov U et al (1994) Expression of the carbohydrate recognition domain of lung surfactant protein D and demonstration of its binding to lipopolysaccharides of gram-negative bacteria. Biochem Biophys Res Commun 202:1674–1680
Lin Z, Pearson C, Chinchilli V et al (2000) Polymorphisms of human SP-A, SP-B, and SP-D genes: association of SP-B Thr131Ile with ARDS. Clin Genet 58:181–191
Linnoila RI, Mulshine JL, Steinberg SM, Gazdar AF (1992) Expression of surfactant-associated protein in non-small-cell lung cancer: a discriminant between biologic subsets. J Natl Cancer Inst Monogr 13:61–66
Liu CF, Chen YL, Chang WT et al (2005a) Mite allergen induces nitric oxide production in alveolar macrophage cell lines via CD14/toll-like receptor 4, and is inhibited by surfactant protein D. Clin Exp Allergy 35:1615–1624
Liu CF, Chen YL, Shieh CC et al (2005) Therapeutic effect of surfactant protein D in allergic inflammation of mite-sensitized mice. Clin Exp Allergy 35:515–521
Lopez JP, Clark E, Shepherd VL (2003) Surfactant protein A enhances Mycobacterium avium ingestion but not killing by rat macrophages. J Leukoc Biol 74:523–530
Lu SH, Ohtsuki Y, Nonami Y et al (2006) Ultrastructural study of nuclear inclusions immunohistochemically positive for surfactant protein A in pulmonary adenocarcinoma with special reference to their morphogenesis. Med Mol Morphol 39:214–220
Madan T, Eggleton P, Kishore U et al (1997a) Binding of pulmonary surfactant proteins A and D to Aspergillus fumigatus conidia enhances phagocytosis and killing by human neutrophils and alveolar macrophages. Infect Immun 65:3171–3179
Madan T, Kishore U, Shah A et al (1997b) Lung surfactant proteins A and D can inhibit specific IgE binding to the allergens of Aspergillus fumigatus and block allergen-induced histamine release from human basophils. Clin Exp Immunol 110:241–249
Madan T, Saxena S, Murthy KJ et al (2002) Association of polymorphisms in the collagen region of human SP-A1 and SP-A2 genes with pulmonary tuberculosis in Indian population. Clin Chem Lab Med 40:1002–1009
Madan T, Kaur S, Saxena S et al (2005) Role of collectins in innate immunity against aspergillosis. Med Mycol 43(Suppl 1):S155–S163
Maeda M, Ichiki Y, Aoyama Y et al (2001) Surfactant protein D (SP-D) and systemic scleroderma (SSc). J Dermatol 28:467–474
Mahajan L, Madan T, Kamal N et al (2008) Recombinant surfactant protein-D selectively increases apoptosis in eosinophils of allergic asthmatics and enhances uptake of apoptotic eosinophils by macrophages. Int Immunol 20:993–1007
Malhotra R, Haurum JS, Thiel S, Sim RB (1994) Binding of human collectins (SP-A and MBP) to influenza virus. Biochem J 304:455–461
Malik S, Greenwood CM, Eguale T et al (2006) Variants of the SFTPA1 and SFTPA2 genes and susceptibility to tuberculosis in Ethiopia. Hum Genet 118:752–759
Malloy JL, Veldhuizen RA, Thibodeaux BA et al (2005) Pseudomonas aeruginosa protease IV degrades surfactant proteins and inhibits surfactant host defense and biophysical functions. Am J Physiol Lung Cell Mol Physiol 288:L409–L418
Marttila R, Haataja R, Guttentag S et al (2003a) Surfactant protein A and B genetic variants in respiratory distress syndrome in singletons and twins. Am J Respir Crit Care Med 168:1216–1222
Marttila R, Haataja R, Rämet M et al (2003b) Surfactant protein A gene locus and respiratory distress syndrome in Finnish premature twin pairs. Ann Med 35:344–352
Matalon S, Shrestha K, Kirk M et al (2009) Modification of surfactant protein D by reactive oxygen-nitrogen intermediates is accompanied by loss of aggregating activity, in vitro and in vivo. FASEB J 23(5):1415–1430
Matsuno Y, Satoh H, Ishikawa H et al (2006) Simultaneous measurements of KL-6 and SP-D in patients undergoing thoracic radiotherapy. Med Oncol 23:75–82
McCormack FX, King TE Jr, Bucher BL et al (1995) Surfactant protein A predicts survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med 152:751–759
McMahan MJ, Mimouni F, Miodovnik M et al (1987) Surfactant associated protein (SAP-35) in amniotic fluid from diabetic and nondiabetic pregnancies.Obstet Gynecol 70:94–8
Meloni F, Salvini R, Bardoni AM et al (2007) Bronchoalveolar lavage fluid proteome in bronchiolitis obliterans syndrome: possible role for surfactant protein A in disease onset. J Heart Lung Transplant 26:1135–1143
Meschi J, Crouch EC, Skolnik P et al (2005) Surfactant protein D binds to human immunodeficiency virus (HIV) envelope protein gp120 and inhibits HIV replication. J Gen Virol 86:3097–3107
Meyerholz DK, Kawashima K, Gallup JM, Grubor B, Ackermann MR (2006) Expression of select immune genes (surfactant proteins A and D, sheep beta defensin 1, and Toll-like receptor 4) by respiratory epithelia is developmentally regulated in the preterm neonatal lamb. Dev Comp Immunol 30:1060–1069
Miakotina OL, Goss KL, Snyder JM (2002) Insulin utilizes the PI 3-kinase pathway to inhibit SP-A gene expression in lung epithelial cells. Respir Res 3:27
Miyata M, Sakuma F, Fukaya E et al (2002) Detection and monitoring of methotrexate-associated lung injury using serum markers KL-6 and SP-D in rheumatoid arthritis. Intern Med 41:467–473
Müller B, Barth P, von Wichert P (1992) Structural and functional impairment of surfactant protein A afterexposure to nitrogen dioxide in rats. Am J Physiol 263(2 Pt 1):L177–84
Mutti A, Corradi M, Goldoni M et al (2006) Exhaled metallic elements and serum pneumoproteins in asymptomatic smokers and patients with COPD or asthma. Chest 129:1288–1297
Mysore MR, Margraf LR, Jaramillo MA et al (1998) Surfactant protein A is decreased in a rat model of congenital diaphragmatic hernia. Am J Respir Crit Care Med 157:654–657
Nakamura N, Miyagi E, Murata S et al (2002) Expression of thyroid transcription factor-1 in normal and neoplastic lung tissues. Mod Pathol 15:1058–67
Nakamura M, Ogura T, Miyazawa N et al (2007) Outcome of patients with acute exacerbation of idiopathic interstitial fibrosis (IPF) treated with sivelestat and the prognostic value of serum KL-6 and surfactant protein D. Nihon Kokyuki Gakkai Zasshi 45:455–459
Nakane T, Nakamae H, Kamoi H et al (2008) Prognostic value of serum surfactant protein D level prior to transplant for the development of bronchiolitis obliterans syndrome and idiopathic pneumonia syndrome following allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant 42:43–49
Narasaraju TA, Jin N, Narendranath CR et al (2003) Protein nitration in rat lungs during hyperoxia exposure: a possible role of myeloperoxidase. Am J Physiol Lung Cell Mol Physiol 285:L1037–L1045
Noah TL, Murphy PC, Alink JJ et al (2003) Bronchoalveolar lavage fluid surfactant protein-A and surfactant protein-D are inversely related to inflammation in early cystic fibrosis. Am J Respir Crit Care Med 168:685–691
Nomori H, Horio H, Fuyuno G et al (1998) Serum surfactant protein A levels in healthy individuals are increased in smokers. Lung 176:355–361
Ochs M, Knudsen L, Allen L, Stumbaugh A, Levitt S, Nyengaard JR, Hawgood S (2004) GM-CSF mediates alveolar epithelial type II cell changes, but not emphysema-like pathology, in SP-D-deficient mice. Am J Physiol Lung Cell Mol Physiol 287:L1333–L1341
Ofek I, Mesika A, Kalina M et al (2001) Surfactant protein D enhances phagocytosis and killing of unencapsulated phase variants of Klebsiella pneumoniae. Infect Immun 69:24–33
Ogawa N, Shimoyama K, Kawabata H et al (2003) Clinical significance of serum KL-6 and SP-D for the diagnosis and treatment of interstitial lung disease in patients with diffuse connective tissue disorders. Ryumachi 43:19–28
Ohbayashi H, Adachi M (2008) Hydrofluoroalkane-beclomethasone dipropionate effectively improves airway eosinophilic inflammation including the distal airways of patients with mild to moderate persistent asthma as compared with fluticasone propionate in a randomized open double-cross study. Allergol Int 57:231–239
Ohlmeier S, Vuolanto M, Toljamo T et al (2008) Proteomics of human lung tissue identifies surfactant protein A as a marker of chronic obstructive pulmonary disease. J Proteome Res 7:5125–5132
Ohnishi H, Yokoyama A, Kondo K et al (2002) Comparative study of KL-6, surfactant protein-A, surfactant protein-D, and monocyte chemoattractant protein-1 as serum markers for interstitial lung diseases. Am J Respir Crit Care Med 165:378–381
Ohtsuki Y, Nakanishi N, Fujita J et al (2007) Immunohistochemical distribution of SP-D, compared with that of SP-A and KL-6, in interstitial pneumonias. Med Mol Morphol 40:163–167
Ohtsuki Y, Kobayashi M, Yoshida S et al (2008) Immunohistochemical localisation of surfactant proteins A and D, and KL-6 in pulmonary alveolar proteinosis. Pathology 40:536–539
O’Riordan DM, Standing JE, Kwon KY et al (1995) Surfactant protein D interacts with Pneumocystis carinii and mediates organism adherence to alveolar macrophages. J Clin Invest 95:2699–2710
Pasula R, Wright JR, Kachel DL et al (1999) Surfactant protein A suppresses reactive nitrogen intermediates by alveolar macrophages in response to Mycobacterium tuberculosis. J Clin Invest 103:483–490
Pavlovic J, Papagaroufalis C, Xanthou M et al (2006) Genetic variants of surfactant proteins A, B, C, and D in bronchopulmonary dysplasia. Dis Markers 22:277–291
Pettigrew MM, Gent JF, Zhu Y et al (2006) Association of surfactant protein A polymorphisms with otitis media in infants at risk for asthma. BMC Med Genet 7:69
Pettigrew MM, Gent JF, Zhu Y et al (2007) Respiratory symptoms among infants at risk for asthma: association with surfactant protein A haplotypes. BMC Med Genet 8:15
Phelps DS, Umstead TM, Mejia M et al (2004) Increased surfactant protein-A levels in patients with newly diagnosed idiopathic pulmonary fibrosis. Chest 125:617–625
Pilling AM, Mifsud NA, Jones SA et al (1999) Expression of surfactant protein mRNA in normal and neoplastic lung of B6C3F1 mice as demonstrated by in situ hybridization. Vet Pathol 36:57–63
Platt JA, Kraipowich N, Villafane F et al (2002) Alveolar type II cells expressing jaagsiekte sheep retrovirus capsid protein and surfactant proteins are the predominant neoplastic cell type in ovine pulmonary adenocarcinoma. Vet Pathol 39:341–352
Pryhuber GS, Hull WM, Fink I et al (1991) Ontogeny of surfactant proteins A and B in human amniotic fluid as indices of fetal lung maturity. Pediatr Res 30:597–605
Qi ZL, Xiao L, Gao YT et al (2002) Expression and clinical significance of surfactant protein D mRNA in peripheral blood of lung cancer patients. Ai Zheng 21:772–775, Abstract
Ragas A, Roussel L, Puzo G et al (2007) The Mycobacterium tuberculosis cell-surface glycoprotein Apa as a potential adhesin to colonize target cells via the innate immune system pulmonary C-type lectin surfactant protein A. J Biol Chem 282:5133–5142
Rämet M, Haataja R, Marttila R et al (2000) Association between the surfactant protein A (SP-A) gene locus and respiratory-distress syndrome in the Finnish population. Am J Hum Genet 66:1569–1579
Reed JA, Ikegami M, Robb L et al (2000) Distinct changes in pulmonary surfactant homeostasis in common β-chain- and GM-CSF-deficient mice. Am J Physiol Lung Cell Mol Physiol 278:L1164–L1171
Restrepo CI, Dong Q, Savov J et al (1999) Surfactant protein D stimulates phagocytosis of Pseudomonas aeruginosa by alveolar macrophages. Am J Respir Cell Mol Biol 21:576–585
Rivière M, Moisand A, Lopez A, Puzo G (2004) Highly ordered supra-molecular organization of the mycobacterial lipoarabinomannans in solution. Evidence of a relationship between supra-molecular organization and biological activity. J Mol Biol 344:907–919
Rossi G, Cavazza A, Sturm N et al (2003) Pulmonary carcinomas with pleomorphic, sarcomatoid, or sarcomatous elements: a clinicopathologic and immunohistochemical study of 75 cases. Am J Surg Pathol 27:311–324
Rubio F, Cooley J, Accurso FJ et al (2004) Linkage of neutrophil serine proteases and decreased surfactant protein-A (SP-A) levels in inflammatory lung disease. Thorax 59:318–323
Saitoh H, Shimura S, Fushimi T et al (1997) Detection of surfactant protein-A gene transcript in the cells from pleural effusion for the diagnosis of lung adenocarcinoma. Am J Med 103:400–404
Samten B, Townsend JC, Sever-Chroneos Z et al (2008) An antibody against the surfactant protein A (SP-A)-binding domain of the SP-A receptor inhibits T cell-mediated immune responses to Mycobacterium tuberculosis. J Leukoc Biol 84:115–123
Saxena S, Madan T, Shah A et al (2003) Association of polymorphisms in the collagen region of SP-A2 with increased levels of total IgE antibodies and eosinophilia in patients with allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol 111:1001–1007
Saxena S, Kumar R, Madan T et al (2005) Association of polymorphisms in pulmonary surfactant protein A1 and A2 genes with high-altitude pulmonary edema. Chest 128:1611–1619
Scanlon ST, Milovanova T, Kierstein S et al (2005) Surfactant protein-A inhibits Aspergillus fumigatus-induced allergic T-cell responses. Respir Res 6:97
Schaeffer LM, McCormack FX, Wu H, Weiss AA (2004) Interactions of pulmonary collectins with Bordetella bronchiseptica and Bordetella pertussis lipopolysaccharide elucidate the structural basis of their antimicrobial activities. Infect Immun 72:7124–7130
Schaub B, Westlake RM, He H et al (2004) Surfactant protein D deficiency influences allergic immune responses. Clin Exp Allergy 34:1819–1826
Schelenz S, Malhotra R, Sim RB et al (1995) Binding of host collectins to the pathogenic yeast Cryptococcus neoformans: human surfactant protein D acts as an agglutinin for acapsular yeast cells. Infect Immun 63:3360–3366
Schmiedl A, Lührmann A, Pabst R, Koslowski R (2008) Increased surfactant protein A and D expression in acute ovalbumin-induced allergic airway inflammation in Brown Norway rats. Int Arch Allergy Immunol 148:118–126
Seifart C, Lin HM, Seifart U et al (2005) Rare SP-A alleles and the SP-A1-6A4 allele associate with risk for lung carcinoma. Clin Genet 68:128–136
Selman M, Lin HM, Montaño M et al (2003) Surfactant protein A and B genetic variants predispose to idiopathic pulmonary fibrosis. Hum Genet 113:542–550
Shijubo N, Tsutahara S, Hirasawa M, Takahashi H, Honda Y, Suzuki A, Kuroki Y, Akino T (1992) Pulmonary surfactant protein A in pleural effusions. Cancer 69:2905–2909
Shijubo N, Honda Y, Itoh Y et al (1998) BAL surfactant protein A and Clara cell 10-kDa protein levels in healthy subjects. Lung 176:257–265
Shima H, Guarino N, Puri P (2000) Effect of hyperoxia on surfactant protein gene expression in hypoplastic lung in nitrofen-induced diaphragmatic hernia in rats. Pediatr Surg Int 16:473–477
Shimoya K, Taniguchi T, Matsuzaki N et al (2000) Chorioamnionitis decreased incidence of respiratory distress syndrome by elevating fetal interleukin-6 serum concentration. Hum Reprod 15:2234–2240
Shimura S, Masuda T, Takishima T et al (1996) Surfactant protein-A concentration in airway secretions for the detection of pulmonary oedema. Eur Respir J 9:2525–2530
Shu LH, Xue XD, Shu LH et al (2007) Effect of dexamethasone on the content of pulmonary surfactant protein D in young rats with acute lung injury induced by lipopolysaccharide. Zhongguo Dang Dai Er Ke Za Zhi 9:155–158
Sidobre S, Nigou J, Puzo G, Rivière M (2000) Lipoglycans are putative ligands for the human pulmonary surfactant protein A attachment to mycobacteria. Critical role of the lipids for lectin-carbohydrate recognition. J Biol Chem 275:2415–2422
Sidobre S, Puzo G, Rivière M (2002) Lipid-restricted recognition of mycobacterial lipoglycans by human pulmonary surfactant protein A: a surface-plasmon-resonance study. Biochem J 365:89–97
Simpson JL, Grissell TV, Douwes J et al (2007) Innate immune activation in neutrophilic asthma and bronchiectasis. Thorax 62:211–219
Sims MW, Tal-Singer RM, Kierstein S et al (2008) Chronic obstructive pulmonary disease and inhaled steroids alter surfactant protein D (SP-D) levels: a cross-sectional study. Respir Res 9:13
Sin DD, Man SF, Marciniuk DD et al (2008a) The effects of fluticasone with or without salmeterol on systemic biomarkers of inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 177:1207–1214
Sin DD, Man SF, McWilliams A, Lam S (2008b) Surfactant protein D and bronchial dysplasia in smokers at high risk of lung cancer. Chest 134:582–588
Sin DD, Pahlavan PS, Man SF (2008c) Surfactant protein D: a lung specific biomarker in COPD? Ther Adv Respir Dis 2:65–74
Singh M, Madan T, Waters P et al (2003) Protective effects of a recombinant fragment of human surfactant protein D in a murine model of pulmonary hypersensitivity induced by dust mite allergens. Immunol Lett 86:299–307
Skinner ML, Schlosser RJ, Lathers D et al (2007) Innate and adaptive mediators in cystic fibrosis and allergic fungal rhinosinusitis. Am J Rhinol 21:538–541
Snyder JM, Kwun JE, O’Brien JA et al (1988) The concentration of the 35-kDa surfactant apoprotein in amniotic fluid from normal and diabetic pregnancies. Pediatr Res 24:728–734
Sorensen GL, Madsen J, Kejling K et al (2006) Surfactant protein D is proatherogenic in mice. Am J Physiol Heart Circ Physiol 290:H2286–H2294
Sorensen GL, Husby S, Holmskov U (2007) Surfactant protein A and surfactant protein D variation in pulmonary disease. Immunobiology 212:381–416
Stamme C, Walsh E, Wright JR (2000) Surfactant protein A differentially regulates IFN-γ- and LPS-induced nitrite production by rat alveolar macrophages. Am J Respir Cell Mol Biol 23:772–779
Starosta V, Griese M (2006) Oxidative damage to surfactant protein D in pulmonary diseases. Free Radic Res 40:419–425
Stevens PA, Schadow B, Bartholain S et al (1992) Surfactant protein A in the course of respiratory distress syndrome. Eur J Pediatr 151:596–600
Stoffers M, Goldmann T, Branscheid D et al (2004) Transcriptional activity of surfactant-apoproteins A1 and A2 in non small cell lung carcinomas and tumor-free lung tissues. Pneumologie 58:395–399 [Article in German]
Stokes RW, Thorson LM, Speert DP (1998) Nonopsonic and opsonic association of Mycobacterium tuberculosis with resident alveolar macrophages is inefficient. J Immunol 160:5514–5521
Strayer DS, Merritt TA, Hallman M (1995) Levels of SP-A-anti-SP-A immune complexes in neonatal respiratory distress syndrome correlate with subsequent development of bronchopulmonary dysplasia. Acta Paediatr 84:128–131
Stray-Pedersen A, Vege A, Opdal SH et al (2009) Surfactant protein A and D gene polymorphisms and protein expression in victims of sudden infant death. Acta Paediatr 98:62–69
Stuart RB, Ovadia B, Suzara VV et al (2003) Inhaled nitric oxide increases surfactant protein gene expression in the intact lamb. Am J Physiol Lung Cell Mol Physiol 285:L628–L633
Suematsu E, Miyamura T, Shimada H et al (2003) Assessment of serum markers KL-6 and SP-D for interstitial pneumonia associated with connective tissue diseases. Ryumachi 43:11–18
Sugahara K, Iyama K, Sano K et al (1994) Differential expressions of surfactant protein SP-A, SP-B, and SP-C mRNAs in rats with streptozotocin-induced diabetes demonstrated by in situ hybridization. Am J Respir Cell Mol Biol 11:397–404
Suzuki A, Shijubo N, Yamada G et al (2005) Napsin A is useful to distinguish primary lung adenocarcinoma from adenocarcinomas of other organs. Pathol Res Pract 20:579–586
Swenson ER, Maggiorini M, Mongovin S et al (2002) Pathogenesis of high-altitude pulmonary edema: inflammation is not an etiologic factor. JAMA 287:2228–2235
Tacken PJ, Hartshorn KL, White MR et al (2004) Effective targeting of pathogens to neutrophils via chimeric surfactant protein D/anti-CD89 protein. J Immunol 172:4934–4940
Tacken PJ, Batenburg JJ (2006) Monocyte CD64 or CD89 targeting by surfactant protein D/anti-Fc receptor mediates bacterial uptake. Immunology. 117:494–501
Takahashi H, Fujishima T, Koba H et al (2000) Serum surfactant proteins A and D as prognostic factors in idiopathic pulmonary fibrosis and their relationship to disease extent. Am J Respir Crit Care Med 162:1109–1114
Takahashi H, Imai Y, Fujishima T et al (2001) Diagnostic significance of surfactant proteins A and D in sera from patients with radiation pneumonitis. Eur Respir J 17:481–487
Takahashi H, Chiba H, Shiratori M et al (2006a) Elevated serum surfactant protein A and D in pulmonary alveolar microlithiasis. Respirology 11:330–333
Takahashi H, Shiratori M, Kanai A et al (2006b) Monitoring markers of disease activity for interstitial lung diseases with serum surfactant proteins A and D. Respirology 11:S51–S54
Takami T, Kumada A, Takei Y et al (2003) A case of Wilson-Mikity syndrome with high serum KL-6 levels. J Perinatol 23:56–58
Takeda K, Miyahara N, Rha YH, Gelfand EW et al (2003) Surfactant protein D regulates airway function and allergic inflammation through modulation of macrophage function. Am J Respir Crit Care Med 168:783–789
Tecle T, White MR, Gantz D et al (2007) Human neutrophil defensins increase neutrophil uptake of influenza A virus and bacteria and modify virus-induced respiratory burst responses. J Immunol 178:8046–8052
Tecle T, White MR, Sorensen G et al (2008) Critical role for cross-linking of trimeric lectin domains of surfactant protein D in antiviral activity against influenza A virus. Biochem J 412:323–329
ter Horst SA, Fijlstra M, Sengupta S et al (2006) Spatial and temporal expression of surfactant proteins in hyperoxia-induced neonatal rat lung injury. BMC Pulm Med 6:9
Thomas NJ, Fan R, Diangelo S et al (2007) Haplotypes of the surfactant protein genes A and D as susceptibility factors for the development of respiratory distress syndrome. Acta Paediatr 96:985–989
Trinder PK, Hickling TP, Sim RB et al (2000) Humoral autoreactivity directed against surfactant protein-A (SP-A) in rheumatoid arthritis synovial fluids. Clin Exp Immunol 120:183–187
Tsutsumida H, Nomoto M, Goto M et al (2007) A micropapillary pattern is predictive of a poor prognosis in lung adenocarcinoma, and reduced surfactant apoprotein A expression in the micropapillary pattern is an excellent indicator of a poor prognosis. Mod Pathol 20:638–647
Ueno T, Linder S, Elmberger G (2003) Aspartic proteinase napsin is a useful marker for diagnosis of primary lung adenocarcinoma. Br J Cancer 88:1229–1233
Uzaslan E, Stuempel T, Ebsen M et al (2005) Surfactant protein A detection in primary pulmonary adenocarcinoma without bronchioloalveolar pattern. Respiration 72:249–253
Uzaslan E, Ebsen M, Stuempel T et al (2006) Surfactant protein A detection in large cell carcinoma of the lung. Appl Immunohistochem Mol Morphol 14:88–90
Vaid M, Kaur S, Sambatakou H et al (2007) Distinct alleles of mannose-binding lectin (MBL) and surfactant proteins A (SP-A) in patients with chronic cavitary pulmonary aspergillosis and allergic bronchopulmonary aspergillosis. Clin Chem Lab Med 45:183–186
van de Graaf EA, Jansen HM, Lutter R et al (1992) Surfactant protein A in bronchoalveolar lavage fluid. J Lab Clin Med 120:252–263
van de Wetering JK, Coenjaerts FE et al (2004) Aggregation of Cryptococcus neoformans by surfactant protein D is inhibited by its capsular component glucuronoxylomannan. Infect Immun 72:145–153
van Iwaarden JF, Pikaar JC, Storm J et al (1994) Binding of surfactant protein A to the lipid A moiety of bacterial lipopolysaccharides. Biochem J 303 (Pt 2):407–411
van Rozendaal BA, van de Lest CH, van Eijk M et al (1999) Aerosolized endotoxin is immediately bound by pulmonary surfactant protein D in vivo. Biochim Biophys Acta 1454:261–269
van Rozendaal BA, van Spriel AB, van De Winkel JG, Haagsman HP (2000) Role of pulmonary surfactant protein D in innate defense against Candida albicans. J Infect Dis 182:917–922
von Bredow C, Birrer P, Griese M (2001) Surfactant protein A and other bronchoalveolar lavage fluid proteins are altered in cystic fibrosis. Eur Respir J 17:716–722
von Bredow C, Wiesener A, Griese M (2003) Proteolysis of surfactant protein D by cystic fibrosis relevant proteases. Lung 181:79–88
Voss T, Schäfer KP, Nielsen PF et al (1992) Primary structure differences of human surfactant-associated proteins isolated from normal and proteinosis lung. Biochim Biophys Acta 1138:261–267
Vuk-Pavlovic Z, Standing JE, Crouch EC et al (2001) Carbohydrate recognition domain of surfactant protein D mediates interactions with Pneumocystis carinii glycoprotein A. Am J Respir Cell Mol Biol 24:475–484
Walenkamp AM, Verheul AF, Scharringa J, Hoepelman IM (1999) Pulmonary surfactant protein A binds to Cryptococcus neoformans without promoting phagocytosis. Eur J Clin Invest 29:83–92
Wang JY, Reid KB (2007) The immunoregulatory roles of lung surfactant collectins SP-A, and SP-D, in allergen-induced airway inflammation. Immunobiology 212:417–425
Wang JY, Kishore U, Lim BL et al (1996) Interaction of human lung surfactant proteins A and D with mite (Dermatophagoides pteronyssinus) allergens. Clin Exp Immunol 106:367–373
Wang JY, Shieh CC, You PF et al (1998) Inhibitory effect of pulmonary surfactant proteins A and D on allergen-induced lymphocyte proliferation and histamine release in children with asthma. Am J Respir Crit Care Med 158:510–518
Wang JY, Shieh CC, Yu CK, Lei HY (2001) Allergen-induced bronchial inflammation is associated with decreased levels of surfactant proteins A and D in a murine model of asthma. Clin Exp Allergy 31:652–662
Wang SX, Liu P, Wei MT et al (2007) Roles of serum clara cell protein 16 and surfactant protein-D in the early diagnosis and progression of silicosis. J Occup Environ Med 49:834–839
Weber B, Borkhardt A, Stoll-Becker S et al (2000) Polymorphisms of surfactant protein A genes and the risk of bronchopulmonary dysplasia in preterm infants. Turk J Pediatr 42:181–185
Wert SE, Yoshida M, LeVine AM et al (2000) Increased metalloproteinase activity, oxidant production, and emphysema in surfactant protein D gene-inactivated mice. Proc Natl Acad Sci USA 97:5972–5977
White MR, Crouch E, Chang D et al (2000) Enhanced antiviral and opsonic activity of a human mannose-binding lectin and surfactant protein D chimera. J Immunol 165:2108–2115
Woodworth BA, Wood R, Baatz JE et al (2007) Sinonasal surfactant protein A1, A2, and D gene expression in cystic fibrosis: a preliminary report. Otolaryngol Head Neck Surg 137:34–38
Wootten CT, Labadie RF, Chen A, Lane KF (2006) Differential expression of surfactant protein A in the nasal mucosa of patients with allergy symptoms. Arch Otolaryngol Head Neck Surg 132:1001–1007
Wright JR (2005) Immunoregulatory functions of surfactant proteins. Nat Rev Immunol 5:58–69
Wright JR, Zlogar DF, Taylor JC et al (1999) Effects of endotoxin on surfactant protein A and D stimulation of NO production by alveolar macrophages. Am J Physiol 276:L650–L658
Wuenschell CW, Zhao J, Tefft JD et al (1998) Nicotine stimulates branching and expression of SP-A and SP-C mRNAs in embryonic mouse lung culture. Am J Physiol 274:L165–L170
Xie JG, Xu YJ, Zhang ZX et al (2005) Surfactant protein A gene polymorphisms in chronic obstructive pulmonary disease. Zhonghua Yi Xue Yi Chuan Xue Za Zhi 22:91–93, Article in Chinese
Yanaba K, Hasegawa M, Takehara K, Sato S (2004) Comparative study of serum surfactant protein-D and KL-6 concentrations in patients with systemic sclerosis as markers for monitoring the activity of pulmonary fibrosis. J Rheumatol 31:1112–1120
Yang S, Panoskaltsis-Mortari A, Ingbar DH et al (2000) Cyclophosphamide prevents systemic keratinocyte growth factor-induced up-regulation of surfactant protein A after allogeneic transplant in mice. Am J Respir Crit Care Med 162:1884–1890
Yang S, Milla C, Panoskaltsis-Mortari A et al (2002) Surfactant protein A decreases lung injury and mortality after murine marrow transplantation. Am J Respir Cell Mol Biol 27:297–305
Yogalingam G, Doyle IR, Power JH (1996) Expression and distribution of surfactant proteins and lysozyme after prolonged hyperpnea. Am J Physiol 270:L320–L330
Yong SJ, Vuk-Pavlovic Z, Standing JE et al (2003) Surfactant protein D-mediated aggregation of Pneumocystis carinii impairs phagocytosis by alveolar macrophages. Infect Immun 71:1662–1671
Yoshida M, Whitsett JA (2006) Alveolar macrophages and emphysema in surfactant protein-D-deficient mice. Respirology 11(Suppl):S37–S40
Yoshida M, Korfhagen TR, Whitsett JA (2001) Surfactant protein D regulates NF-kB and matrix metalloproteinase production in alveolar macrophages via oxidant-sensitive pathways. J Immunol 166:7514–7519
Yurdakök M (2004) Inherited disorders of neonatal lung diseases. Turk J Pediatr 46:105–114
Zamecnik J, Kodet R (2002) Value of thyroid transcription factor-1 and surfactant apoprotein A in the differential diagnosis of pulmonary carcinomas: a study of 109 cases. Virchows Arch 440: 353–61
Zhai L, Wu HM, Wei KL et al (2008) Genetic polymorphism of surfactant protein A in neonatal respiratory distress syndrome. Zhongguo Dang Dai Er Ke Za Zhi 10:295–298, Article in Chinese
Zhang L, Ikegami M, Dey CR et al (2002) Reversibility of pulmonary abnormalities by conditional replacement of surfactant protein D (SP-D) in vivo. J Biol Chem 277:38709–38713
Zhang F, Pao W, Umphress SM et al (2003) Serum levels of surfactant protein D are increased in mice with lung tumors. Cancer Res 63:5889–5894
Zhao J, Yeong LH, Wong WS (2007) Dexamethasone alters bronchoalveolar lavage fluid proteome in a mouse asthma model. Int Arch Allergy Immunol 142:219–229
Zhu BL, Ishida K, Quan L et al (2001) Immunohistochemistry of pulmonary surfactant-associated protein A in acute respiratory distress syndrome. Leg Med (Tokyo) 3:134–140
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2012 Springer-Verlag Wien
About this chapter
Cite this chapter
Gupta, A. (2012). Pulmonary Collectins in Diagnosis and Prevention of Lung Diseases. In: Animal Lectins: Form, Function and Clinical Applications. Springer, Vienna. https://doi.org/10.1007/978-3-7091-1065-2_43
Download citation
DOI: https://doi.org/10.1007/978-3-7091-1065-2_43
Published:
Publisher Name: Springer, Vienna
Print ISBN: 978-3-7091-1064-5
Online ISBN: 978-3-7091-1065-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)